intercostal space icision
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, textbook-referenced guide to intercostal space incisions:
Intercostal Space Incision
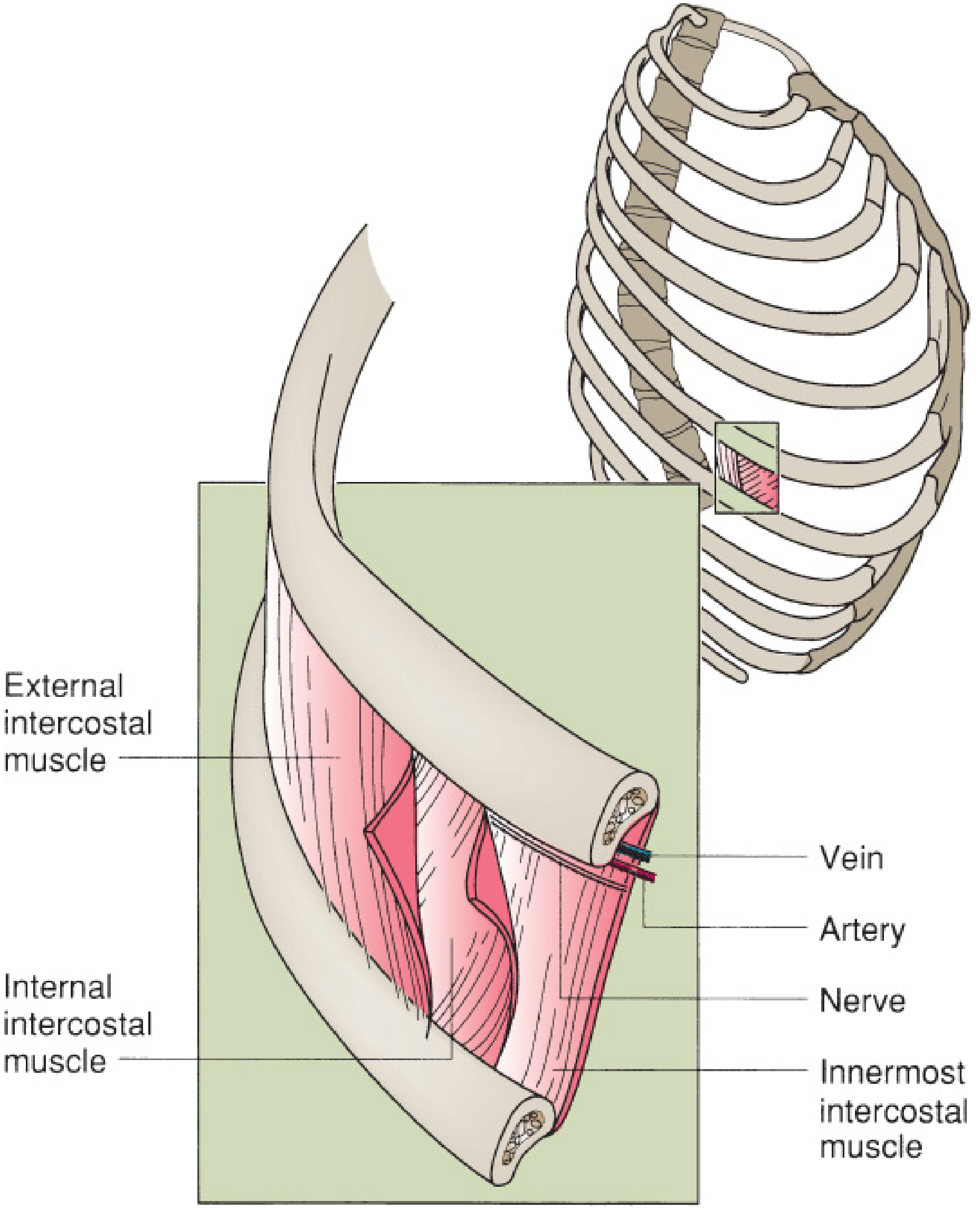
Anatomy of the Intercostal Space
Each intercostal space contains three muscle layers and a neurovascular bundle:
| Layer (outer to inner) | Notes |
|---|---|
| External intercostal muscle | Fibres run downward and forward |
| Internal intercostal muscle | Fibres run downward and backward |
| Innermost intercostal muscle | Deepest layer, runs parallel to internal |
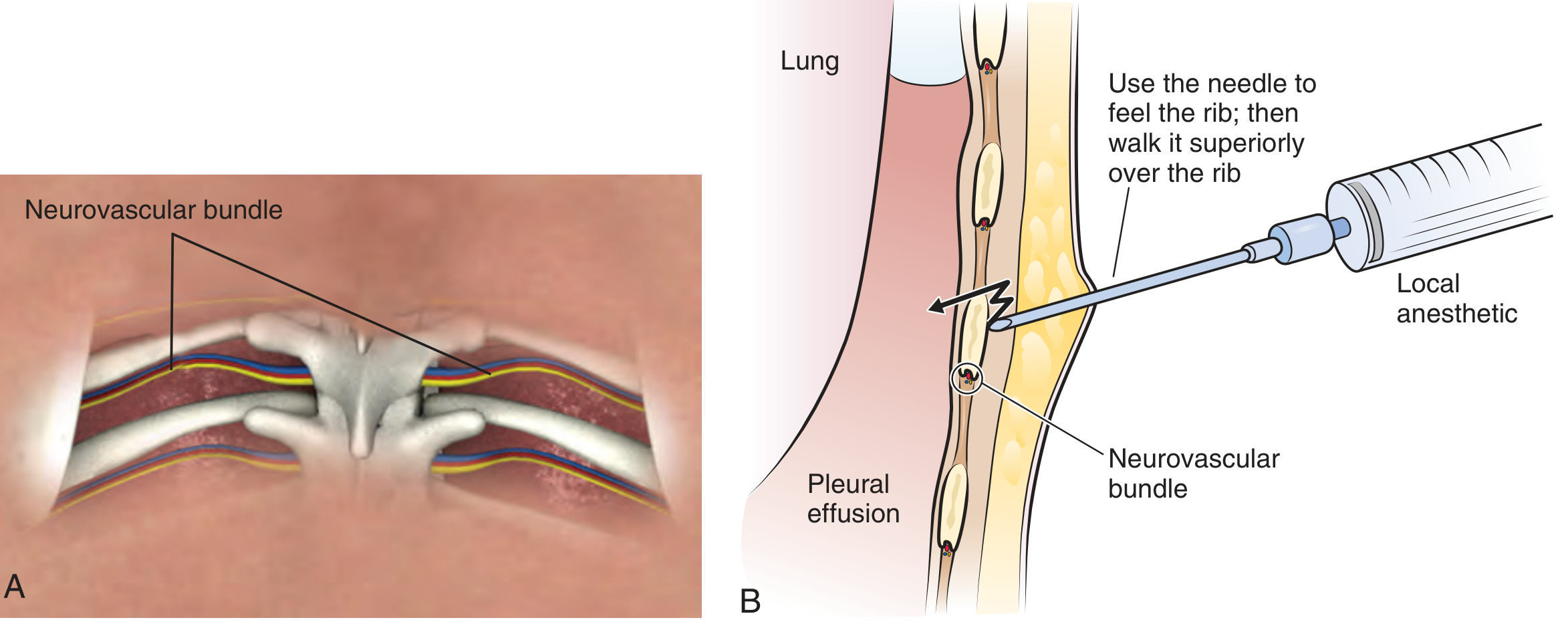
The neurovascular bundle (intercostal vein, artery, nerve - arranged VAN from top to bottom) runs in the costal groove along the inferior aspect of each rib.
The Golden Rule of Intercostal Incision
Always enter the intercostal space just above (superior to) the upper border of the lower rib.
This keeps the instrument/incision away from the neurovascular bundle hugging the underside of the upper rib. Violating this rule risks:
- Intercostal artery hemorrhage (can be severe - these communicate with the aorta)
- Intercostal nerve injury (persistent post-procedural pain/neuralgia)
- Intercostal vein injury
Common Clinical Procedures Using Intercostal Incisions
1. Tube Thoracostomy (Chest Tube Insertion)
Site: 4th or 5th intercostal space, midaxillary to anterior axillary line (at the level of the nipple in men, inframammary crease in women).
Technique:
- Make an oblique skin incision 1-2 cm below the intended interspace of tube placement
- Use a large clamp to tunnel through subcutaneous tissue and intercostal muscles, entering the next higher interspace just above the rib
- Once through the internal intercostal fascia, open the clamp to enlarge the hole to ~2 cm
- Insert a finger to confirm intrapleural position and check for lung adhesions
- Advance the chest tube until the last side hole is within the pleural space
- Tintinalli's Emergency Medicine
The oblique subcutaneous tunnel technique closes naturally after tube removal, reducing recurrent pneumothorax risk.
2. Thoracentesis (Needle Aspiration)
Site: Posterior chest, 1-2 interspaces below the fluid level (confirmed by ultrasound), typically around the 7th-9th intercostal space posteriorly.
Technique:
- Insert needle above the superior edge of the lower rib
- "Walk" the needle up and over the rib surface until it slips into the intercostal space
- Advance until the pleural space is entered (a "pop" may be felt)
- Always use ultrasound guidance when available to reduce the risk of pneumothorax and visceral injury
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
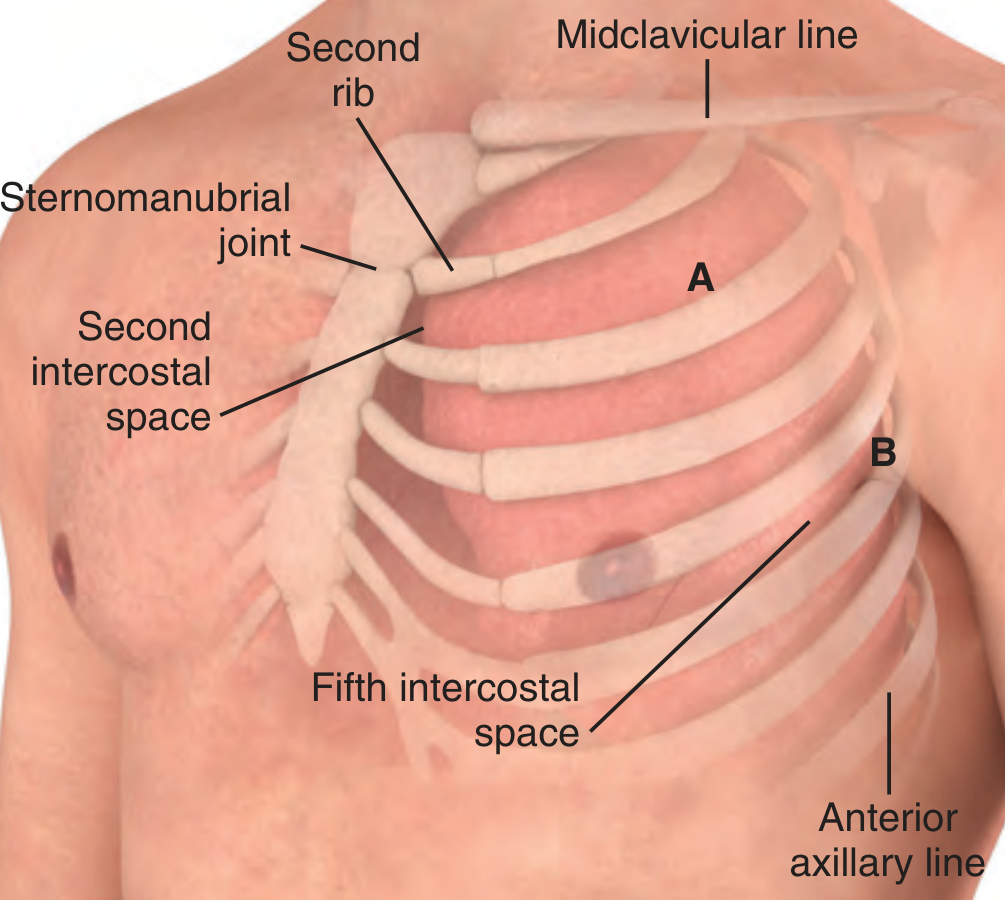
3. Needle Thoracostomy (Tension Pneumothorax Decompression)
Site: Traditionally 2nd intercostal space, midclavicular line. More recently, the 4th-5th ICS at the anterior axillary line is preferred because it provides the shortest distance from skin to pleura and avoids the thick chest wall (mean thickness ~4.5 cm in the US).
Technique: Insert catheter-over-needle at the selected site, entering just above the lower rib.
- Tintinalli's Emergency Medicine
4. Open Thoracotomy / Thoracoscopy (VATS)
For thoracotomy incisions, the intercostal muscles are divided along the lower margin of the interspace, taking care not to injure the neurovascular bundle below the rib above. The pleural cavity is then entered.
For urologic thoracoabdominal approaches, the incision runs along the 8th or 9th intercostal space from the posterior axillary line curving over the costal margin into the abdomen.
- Schwartz's Principles of Surgery, 11e; Campbell-Walsh-Wein Urology
Summary: Key Points
| Principle | Detail |
|---|---|
| Safe entry zone | Just above the upper border of the lower rib |
| Neurovascular bundle location | Inferior groove of each rib (VAN order: vein, artery, nerve) |
| Chest tube site | 4th-5th ICS, anterior-midaxillary line |
| Needle decompression site | 2nd ICS midclavicular line OR 4th-5th ICS anterior axillary line |
| Thoracentesis site | Upper border of lower rib, posterior chest |
| Skin incision for chest tube | 1-2 cm below the actual interspace entry, then tunnel upward |
The fundamental reason all intercostal procedures target the superior aspect of the lower rib is to stay safely away from the neurovascular bundle tucked into the costal groove above.
This is a shared conversation. Sign in to Orris to start your own chat.