Pagets disease
Reading File
Finding Sources
Searching PubMed
"Paget disease" bone
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Here is a complete overview of Paget's Disease of Bone drawn from Harrison's Principles of Internal Medicine (22E), Goldman-Cecil Medicine, Firestein & Kelley's Rheumatology, and Katzung's Pharmacology.
Paget's Disease of Bone
Definition
Paget's disease is a localized bone-remodeling disorder affecting widespread, non-contiguous areas of the skeleton. The core pathology is overactive osteoclastic resorption followed by compensatory but disorganized osteoblastic bone formation, producing a structurally weak mosaic of woven and lamellar bone. The affected bone is expanded, less compact, and hypervascular.
- Harrison's Principles of Internal Medicine 22E
Epidemiology
- Prevalence ~0.5-3% in populations over 40-55 years of age; autopsy series show ~3% over age 40
- More common in males; prevalence rises sharply with age
- High prevalence in Western Europe (UK, France, Germany) and among people of European descent who migrated to Australia, New Zealand, South Africa, and the Americas
- Rare in native populations of the Americas, Africa, Asia, and the Middle East
- For unclear reasons, prevalence and severity have been decreasing over recent decades, and age at diagnosis is increasing
Etiology
Both genetic and viral factors are implicated:
Genetic:
- Positive family history in 15-25% of patients; raises risk 7-10-fold in first-degree relatives
- Autosomal dominant pattern with variable penetrance in familial cases
- Key genetic associations:
- TNFRSF11B (OPG gene) homozygous deletion → juvenile Paget's (familial idiopathic hyperphosphatasia) - uncontrolled osteoclastic resorption
- TNFRSF11A (RANK gene) mutations → familial expansile osteolysis, expansile skeletal hyperphosphatasia
- Profilin 1 mutations → early-onset Paget's with predisposition to osteosarcoma
- Valosin-containing protein mutations → inclusion body myopathy with Paget's disease and frontotemporal dementia
Viral:
- Cytoplasmic and nuclear inclusions resembling paramyxoviruses (measles, RSV, canine distemper virus) found in pagetic osteoclasts
- Measles virus nucleocapsid/matrix gene vectors can convert osteoclast precursors into pagetic-like osteoclasts
- The decline in Paget's disease incidence coincides with widespread measles vaccination
- However, no live virus has been cultured from pagetic bone, and full-length viral genes have not been cloned from patients
Pathophysiology
The principal abnormality is increased number and activity of osteoclasts:
- Pagetic osteoclasts are 10-100 times more numerous, much larger, and have up to 100 nuclei (vs 3-5 in normal osteoclasts)
- Create a sevenfold increase in resorptive surfaces; erosion rate of 9 μg/day (normal 1 μg/day)
- Mechanisms driving hyperactive osteoclasts:
- Hypersensitivity to 1,25(OH)₂D₃
- Hyperresponsiveness to RANKL (osteoclast stimulatory factor)
- Increased RANKL expression by marrow stromal cells in pagetic lesions
- Elevated IL-6 (overexpressed in pagetic osteoclasts and elevated in blood)
- Upregulation of proto-oncogene c-fos (increases osteoclastic activity)
- Overexpression of antiapoptotic oncogene Bcl-2 in pagetic bone
Bone mass is normal or increased (not reduced) unless there is concomitant calcium/vitamin D deficiency.
Three Phases of Paget's Disease
| Phase | Description | Radiographic Sign |
|---|---|---|
| Lytic (hot) | Prominent osteoclastic resorption + hypervascularization | Advancing lytic wedge, "blade of grass" lesion |
| Mixed (lytic + blastic) | Active resorption and formation; woven bone replaces lamellar; fibrous tissue may replace marrow | Combined sclerosis and lysis |
| Sclerotic ("burned-out") | Resorption declines; hard, dense, avascular pagetic/mosaic bone | Dense sclerosis |
All three phases can be present simultaneously at different skeletal sites.
Clinical Manifestations
Most patients are asymptomatic - often detected incidentally by elevated alkaline phosphatase or radiographic abnormality.
Common sites: pelvis, vertebral bodies, skull, femur, tibia
Symptoms when present:
- Bone pain - the most common symptom; arises from increased vascularity, expanding lytic lesions, fractures, or bowing
- Skeletal deformities - bowing of femur/tibia, enlarged skull with frontal bossing, short stature with simian posturing
- Secondary osteoarthritis - at joints adjacent to pagetic bone
- Fractures - in 10-30% of patients; most common at femoral shaft and subtrochanteric regions; "banana fractures" - short fissure fractures traversing the cortex
- Neurological complications - from bone expansion compressing neural tissue: hearing loss (most common; due to cochlear or auditory nerve compression), cranial nerve palsies, spinal cord/nerve root compression, basilar invagination causing brainstem or cerebellar signs
- Cardiovascular complications - in patients with >15-35% skeletal involvement; extensive arteriovenous shunting through hypervascular pagetic bone leads to high-output state and cardiac enlargement; high-output heart failure is rare and usually requires coexisting cardiac pathology; calcific aortic stenosis and diffuse vascular calcifications also associated
- Sarcomatous transformation - rare, <0.5-1% of patients; mostly osteosarcoma; presents as new pain in a long-standing pagetic lesion; incidence appears to be decreasing with effective treatment
- Osteoclast-rich benign giant cell tumors may arise adjacent to pagetic bone; respond to glucocorticoids
- Hypercalcemia - rarely from immobilization; hypercalcemia even with immobilization warrants a search for another cause
Diagnosis
Clinical examination findings
- Enlarged skull with frontal bossing
- Bowing of extremities; leg-length discrepancy
- Warmth and tenderness over a bone
- Simian posturing (short stature, bowed legs)
Radiographic features
- Enlargement or expansion of the entire bone or a segment of a long bone
- Cortical thickening; coarsening of trabecular markings
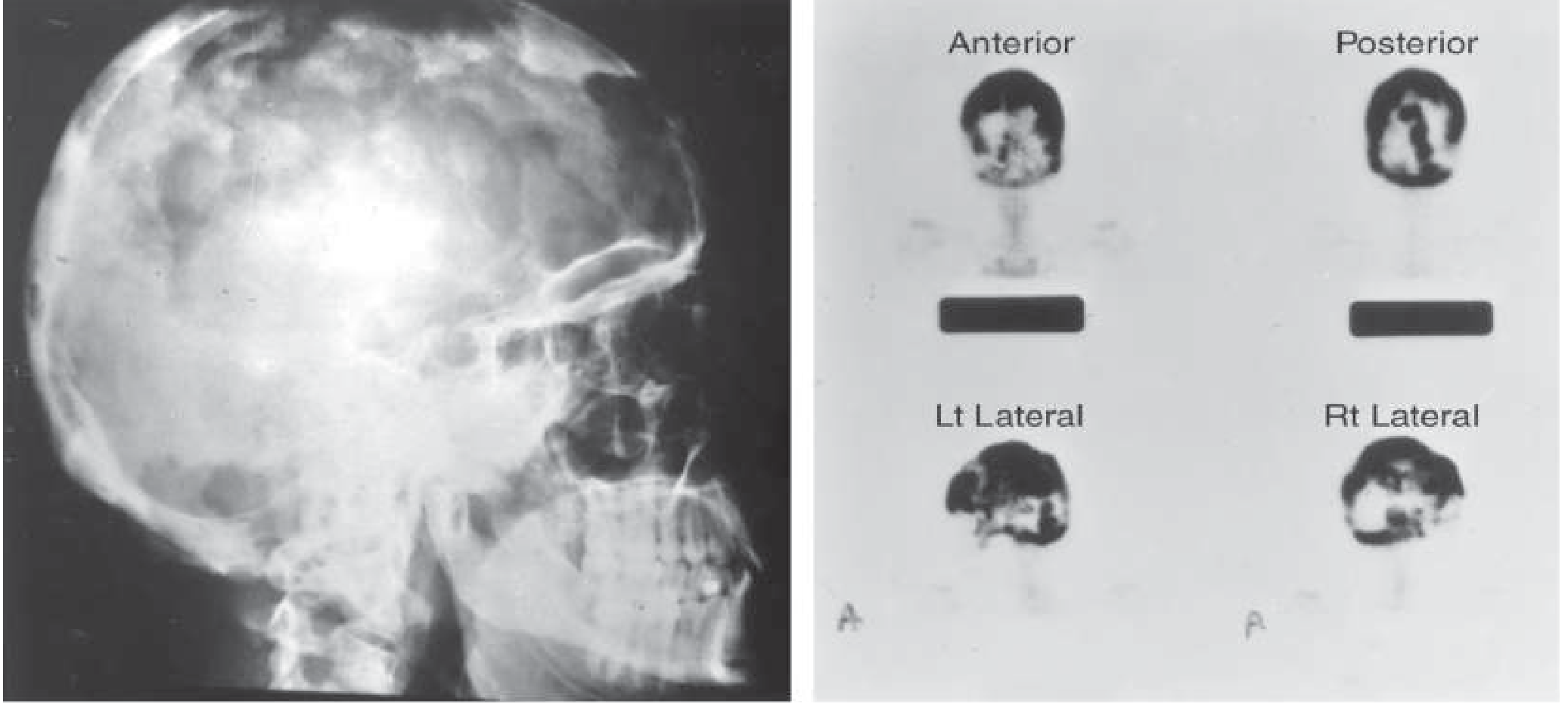
- Skull: "cotton wool" appearance, osteoporosis circumscripta, thickening of diploic areas
- Vertebrae: cortical thickening of endplates → "picture frame" vertebra; diffuse sclerosis → "ivory vertebra"
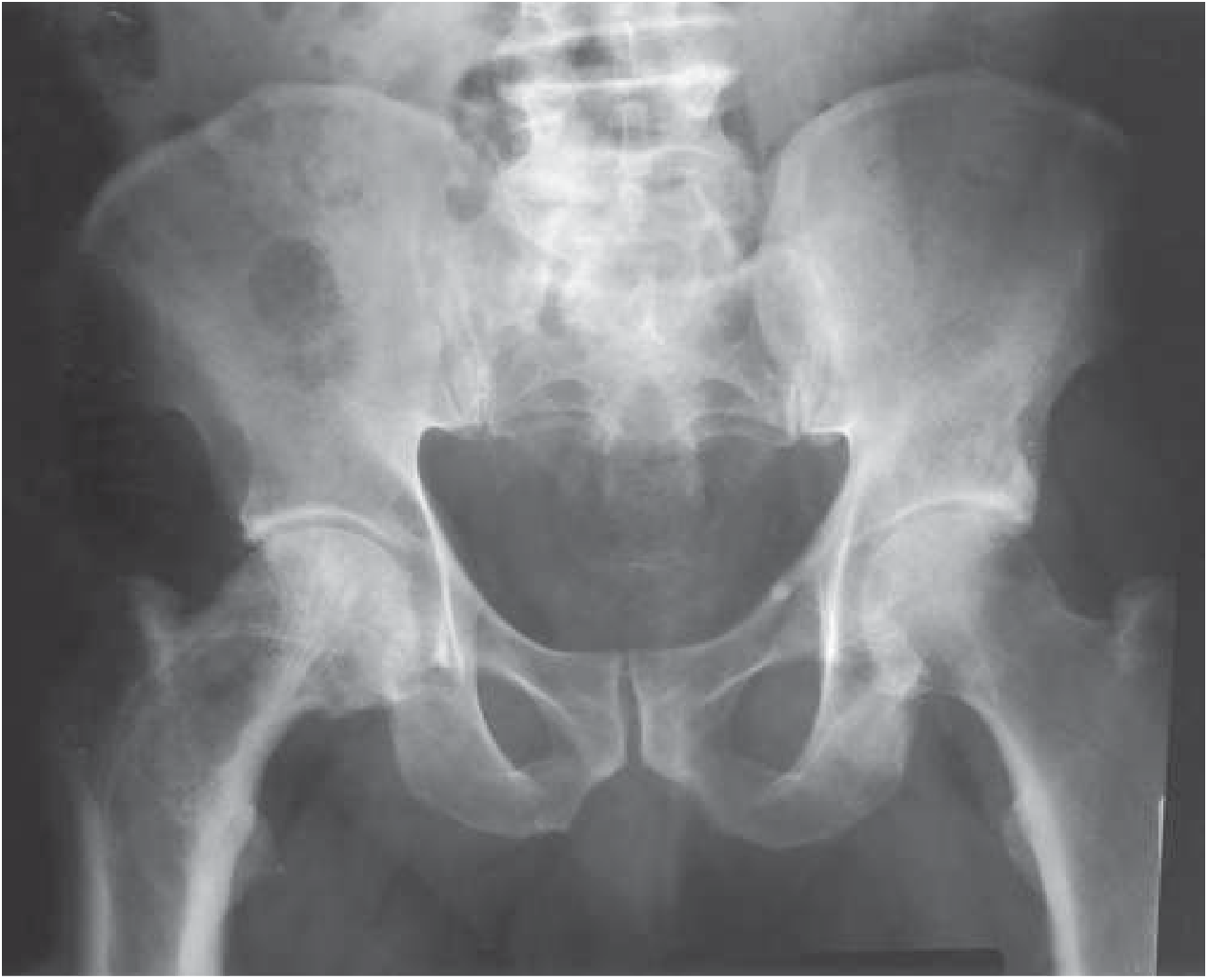
- Pelvis: thickened iliopectineal line (brim sign), protrusio acetabuli, whorls of coarse trabeculation
- Long bones: bowing deformity, "blade of grass" lytic front
Imaging
- ⁹⁹mTc bone scan - most sensitive for identifying active skeletal lesions (but less specific)
- CT - useful for fracture assessment
- MRI - needed when sarcoma, giant cell tumor, or metastatic disease is suspected
- Bone biopsy - required for definitive diagnosis of malignancy
Biochemical markers
- Serum total alkaline phosphatase (ALP) - the test of choice for both diagnosis and monitoring therapy; reflects extent and severity; can be elevated up to 10x normal in active disease
- Bone-specific ALP - useful when total ALP is normal but a single site is progressing symptomatically
- PINP (procollagen type I N-terminal propeptide) - reflects disease activity; a useful bone formation marker
- Serum osteocalcin - not reliably elevated; NOT recommended for diagnosis or management
- Urinary hydroxyproline - elevated (marker of bone resorption); useful for monitoring
- Serum calcium and phosphate are normal in Paget's disease
- Mild secondary hyperparathyroidism may develop during bisphosphonate therapy if calcium/vitamin D intake is insufficient
Treatment
Per Endocrine Society Clinical Practice Guidelines (2014), pharmacologic therapy is indicated for most patients with active Paget's disease at risk for complications.
Indications for treatment
- Bone pain or headache from metabolically active disease
- Fracture prevention in active lytic lesions of weight-bearing bones
- To decrease local blood flow before elective bone surgery (reduces operative blood loss)
- To prevent progression of neurologic complications
- Correction of hypercalcemia from immobilization
Bisphosphonates (first-line)
| Drug | Dose | ALP Normalization |
|---|---|---|
| Zoledronic acid (preferred) | 5 mg IV over 15 min | ~90% at 6 months |
| Pamidronate | 30 mg/day IV over 4h × 3 days | ~50% |
| Risedronate | 30 mg/day orally × 2 months | ~70-80% |
| Alendronate | 40 mg/day orally × 6 months | ~50-60% |
| Tiludronate | 400 mg/day orally × 3 months | ~35% |
| Etidronate | 5 mg/kg/day (rarely used now) | Lower efficacy |
- Long-term remissions (months to years) expected in bisphosphonate responders
- Treatment should not exceed 6 months per course but can be repeated after 6 months
- Key toxicity of etidronate: osteomalacia and increased fractures at doses above 5 mg/kg/day
- Key toxicity of alendronate/newer bisphosphonates at Paget doses: gastric irritation (reversible on stopping)
- Adequate calcium and vitamin D intake must be ensured before bisphosphonate therapy to prevent hypocalcemia/secondary hyperparathyroidism
Calcitonin (second-line)
- Subcutaneous/IM: 50-100 MRC units daily or every other day
- Nasal inhalation: 200-400 units/day
- Weeks to months for response (pain relief, ALP reduction)
- Limitation: patients often lose response over time (not correlated with antibody development)
Surgery
- Joint replacement for severe secondary arthritis
- Internal fixation for fractures or impending fractures in weight-bearing bones
- Decompressive surgery for neurological complications
Summary Table
| Feature | Key Point |
|---|---|
| Pathology | Osteoclast-driven bone resorption → disorganized bone formation → mosaic bone |
| Key marker | Serum total ALP (elevated; reflects disease activity) |
| Most common symptom | Bone pain |
| Most common sites | Pelvis > vertebrae > skull > femur > tibia |
| Most feared complication | Osteosarcoma (<1%) |
| Most common neurological complication | Hearing loss |
| First-line treatment | Bisphosphonates (zoledronic acid most effective) |
| Serum Ca/PO₄ | Normal |
Sources: Harrison's Principles of Internal Medicine 22E, pp. 3355-3357; Firestein & Kelley's Textbook of Rheumatology, p. 2250; Katzung's Basic and Clinical Pharmacology 16E, p. 1229; Goldman-Cecil Medicine International Edition
This is a shared conversation. Sign in to Orris to start your own chat.