Safe and unsafe CSOM in detail for ms ent pg exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have all the key information needed. Now I'll compile a comprehensive, exam-focused answer on Safe and Unsafe CSOM.
CSOM: Safe vs Unsafe - Complete Guide for MS ENT PG Exam
Source: Cummings Otolaryngology Head and Neck Surgery
Overview / Classification
CSOM is classically divided into two types based on the presence or absence of cholesteatoma:
| Feature | Safe CSOM (Tubotympanic / Mucosal) | Unsafe CSOM (Atticoantral / Squamosal) |
|---|---|---|
| Also called | Tubotympanic disease, mucosal disease | Atticoantral disease, squamosal disease |
| Defining feature | Chronic TM perforation without cholesteatoma | With cholesteatoma (or dangerous granulation tissue) |
| Perforation site | Central (pars tensa) | Marginal / attic (pars flaccida), posterosuperior |
| Discharge | Mucoid, profuse, not malodorous | Scanty, purulent, foul-smelling (anaerobes) |
| Bone erosion | Absent or minimal | Present - hallmark of the disease |
| Risk of complications | Low | High |
| Treatment | Medical + myringoplasty/tympanoplasty | Surgery (mastoidectomy) - mandatory |
SAFE CSOM (Tubotympanic Disease / CSOM without Cholesteatoma)
Pathogenesis
Acute or recurrent AOM leads to a permanent perforation of the tympanic membrane. The factors that cause acute middle ear infection to become chronic are not fully understood. Key pathological findings in temporal bones with chronic perforated TM include:
- Granulation tissue: 97.4%
- Ossicular changes: 90.5%
- Tympanosclerosis: 19.8%
- Cholesterol granuloma: 12.1%
- Cholesteatoma: 4.3% (only when already perforated)
Aeration of the middle ear and mastoid depends on gas passage around the ossicles in the epitympanic space into the antrum via only two constant openings: between the tensor tympani tendon and stapes, and between the short process of incus and the stapedial tendon. Edema and granulation tissue obstructing these narrow passages leads to irreversible mucosal and bony changes.
Clinical Features
- Discharge: Profuse, mucoid, non-foul-smelling (unless secondarily infected)
- Perforation: Central, involving the pars tensa - safe because it does not involve the annulus
- Hearing loss: Predominantly low-frequency conductive hearing loss; a small perforation affects low frequencies, a large one affects both low and high
- Tympanosclerosis: White chalky plaques from collagen destruction and dystrophic calcification
- No signs of bone erosion
- No cholesteatoma
Otoscopic appearance:
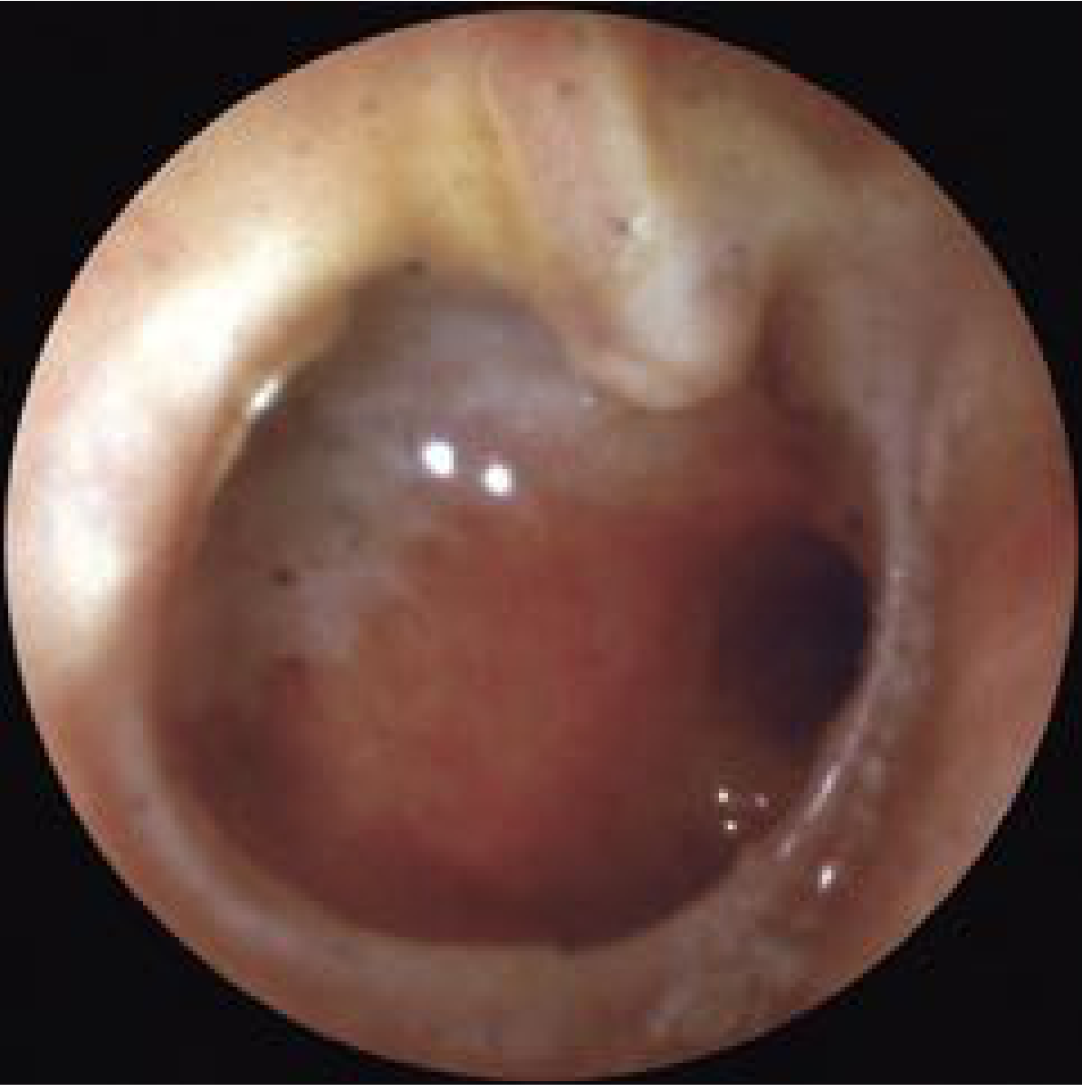 Fig: Tympanic membrane perforation with chronic inflammation (safe CSOM)
Fig: Tympanic membrane perforation with chronic inflammation (safe CSOM)
Bacteriology
- Predominantly Gram-negative aerobes: Pseudomonas aeruginosa, Proteus, E. coli
- Staphylococcus aureus (common in exacerbations)
- Anaerobes less common than in cholesteatoma
Management
Medical (conservative):
- Aural toilet - dry mopping or suction clearance
- Topical antibiotic drops (fluoroquinolones - ciprofloxacin most commonly used)
- Systemic antibiotics during acute exacerbations
- Water precautions (avoid water entry)
- Treat underlying nasal/nasopharyngeal pathology (adenoids, rhinosinusitis)
Surgical:
- Myringoplasty: Repair of TM perforation alone (no ossicular work)
- Tympanoplasty: TM repair with ossicular chain reconstruction if needed
- Pre-requisite: The ear should be dry for at least 6-8 weeks before surgery
- Aim: Restore hearing, prevent recurrent infections, prevent progression to unsafe disease
UNSAFE CSOM (Atticoantral Disease / CSOM with Cholesteatoma)
What is Cholesteatoma?
Cholesteatomas are epidermal inclusions of the middle ear or mastoid - cystic structures or keratinizing epithelium within the middle ear cleft. They contain desquamated debris (principally keratin). The term was coined by Johannes Müller in 1838 because the white-yellow keratin flakes grossly resemble cholesterol crystals. Cruveilhier first described it as a "pearly tumor" of the temporal bone.
Types
1. Congenital Cholesteatoma
- Originates from areas of keratinizing epithelium within the middle ear cleft
- No antecedent history of otitis
- Michaels found epidermoid formation in 37/68 fetal temporal bones (10-33 weeks gestation)
- Staging (Potsic):
- Stage I: Limited to one quadrant
- Stage II: Multiple quadrants, no ossicular involvement
- Stage III: Ossicular involvement, no mastoid extension
- Stage IV: Mastoid involvement (67% risk of residual disease post-surgery)
2. Acquired Cholesteatoma
- Primary acquired: Arises from pars flaccida retraction pocket (invagination theory)
- Secondary acquired: Keratinizing epithelium migrates through a marginal TM perforation
Theories of Pathogenesis of Acquired Cholesteatoma (4 theories)
-
Invagination Theory (Retraction Pocket Theory) - Most widely accepted
- Eustachian tube dysfunction → negative middle ear pressure (ex vacuo) → retraction of pars flaccida (less fibrous, less resistant)
- As the pocket deepens, desquamated keratin cannot self-clear → cholesteatoma
- Results in attic retraction pocket / posterosuperior defect
-
Basal Cell Hyperplasia Theory
- Basal cells of the TM proliferate and invade the middle ear
- Chronic inflammation stimulates abnormal proliferation
-
Epithelial Migration (Invasion) Theory
- Keratinizing squamous epithelium from the ear canal surface migrates through a marginal TM perforation into the middle ear (secondary acquired cholesteatoma)
-
Squamous Metaplasia Theory
- Middle ear cuboidal/columnar epithelium undergoes squamous metaplasia under chronic inflammatory stimulus
Sudhoff and Tos proposed a combination of invagination and basal cell theories for retraction pocket cholesteatoma. Jackler and colleagues recently proposed the mucosal traction theory.
Clinical Features
- Discharge: Scanty, foul-smelling (malodorous) - due to infection with anaerobic bacteria
- Perforation: Marginal or attic (pars flaccida) - UNSAFE because it involves the annulus, allowing epithelial ingrowth
- Hearing loss: Conductive (initially), may become mixed or sensorineural if labyrinthine fistula develops
- Signs of bone erosion:
- Scutum erosion (attic wall erosion) - earliest sign
- Ossicular erosion (incus long process most common)
- Canal wall erosion
- White/pearly mass visible in the attic or posterosuperior quadrant
Otoscopic appearance:
 Fig: Primary acquired cholesteatoma in the pars flaccida region with scutum erosion (unsafe CSOM)
Fig: Primary acquired cholesteatoma in the pars flaccida region with scutum erosion (unsafe CSOM)
Mechanism of Bone Erosion
Cholesteatoma causes bone erosion by:
- Enzymatic destruction: Matrix metalloproteinases (MMPs 1, 2, 3, 9) in basal and suprabasal cell layers; neutral collagenase degrades osteoid surface
- Osteoclast activation: RANKL on osteoblasts/T-cells binds to RANK on monocytes → osteoclast formation; pro-inflammatory cytokines (IL-1, LPS from bacteria) potentiate this
- Pressure: Physical pressure with or without inflammation is sufficient to induce bone resorption experimentally
- Most common site: Incus (long process) → conductive hearing loss
Bacteriology of Infected Cholesteatoma
| Organism | % of cultures |
|---|---|
| Pseudomonas aeruginosa | 31.1% |
| Staphylococcus aureus | 19.1% |
| Proteus mirabilis | 7.7% |
| Peptococcus (anaerobe) | 12.4% |
| Bacteroides sp. (anaerobe) | 12.4% |
| Peptostreptococcus | 4.8% |
| Clostridium sp. | 3.8% |
| Fusobacterium sp. | 2.9% |
Both aerobes and anaerobes present - explains the malodorous discharge.
Complications of CSOM
Extracranial Complications
- Acute mastoiditis → Coalescent mastoiditis
- Subperiosteal (postauricular) abscess
- Bezold abscess (tracking along sternocleidomastoid)
- Temporal abscess
- Labyrinthine fistula (most common site: lateral/horizontal semicircular canal) → vertigo + sensorineural hearing loss
- Facial nerve paralysis (acute from infection, or insidious from cholesteatoma expanding into fallopian canal)
- Petrous apicitis (Gradenigo syndrome: deep facial pain, abducens palsy, otorrhea)
- Encephalocele / CSF leakage (through eroded tegmen)
Intracranial Complications
- Meningitis (most common intracranial complication)
- Brain abscess (temporal lobe most common from otogenic source)
- Subdural empyema
- Epidural abscess
- Lateral sinus thrombosis (sigmoid sinus)
- Otitic hydrocephalus
Note: Extracranial complications are more common in children (0-5 years); intracranial complications are more common in young adults (21-30 years).
Surgical Management of Unsafe CSOM
Surgery is mandatory. Key surgical approaches:
Canal Wall-Up (CWU) / Intact Canal Wall Mastoidectomy
| Advantages | Disadvantages |
|---|---|
| Physiologic TM position | Residual and recurrent cholesteatoma may occur |
| Adequate middle ear space | Incomplete exteriorization of facial recess |
| No mastoid cavity problem | Second-look (second-stage) operation often required |
Canal Wall-Down (CWD) / Radical / Modified Radical Mastoidectomy
| Advantages | Disadvantages |
|---|---|
| Residual cholesteatoma easily found on follow-up | Mastoid cavity problems (infected bowl) |
| Recurrent cholesteatoma is rare | Requires lifelong periodic cavity cleanings |
| Total exteriorization of facial recess | Shallow middle ear - difficult to reconstruct |
Bondy's operation: Modified radical mastoidectomy for attic cholesteatoma with intact ossicular chain - removes only the attic/mastoid portion, preserving the mesotympanum.
Factors Determining Surgical Choice
- Extent of disease
- Presence of complications
- Hearing status of both ears
- Eustachian tube function
- Mastoid pneumatization
- Patient factors: age, comorbidities, reliability for follow-up
- Surgeon's skill
Conservative (Non-surgical) Role in Unsafe CSOM
Only in very limited situations:
- Patient medically unfit for surgery
- Only hearing ear where surgical risk outweighs benefit
- Irrigation with 2% acetic acid in 20% isopropyl alcohol can keep some cholesteatomas stable if the opening into the ear canal is sufficiently large
- Always monitor closely - if disease progresses, surgery is indicated
Quick Exam Comparison Table
| Feature | Safe CSOM | Unsafe CSOM |
|---|---|---|
| Synonym | Tubotympanic / Mucosal | Atticoantral / Squamosal |
| Pathology | Mucosal disease | Cholesteatoma |
| TM perforation | Central (pars tensa) | Marginal / Attic (pars flaccida) |
| Discharge | Profuse, mucoid, non-foul | Scanty, purulent, foul-smelling |
| Bone erosion | No | Yes (scutum, ossicles, lateral SCC) |
| Hearing loss | Conductive (low freq) | Conductive → mixed/SNHL |
| Complications | Rare | Common, serious |
| Treatment | Medical → Myringoplasty | Mastoidectomy (mandatory) |
| Prognosis | Good | Guarded |
| Urgency | Elective surgery | Semi-urgent/urgent surgery |
High-Yield Exam Points
- "Safe" does NOT mean no surgery - it means surgery is elective, not urgent
- Attic perforation = UNSAFE until proven otherwise; marginal perforation implies risk of cholesteatoma
- Foul smell = anaerobes = cholesteatoma - the most specific clinical indicator
- Incus long process is the most commonly eroded ossicle in CSOM with cholesteatoma
- Horizontal semicircular canal is the most common site of labyrinthine fistula
- Scutum erosion on X-ray (Schuller's view) or CT is a hallmark of atticoantral disease
- Squamous epithelium does not belong in the middle ear - any keratin/white mass in middle ear = cholesteatoma
- MMPs + osteoclasts = mechanism of bone erosion
- Bezold abscess - passes through the tip of mastoid along the SCM - the pus tracks under the muscle
- Gradenigo triad (petrous apicitis): otorrhea + retro-orbital pain (V1 irritation) + diplopia (CN VI palsy/Dorello canal compression)
Source: Cummings Otolaryngology Head and Neck Surgery (Cummings ENT), Chapters 140-141
This is a shared conversation. Sign in to Orris to start your own chat.