Liniae nigra
Reading File
Finding Sources
Searching Images
linea nigra pregnancy abdomen
Reading File
Reading File
Loading Image
Reading File
Linea Nigra
Linea nigra (Latin: "black line") is the hyperpigmentation of the linea alba — the normally pale, avascular fibrous structure running vertically along the midline of the anterior abdominal wall from the pubic symphysis to the xiphoid process of the sternum.

Linea nigra extending from the pubic symphysis toward the xiphoid process; pigmentation is typically more pronounced inferior to the umbilicus.
Pathophysiology
Hyperpigmentation develops due to increased circulating levels of:
- Melanocyte-stimulating hormone (MSH) — particularly β-MSH and α-MSH
- Estrogen and progesterone — stimulate melanocytes in the epidermis
- Placental lipids — can stimulate tyrosinase activity, further increasing melanin synthesis
- β-endorphin also plays a contributory role
These hormonal shifts drive melanocyte activation across multiple skin sites, with linea nigra being the midline abdominal manifestation.
Clinical Features
| Feature | Detail |
|---|---|
| Location | Midline of abdomen, pubic symphysis → xiphoid process |
| Appearance | Linear hyperpigmented band (tan to dark brown) |
| Asymmetry | More pronounced inferior to the umbilicus |
| Timing | Develops during pregnancy |
| Occurrence | Part of a broader pattern of pregnancy hyperpigmentation affecting ≥90% of pregnant women |
Other areas commonly hyperpigmented in pregnancy include the areolae, axillae, genitalia, and neck. Linea nigra is part of the same physiologic process.
Course and Prognosis
Linea nigra is typically reversible — it regresses after delivery in most women. It is considered a physiologic change, not a pathologic one, and requires no treatment.
Differential Diagnosis
It must be distinguished from:
- Pigmentary demarcation lines (Voigt/Futcher lines) — obliquely oriented lines on the limbs, not midline
- Acanthosis nigricans — if the neck/axillae also become velvety or papillomatous, consider an underlying endocrinopathy (e.g., diabetes mellitus)
Context: Pregnancy Dermatology
Linea nigra is one of the most visible physiologic skin changes of pregnancy, alongside:
- Melasma (chloasma) — blotchy facial hyperpigmentation (~70% of pregnancies)
- Striae gravidarum — stretch marks on abdomen, hips, and breasts
- Spider angiomas — most common vascular change
- Palmar erythema
— Fitzpatrick's Dermatology, Vol. 1–2, Chapter 105 | Creasy & Resnik's Maternal-Fetal Medicine
Explain the procedure of palpation in gastrointestinal system examination
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
abdominal palpation technique gastrointestinal examination
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive information to compose a thorough answer. Here it is:
Palpation in Gastrointestinal System Examination
Palpation is the third step in the abdominal examination sequence — following inspection and auscultation/percussion — and is the most informative component of the physical examination.
Patient Preparation
Before beginning palpation:
- Patient lies supine with arms at the sides
- Ask the patient to bend the knees and place the soles of feet flat on the bed — this relaxes the abdominal musculature and reduces voluntary guarding, allowing more accurate assessment
- Warm hands before contact to prevent reflex tensing
- Expose the abdomen from the xiphoid process to the inguinal ligaments
- Ask the patient to identify their area of most pain — begin palpation farthest from that point to gain cooperation and establish a baseline
Sequence of Palpation
1. Light (Superficial) Palpation
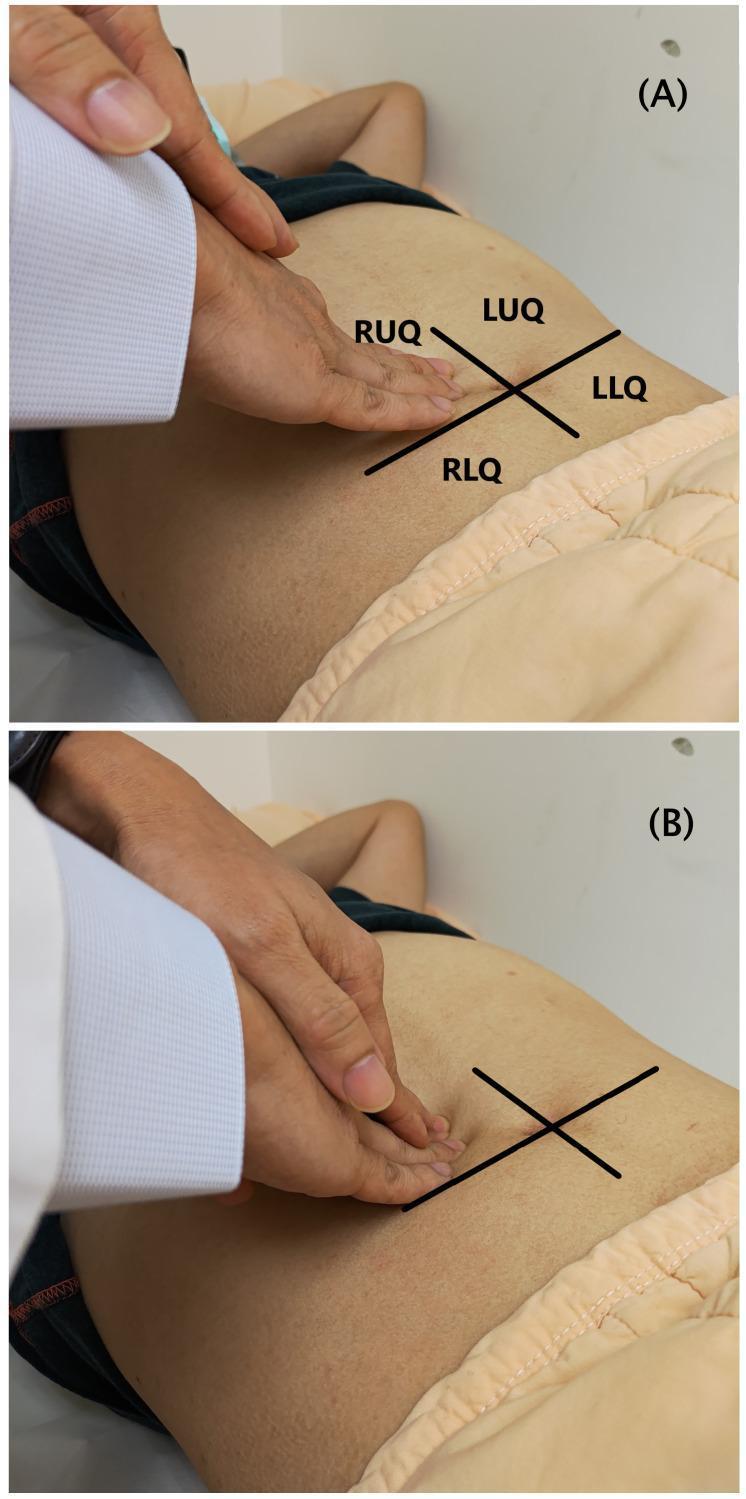
(A) Light palpation — flat hand, gentle pressure; (B) Deep palpation — flexed fingers, greater depression of the abdominal wall
- Use the pads of the fingers with the hand held relatively flat
- Apply gentle, uniform pressure (~1–2 cm depth) across all quadrants
- Move systematically through all four quadrants: RUQ → LUQ → LLQ → RLQ (or clockwise), ending at the area of pain
- Purpose: detect muscle resistance (guarding), superficial tenderness, and superficial masses of the abdominal wall — hernias, subcutaneous lipomas, lymph nodes, hematomas, abscesses
Involuntary guarding (reflex muscle spasm that persists despite relaxation maneuvers) suggests underlying peritoneal irritation. Distinguish from voluntary guarding (patient tensing due to anxiety or anticipated pain).
2. Deep Palpation
- Apply greater pressure (4–5 cm or more), using flexed fingers or the bimanual technique (one hand on top of the other)
- Systematic coverage of all quadrants
- Purpose: assess the deeper abdominal organs and detect deep masses
Superficial or deep masses should be assessed for:
- Size and location
- Mobility (mobile vs. fixed)
- Content (solid, cystic/fluid-filled, or air-containing)
- Tenderness
Deep masses include: neoplasms (liver, gallbladder, pancreas, stomach, colon, kidney), abscesses (appendiceal, diverticular, Crohn-related), and aortic aneurysms (pulsatile, midline, expansile).
Organ-Specific Palpation
Liver (Right Upper Quadrant)
- Begin palpation below the anticipated liver edge (right iliac fossa level), moving upward
- Ask the patient to take a deep breath — the descending diaphragm pushes the liver edge into the examiner's fingers
- Assess: size (below costal margin), contour (smooth vs. irregular/nodular), texture (soft vs. firm/hard), and tenderness
- Percussion demarcates the upper border; a span >12 cm in the midclavicular line suggests hepatomegaly
Spleen (Left Upper Quadrant)
- The tip of an enlarged spleen is palpated during inspiration
- Support the left costal margin with the left hand (providing counterpressure from behind), while palpating below the left costal margin with the right hand
- Alternative: hook fingers lightly under the left lower rib cage while standing cephalad to the patient
- A normal-sized spleen is not palpable; palpability implies significant enlargement
Kidneys
- Use bimanual ballottement: one hand in the flank posteriorly, one anteriorly
- Normal kidneys are generally not palpable except in thin individuals; the right kidney descends more and may be felt on deep inspiration
Aorta
- Palpate in the epigastrium, slightly left of midline
- Note width — >3 cm suggests an abdominal aortic aneurysm (pulsatile, expansile)
Special Signs Elicited on Palpation
| Sign | Technique | Clinical Significance |
|---|---|---|
| Rebound tenderness (Blumberg sign) | Slowly apply deep pressure, then rapidly release — pain on release > pain on application | Peritoneal irritation / peritonitis |
| Involuntary guarding | Persistent muscle rigidity despite relaxation maneuvers | Peritonitis |
| Board-like rigidity | Abdomen hard as a board throughout | Perforated viscus / severe peritonitis |
| Murphy's sign | Palpate RUQ below costal margin; ask patient to inspire deeply — involuntary arrest of inspiration due to pain | Acute cholecystitis |
| Rovsing's sign | Palpate LLQ → pain referred to RLQ | Acute appendicitis |
| Iliopsoas sign | Extend the right leg against resistance → pain | Retrocecal appendicitis |
| Obturator sign | Passive internal rotation of flexed right hip → pain | Pelvic appendicitis / pelvic abscess |
| Carnett's sign | Pain increases when abdominal wall muscles are tensed | Pain is from abdominal wall, not visceral |
Pain out of proportion to examination — severe pain but minimal tenderness on palpation — is a red flag for mesenteric ischemia rather than perforation.
Assessing for Ascites
When a protuberant abdomen with bulging flanks is present:
- Shifting dullness: percuss flanks in the supine position to find the dullness-tympany transition; then ask the patient to roll to one side and re-percuss — dullness shifts with gravity if ascites is present (most sensitive bedside test)
- Fluid thrill: tap one flank sharply while the assistant places a hand on the midline; a transmitted fluid wave is felt on the opposite flank
Key Practical Points
- Always palpate the area of maximum pain last
- Overly vigorous palpation of a very tender abdomen may cause such distress that the patient cannot cooperate for the rest of the examination
- Rebound tenderness may not need to be formally tested if the patient winces during percussion or when the bed is jarred — percussion-induced peritonism is equivalent
- Palpation findings in the elderly, immunocompromised, or intoxicated patient may be markedly attenuated despite significant pathology
- Serial palpation by the same examiner over time is invaluable — evolution of signs (improvement or progression) guides surgical decision-making
— Goldman-Cecil Medicine, Chapter on Abdominal Examination | Sleisenger & Fordtran's Gastrointestinal and Liver Disease | Sabiston Textbook of Surgery, Chapter 85
This is a shared conversation. Sign in to Orris to start your own chat.