Heel painheel pain
Reading File
Finding Sources
Finding Sources
Searching PubMed
"plantar fasciitis" AND treatment
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Now I have comprehensive information to provide a detailed answer on heel pain.
Heel Pain - A Comprehensive Clinical Overview
Epidemiology
About 10% of people will experience an episode of plantar heel pain at some point in their lives. More than 2 million patients are treated for plantar fasciitis every year in the United States alone. It is more common in rheumatology patients and in active individuals.
- Rheumatology, 2-Volume Set (Elsevier 2022), p. 756
Differential Diagnosis of Heel Pain
Heel pain has multiple causes, broadly divided by anatomical location:
Plantar (Under the Heel)
| Condition | Key Features |
|---|---|
| Plantar fasciitis (plantar fasciopathy) | Most common cause; worst pain in morning first steps |
| Heel pad atrophy | Degeneration of elastic adipose tissue; worse with aging |
| Calcaneal stress fracture | Athletes; diffuse heel pain with activity |
| Plantar calcaneal bursitis | Localized swelling under the heel |
| Entrapment of Baxter's nerve (1st branch of lateral plantar nerve) | Neurogenic pain, lateral heel tenderness |
| Tarsal tunnel syndrome | Burning/tingling along medial heel and sole |
| Plantar heel spur | Osseous exostosis; often a result of chronic plantar fasciitis |
| Soft tissue abscess | Consider in diabetic/neuropathic patients |
Posterior (Behind the Heel)
| Condition | Key Features |
|---|---|
| Achilles tendinopathy / enthesitis | Common in seronegative arthropathies (AS, PsA, ReA) |
| Retrocalcaneal bursitis | Deep to Achilles; associated with RA and inflammatory disease |
| Achilles bursa (superficial) | Mechanical irritation from footwear |
| Haglund's deformity/exostosis | Dorsal calcaneal prominence; bursal inflammation |
| Insertional Achilles tendinopathy | Posterior heel spur at tendon insertion |
Systemic / Other
- Rheumatoid arthritis, ankylosing spondylitis, Reiter syndrome - especially if bilateral heel pain
- Calcaneal apophysitis (Sever's disease) - children/adolescents during growth spurts
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 4902; THIEME Atlas of Anatomy
Plantar Fasciitis - The Most Common Cause
Risk Factors
- Obesity
- Pes planus (flat foot) or pes cavus (high arch)
- Limited ankle dorsiflexion
- Prolonged standing or walking on hard surfaces
- Inappropriate footwear
- Runners (especially with change to harder surface or increased mileage)
Mechanism - Windlass Effect
The plantar fascia originates from the anteromedial calcaneal tuberosity and inserts into the metatarsophalangeal joint plantar plates. When toes dorsiflex, the fascia tightens around the metatarsal heads (windlass mechanism), elevating the longitudinal arch and placing maximum traction at the calcaneal origin - the point of peak tenderness.
Classic Presentation
- Morning pain: severe pain with the very first steps on arising (or after periods of inactivity)
- Pain lessens initially with walking, then worsens with continued activity
- Pain worse on walking barefoot or going up stairs
- Tenderness on palpation over the inferior heel at the plantar fascia calcaneal attachment
Imaging
Ultrasound (below): Shows thickening of the fascia at the calcaneal insertion and diffuse hypoechogenicity (edema). The arrows indicate marked fascial thickening at the calcaneus (C), with more normal structure distally (arrowheads).
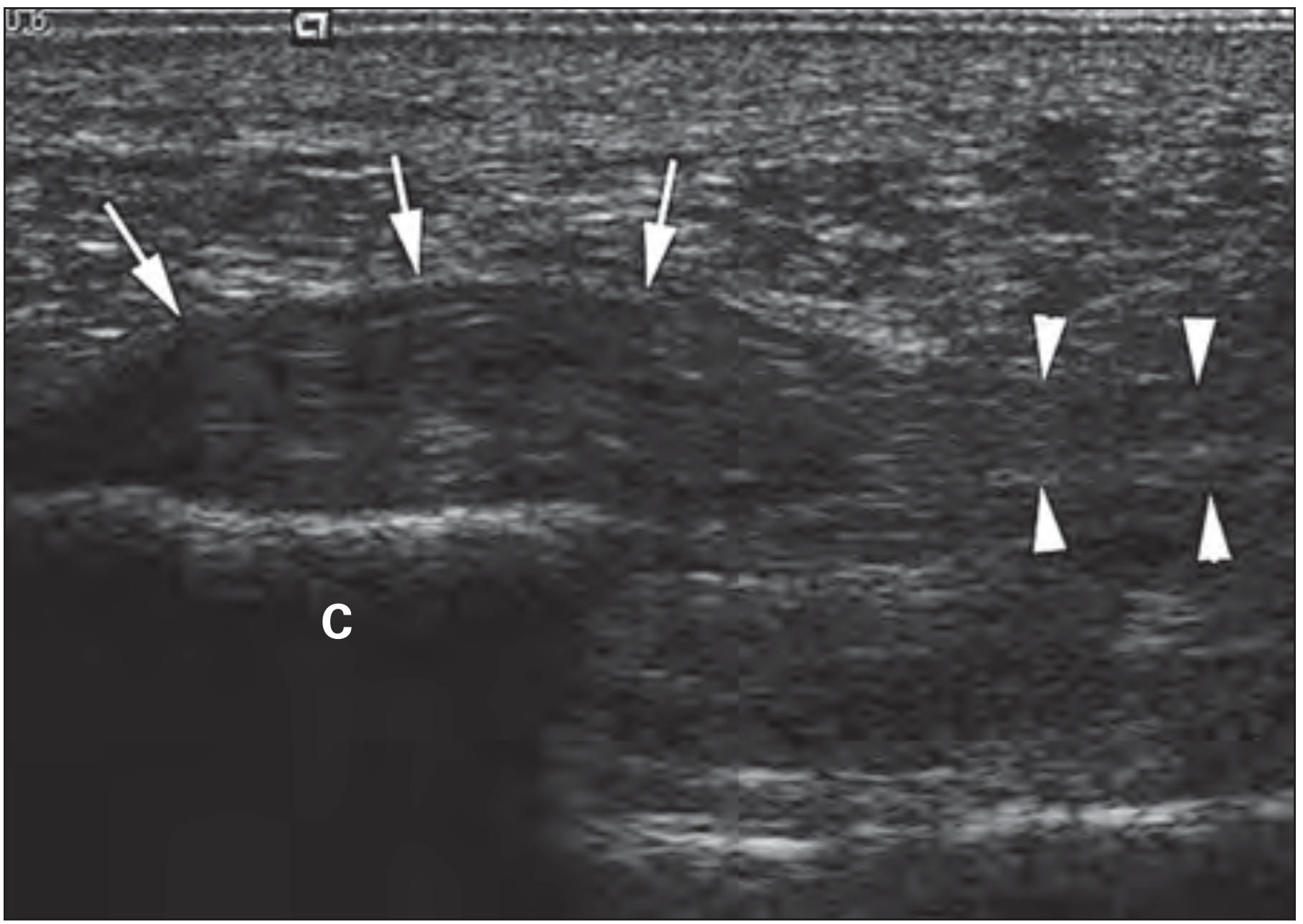
Ultrasound showing plantar fasciitis - marked thickening of fascia (arrows) at the calcaneus (C), normal structure distally (arrowheads). From Rheumatology, 2-Volume Set, p. 756.
- Plain X-ray: May show a heel spur (calcaneal enthesophyte) - of little diagnostic significance on its own
- MRI: Sensitive but usually not needed to establish the diagnosis
Management
Conservative (First-Line) - >80% resolve within 12 months
- Activity modification: Reduce or eliminate inciting activities
- Stretching: Plantar fascia and calf stretching exercises
- Ice, heat, massage
- Footwear modification: Supportive shoes with cushioning
- Orthoses: Medial arch support (contoured foot orthoses)
- Taping: "Low-Dye" taping has evidence of efficacy
- Night splints: Keep ankle in neutral position to prevent contracture
- Weight loss: Helpful in overweight patients
- NSAIDs: Short course for those without contraindications
Injections
- Corticosteroid injection: Evidence for short-term benefit, but painful and long-term benefits unclear; small risk of plantar fascia rupture with repeated injections
- PRP (platelet-rich plasma): Emerging evidence, particularly for tendinopathy (recent meta-analysis, 2025)
Extracorporeal Shock Wave Therapy (ESWT)
- Evidence supports use for chronic/recalcitrant cases
- A recent 2024 systematic review and meta-analysis (PMID 38738305) comparing ESWT to corticosteroid injections found ESWT is effective for pain, plantar fascia thickness, and foot function, with more durable benefits than corticosteroids
Surgery
- Plantar fasciotomy: Reserved for patients who have failed at least 6-12 months of conservative treatment
- Gastrocnemius recession is an option in patients with associated gastrocnemius tightness
Posterior Heel / Bursitis Treatment
- Physical therapy + NSAIDs for mechanical bursitis
- Footwear modification to offload the posterior heel
- Corticosteroid injection for inflammatory bursitis (RA-associated)
- Harrison's Principles of Internal Medicine 22E, p. 3019; Rheumatology 2-Volume Set, p. 756
Red Flags - When to Investigate Further
- Bilateral heel pain - rule out seronegative spondyloarthropathy (ankylosing spondylitis, psoriatic arthritis, reactive arthritis)
- Heel pain in a diabetic or immunocompromised patient - rule out deep soft-tissue abscess
- Night pain or rest pain - consider neoplasm or systemic disease
- Failure to improve with conservative treatment at 6-12 weeks - consider imaging (MRI, bone scan)
Sources: Harrison's Principles of Internal Medicine 22E; Rheumatology 2-Volume Set (Elsevier 2022); Campbell's Operative Orthopaedics 15th Ed 2026; THIEME Atlas of Anatomy
This is a shared conversation. Sign in to Orris to start your own chat.