Clinical Implications for commonly ordered Renal Function tests.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have very comprehensive content from multiple authoritative textbooks. Let me compile the full response.
Clinical Implications of Commonly Ordered Renal Function Tests
Overview: Standard Reference Ranges
| Test | Reference Range | Units |
|---|---|---|
| Blood Urea Nitrogen (BUN) | 5-25 | mg/dL |
| Creatinine | 0.5-1.5 | mg/dL |
| Sodium | 133-147 | mmol/L |
| Potassium | 3.2-5.2 | mmol/L |
| Chloride | 94-110 | mmol/L |
| CO₂ (bicarbonate) | 22-32 | mmol/L |
| Uric acid | 2.5-7.5 | mg/dL |
| Calcium | 8.5-10.5 | mg/dL |
| Phosphorus | 2.2-4.2 | mg/dL |
| Urine pH | 4.5-8.0 | - |
| Urine specific gravity | 1.002-1.030 | - |
(Miller's Anesthesia, 10e - Table 55.2)
1. Glomerular Filtration Rate (GFR)
GFR is the best overall measure of glomerular function, with a normal value of approximately 125 mL/min. Clinical implications at different thresholds:
- GFR >50% of normal: No manifestations of reduced GFR - patient is typically asymptomatic
- GFR reduced to ~30% of normal: Moderate renal insufficiency - biochemical elevations in urea and creatinine, with early symptoms like nocturia, anemia, fatigue, decreased appetite, and calcium/phosphorus abnormalities
- GFR severely reduced: Overt uremia with acidemia, volume overload, and neurologic, cardiac, and respiratory manifestations
- GFR 5-10% of normal: End-stage renal disease (ESRD) - renal replacement therapy required
Intercurrent clinical stressors (sepsis, surgery, nephrotoxins) can push patients with mild-moderate insufficiency into overt uremia.
Estimating GFR
Cockcroft-Gault formula:
CrCl (mL/min) = [(140 - age) × lean body weight (kg)] / [plasma creatinine (mg/dL) × 72]
- Multiply by 0.85 for women (lower muscle mass fraction)
MDRD equation: Validated in adult Caucasian and African American populations with GFR <60 mL/min/1.73 m². Not reliable for GFR >60 or in pregnant women, children, or acutely ill patients. Corrects by 0.742 for female sex and 1.210 for African American race.
CKD-EPI equation: Based on serum creatinine, age, sex, and race. More accurate than MDRD when GFR is high (>60 mL/min/1.73 m²), and more accurately predicts risk of ESRD, cardiovascular mortality, and all-cause mortality. Current preferred method.
2. Serum Creatinine
- Normal: 0.8-1.2 mg/dL in adults; 0.4-0.8 mg/dL in young children; 0.5-1.0 mg/dL in pregnancy
- End product of skeletal muscle creatine metabolism; production is constant
- Freely filtered at the glomerulus, negligible tubular secretion, not reabsorbed
Key clinical implications:
- Serum creatinine does NOT rise significantly until approximately 50% of renal function is lost
- Because of the wide normal range, a 50% increase in serum creatinine - reflecting a 50% drop in GFR - may go unnoticed without baseline values
- Not significantly influenced by dietary intake (unlike BUN), making it more specific for renal dysfunction
- Drug excretion reliant on glomerular filtration may already be significantly impaired at creatinine levels of 1.5-2.0 mg/dL, which may appear "only mildly elevated"
- False elevation (Jaffe reaction method): cephalosporins, ketones, glucose, fructose, protein, urea, and ascorbic acid
3. Blood Urea Nitrogen (BUN)
- Normal: 5-25 mg/dL
- Urea is the primary metabolite of protein catabolism, excreted entirely by the kidneys
- Unlike creatinine, BUN is NOT a direct correlate of GFR - it is heavily influenced by non-renal factors
- BUN is not elevated until GFR is reduced by approximately 75%
Causes of ELEVATED BUN:
- High dietary protein intake
- Dehydration / volume depletion
- Gastrointestinal bleeding (protein load from digested blood)
- Steroids, exercise, massive tissue breakdown
- Bilateral urinary obstruction
Causes of DECREASED BUN:
- Liver disease (impaired urea synthesis)
- Malnutrition
- Sickle cell anemia
- SIADH (dilutional)
- Overhydration
4. BUN:Creatinine Ratio
One of the most clinically useful derived values:
| BUN:Creatinine Ratio | Clinical Interpretation |
|---|---|
| ~10:1 | Normal |
| >20:1 (up to 40:1) | Prerenal azotemia (dehydration, bilateral obstruction, urinary extravasation) |
| <10:1 | Liver disease, overhydration, advanced hepatic insufficiency |
| Normal or decreased | Most intrinsic (intrarenal) disease |
(Quick Compendium of Clinical Pathology, 5e; Smith and Tanagho's General Urology, 19e)
5. Endogenous Creatinine Clearance
- Requires timed 24-hour urine collection + concurrent serum creatinine
- Normal: 90-110 mL/min (uncorrected); 70-140 mL/min when corrected for body surface area
- More accurate GFR estimate than serum creatinine alone
- Values may be falsely low if urine collection is incomplete or serum specimen not concurrent
6. Cystatin C
- Produced by nearly all nucleated cells; freely filtered at the glomerulus; completely reabsorbed by the proximal tubule
- Superior to creatinine as a predictor of cardiovascular mortality
- An early indicator of evolving CKD - rises before creatinine in early GFR decline
- Increasingly used to calculate eGFR (CKD-EPI Cys C equation)
- Not affected by muscle mass, making it especially useful in sarcopenic or obese patients
(Quick Compendium of Clinical Pathology, 5e)
7. Urine Specific Gravity and Osmolality (Tubular Function)
These test the concentrating ability of the renal tubules:
| Finding | Interpretation |
|---|---|
| SG 1.030 / Osm 1050 mOsm/kg | Excellent tubular function |
| SG 1.010 / Osm ~290 mOsm/kg (isosthenuria) | Fixed at plasma osmolality - significant renal disease |
| Urine Osm 50-100 mOsm/kg | Dilution still preserved; can occur even in advanced renal disease |
- With diminishing function, concentrating ability is lost before diluting ability
- Urine osmolality is a more precise measure than specific gravity
8. Urinalysis - Clinical Implications
Dipstick
| Component | Normal | Clinical Significance of Abnormality |
|---|---|---|
| Protein | 0 mg/dL | >150 mg/day = significant; >750 mg/day = severe glomerular damage (nephrotic range >3.5 g/day) |
| Glucose | 0 | Glycosuria = tubular reabsorption overwhelmed (diabetes, IV dextrose infusion) |
| Blood | Negative | Hematuria suggests glomerulonephritis, urolithiasis, malignancy, or infection |
| Ketones | 0 | Diabetic ketoacidosis, starvation |
| pH | 4.5-8.0 | Acidic in infection with urea-splitting organisms; alkaline in RTA |
| Bilirubin | Negative | Obstructive jaundice, hepatocellular disease |
- The dipstick is most sensitive to albumin and relatively insensitive to other proteins (e.g., Bence Jones proteins in myeloma may be missed)
- Microalbumin assay detects as little as 0.3 mg/dL - sensitive early marker of glomerular dysfunction (used in diabetic nephropathy screening)
Microscopic Urinalysis
| Finding | Normal | Clinical Significance |
|---|---|---|
| RBCs | 0-3/hpf | >3 = hematuria; dysmorphic RBCs suggest glomerular origin |
| WBCs | 0-5/hpf | Pyuria = UTI, interstitial nephritis |
| Casts | 0-2/lpf | Hyaline (nonspecific); RBC casts = glomerulonephritis; WBC casts = pyelonephritis/interstitial nephritis; granular casts = ATN |
- Urine β₂-microglobulin and lysozyme can detect tubular dysfunction specifically
9. Serum Electrolytes
| Electrolyte | Clinical Implication in Renal Disease |
|---|---|
| Sodium (133-147 mmol/L) | Helps differentiate hyponatremia causes: volume contraction vs. SIADH vs. salt-losing nephropathy |
| Potassium (3.2-5.2 mmol/L) | Hyperkalemia does not appear until uremia; critical for arrhythmia risk |
| Chloride (94-110 mmol/L) | Reflects acid-base balance; low in metabolic alkalosis, high in non-anion gap metabolic acidosis |
| CO₂/Bicarbonate (22-32 mmol/L) | Low in renal tubular acidosis, uremic acidosis |
| Calcium (8.5-10.5 mg/dL) | Low in CKD (reduced 1,25-OH vitamin D); elevated suggests hyperparathyroidism or renal cell carcinoma paraneoplastic syndrome |
| Phosphorus (2.2-4.2 mg/dL) | Elevated in CKD (reduced excretion) - drives secondary hyperparathyroidism |
Always interpret calcium alongside serum albumin: corrected Ca = measured Ca + 0.8 × (4.0 - albumin g/dL)
10. Fractional Excretion of Sodium (FENa)
A derived urinary index critical for differentiating AKI causes:
FENa (%) = (Urine Na × Plasma Cr) / (Plasma Na × Urine Cr) × 100
| FENa | Urine Osm | Urine SG | BUN:Cr | Interpretation |
|---|---|---|---|---|
| <1% | >500 mOsm/kg | >1.020 | >20:1 | Prerenal AKI (kidneys avidly retaining Na) |
| >2% | 300-400 mOsm/kg | <1.010 | <20:1 | Intrinsic renal AKI (tubular damage, can't conserve Na) |
- FENa <1% can also be seen with contrast nephropathy, myoglobinuria, and hepatorenal syndrome even with intrinsic injury
- Use FEUrea (<35% prerenal; >35% intrinsic) in patients on diuretics, where FENa is unreliable
(Quick Compendium of Clinical Pathology, 5e; Miller's Anesthesia, 10e)
11. CKD Screening (NKF Recommendations)
Annual screening is recommended in high-risk patients (diabetes, hypertension, family history of renal disease) using:
- eGFR (serum creatinine-based, CKD-EPI preferred)
- Urine microalbumin (or albumin-to-creatinine ratio)
CKD is defined by:
- GFR <60 mL/min/1.73 m² OR
- Albuminuria persisting for 3 or more consecutive months
Quick Summary: Test-to-Pathology Map
| Test | What It Primarily Assesses | Limitation |
|---|---|---|
| Serum Creatinine | Glomerular filtration | Insensitive until 50% loss; muscle-mass dependent |
| BUN | Glomerular filtration + nitrogen load | Affected by diet, hydration, GI bleeding |
| BUN:Cr ratio | Prerenal vs intrinsic disease | Affected by liver disease |
| eGFR (CKD-EPI) | Overall renal function | Not validated in AKI |
| Cystatin C | Early GFR decline | Not widely available |
| Urine SG / Osm | Tubular concentrating function | Affected by diuretics |
| Urinalysis (dipstick) | Glomerular barrier (protein), tubular threshold (glucose) | Dipstick misses non-albumin proteins |
| FENa | AKI type differentiation | Unreliable with diuretics |
| Microalbumin | Early glomerular damage | Elevated in non-renal conditions (e.g., fever, exercise) |
Sources:
- Miller's Anesthesia, 10e, Chapter 55 - Table 55.2, Glomerular Function, Tubular Function sections
- Smith and Tanagho's General Urology, 19e, Renal Function Tests chapter
- Quick Compendium of Clinical Pathology, 5e, Section 1.5.5 - Renal Function Tests and AKI evaluation
False elevation (Jaffe reaction method): cephalosporins, ketones, glucose, fructose, protein, urea, and ascorbic acid means
Finding Sources
Searching the Web
Jaffe reaction creatinine false elevation chromogens mechanism
Reading File
Reading File
Loading Image
Now I have everything needed for a thorough, textbook-backed answer.
The Jaffe Reaction and False Elevation of Creatinine
What the Jaffe Reaction Is
First described by Max Jaffe in 1886, this is the oldest colorimetric lab method still in routine clinical use. The principle is simple:
Creatinine + Picric acid (picrate ion) → Orange-red complex (read at 490-500 nm)
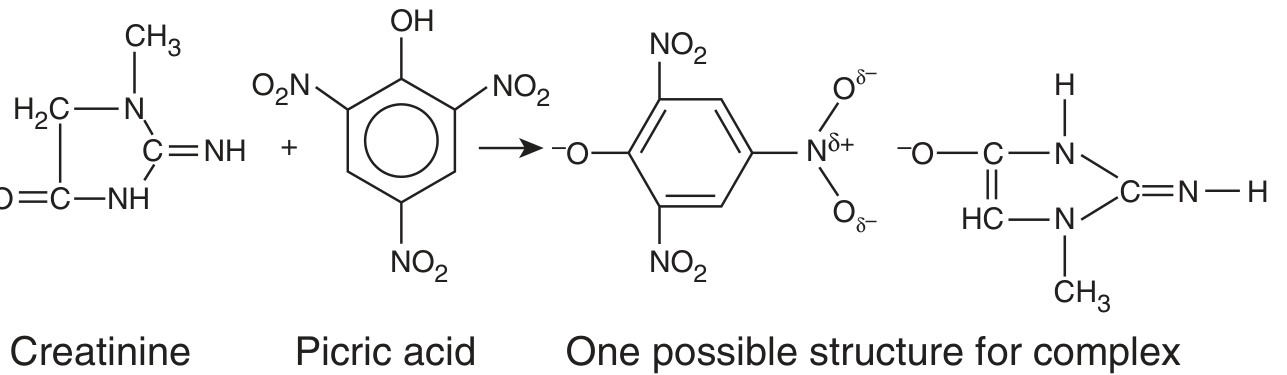
The instrument reads the intensity of this orange-red color and converts it to a creatinine concentration. The more color = the higher the reported creatinine.
(Henry's Clinical Diagnosis and Management by Laboratory Methods - Eq. 28.10)
The Core Problem: Non-Specificity
The Jaffe reaction is not specific for creatinine. Picric acid under alkaline conditions reacts with many other compounds - called "Jaffe chromogens" or "non-creatinine chromogens" - that also produce a similar orange-red color.
The machine cannot distinguish between the true creatinine-picrate complex and the false chromogen-picrate complex. It reads all the color together and reports an artificially high creatinine value.
This is the meaning of "false elevation" - the creatinine number reported by the lab is higher than the patient's actual creatinine.
Each Interferent Explained
| Interferent | Clinical Context | Mechanism / Significance |
|---|---|---|
| Ketones (acetone, acetoacetate) | DKA, starvation, prolonged fasting | Most clinically significant. Acetoacetate can raise apparent creatinine by up to 3.5 mg/dL at high concentrations. A patient with DKA may appear to have acute kidney injury when the kidneys are actually fine. |
| Cephalosporins | Antibiotic therapy | React with picrate and produce color. First-generation cephalosporins (e.g., cefazolin) are the biggest offenders. A patient on IV cefazolin may have a falsely elevated creatinine. |
| Glucose | Diabetes, IV dextrose infusion | At high serum glucose concentrations, directly interferes with the picrate reaction, producing a false color signal. Ironically, diabetics - who need accurate creatinine for detecting nephropathy - are most vulnerable to this artifact. |
| Fructose | IV fructose solutions, hereditary fructose intolerance | Similar mechanism to glucose - reacts with alkaline picrate to yield a chromogen. |
| Protein | High serum protein (e.g., hyperproteinemia) | Reacts slowly with picrate (rate becomes rapid after 80-100 seconds). Kinetic methods largely eliminate this by reading between 20-80 seconds. |
| Urea | Uremia, high-protein diet | Acts as a chromogen with alkaline picrate. Notably, patients with renal failure (high urea) already have high creatinine - the interference worsens an already-elevated value. |
| Ascorbic acid | Vitamin C supplementation, IV vitamin C | Reacts with alkaline picrate, creating a false color signal. |
(Tietz Textbook of Laboratory Medicine, 7e; Henry's Clinical Diagnosis and Management, p. 2940)
Why This Matters Clinically
1. False diagnosis of AKI or CKD:
A patient in DKA with high ketones and high glucose may show creatinine of 2.5 mg/dL on a Jaffe assay, when the true creatinine is 1.2 mg/dL. This could trigger unnecessary workup, fluid restriction, or nephrology consult.
2. Incorrect drug dosing:
Many drugs (e.g., aminoglycosides, vancomycin, renally-cleared antibiotics, chemotherapy) are dosed based on estimated GFR derived from creatinine. A falsely elevated creatinine → falsely calculated low GFR → underdosing of critical medications.
3. Masking true renal disease in diabetics:
In poorly controlled diabetes, elevated glucose AND ketones both falsely inflate the Jaffe creatinine. This can mask early diabetic nephropathy by making creatinine appear higher than it truly is - or conversely create spurious concern at what is actually a normal level.
4. Bilirubin does the opposite:
Elevated bilirubin (icteremia) is a negative interferent - it absorbs at a wavelength that competes with the orange-red complex, causing creatinine to be falsely low (opposite effect).
How Labs Minimize These Interferences
| Strategy | How It Helps |
|---|---|
| Kinetic (rate) Jaffe assay | Reads the color change between 20-80 seconds after mixing. Ketones/acetoacetate react very fast (0-20 s) and protein reacts slow (>80 s). Reading in the "window" largely excludes both. |
| Enzymatic creatinine assay | Uses creatininase + creatinase + sarcosine oxidase enzymes - highly specific for creatinine, not affected by chromogens. Now preferred in reference labs. |
| Ferricyanide addition | Oxidizes bilirubin to biliverdin, reducing its negative interference. |
| Dilution of urine samples | Urine creatinine is so much higher than serum that chromogen interference is proportionally negligible in urine - Jaffe is more reliable for urine than for serum. |
Summary in One Sentence
The Jaffe reaction measures color intensity, not creatinine specifically - so any substance that also turns orange-red with alkaline picrate (ketones, glucose, cephalosporins, etc.) gets counted as "creatinine," making the reported value falsely higher than the true value.
Sources:
- Tietz Textbook of Laboratory Medicine, 7e - Chemical Methods: The Jaffe Reaction
- Henry's Clinical Diagnosis and Management by Laboratory Methods - Creatinine section, p. 2938-2940
- Quick Compendium of Clinical Pathology, 5e - Section 1.5.5.1.2
This is a shared conversation. Sign in to Orris to start your own chat.