Salt and start protocol
Reading File
Finding Sources
Finding Sources
Searching the Web
SALT START triage protocol mass casualty emergency
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full breakdown:
SALT and START Triage Protocols
These are the two most widely used mass casualty incident (MCI) / multiple casualty triage systems in emergency and disaster medicine.
START Triage
Simple Triage and Rapid Treatment - the older of the two systems, developed in 1983 through collaboration between Hoag Memorial Hospital and Newport Beach Fire Department.
How it works: RPM (Respirations, Perfusion, Mental Status)
Step 1: Ask all walking victims to move to a designated area. They are classified GREEN ("walking wounded") and reassessed later.
Step 2: For all remaining patients, assess in ~30-60 seconds:
| Parameter | Finding | Category |
|---|---|---|
| Respirations | Absent after airway opening | BLACK (dead) |
| >30/min | RED (immediate) | |
| <30/min | Assess next | |
| Perfusion | Radial pulse absent or HR >120 | RED (immediate) |
| Pulse present | Assess next | |
| Mental status | Cannot follow simple commands | RED (immediate) |
| Can follow commands | YELLOW (delayed) |
Interventions during START: Only airway opening and direct pressure on obvious hemorrhage.
START Color Categories
- 🔴 RED - Immediate: Life-threatening but salvageable; needs care within minutes
- 🟡 YELLOW - Delayed: Serious injury but can wait
- 🟢 GREEN - Minimal: "Walking wounded," minor injuries
- ⚫ BLACK - Deceased/Expectant: Dead or unsurvivable
Pediatric version: JumpSTART (for children <8 years) - adds 5 rescue breaths for apneic children with a pulse before declaring black, and modifies respiratory/mental status thresholds.
Rosen's Emergency Medicine: "For anyone considering implementing an adult mass casualty triage algorithm, we recommend using START triage until more evidence emerges describing the performance of SALT triage in actual disasters."
SALT Triage
Sort, Assess, Lifesaving Interventions, Treatment/Transport - developed in 2008 by a CDC-sponsored expert panel. Endorsed by ACEP, ACS-COT, American Trauma Society, NAEMSP, and NDLSF. Designed as the national all-hazards standard.
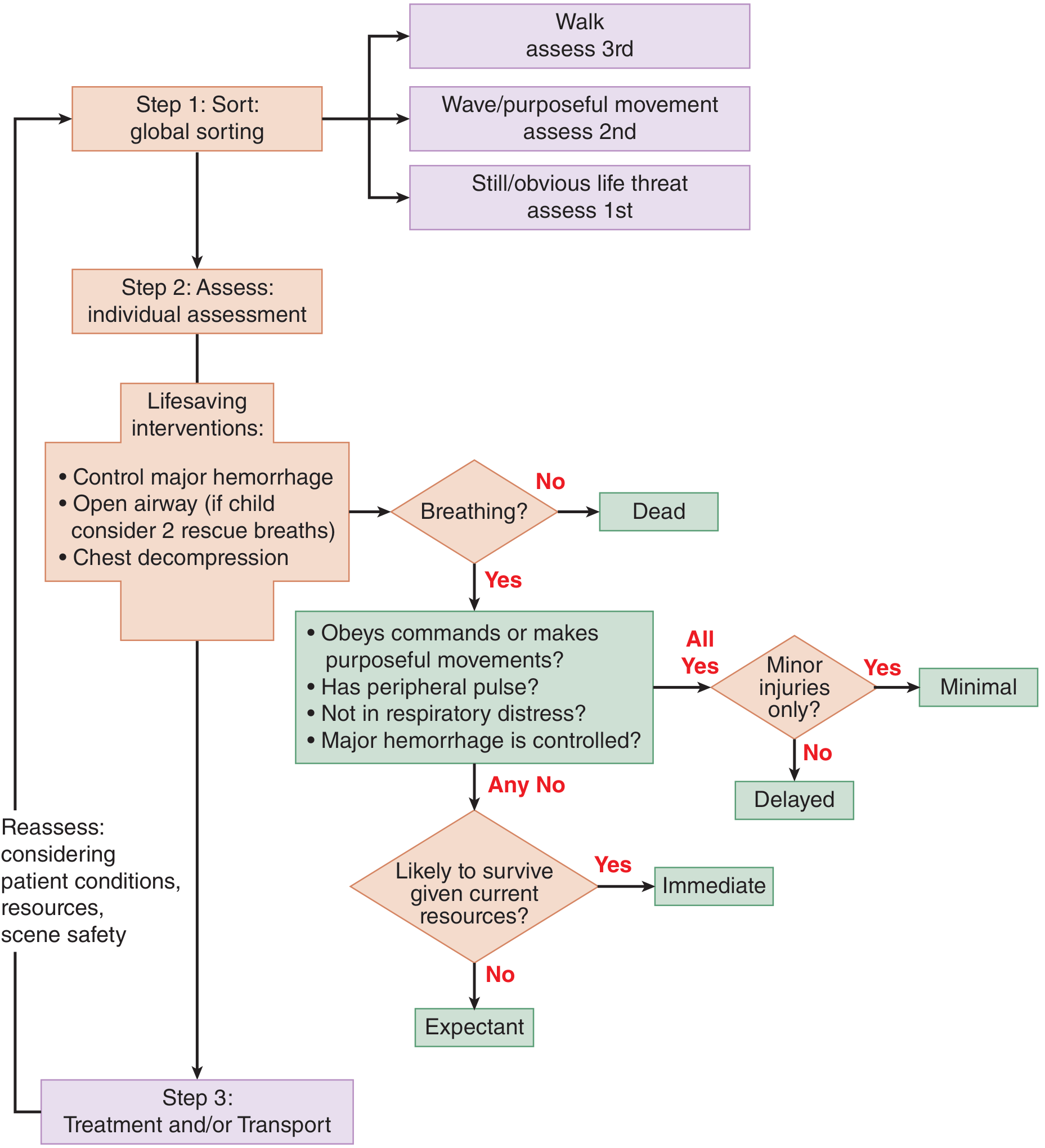
Step 1: SORT - Global Sorting (three tiers)
| Command | Response | Assessment Priority |
|---|---|---|
| "Walk to this area" | Walks | 3rd (last) - intact airway, breathing, circulation, and mentation |
| "Wave/move" | Waves/purposeful movement | 2nd |
| No movement / obvious life threat | Still | 1st (most likely to need lifesaving intervention) |
Step 2: ASSESS + Lifesaving Interventions (LSI)
For each patient individually. Lifesaving interventions must be:
- Provided quickly
- Greatly improve survival likelihood
- Not require the provider to stay with the patient
- Within scope of practice
- Require only immediately available equipment
Permitted LSIs:
- Control major hemorrhage (tourniquet, wound packing)
- Open airway (airway positioning; in children, consider 2 rescue breaths)
- Chest decompression
Step 3: ASSIGN Triage Category
After LSI, ask: Does the patient obey commands or make purposeful movements? Have a peripheral pulse? Have no respiratory distress? Is major hemorrhage controlled?
| All 4 "Yes" | Minor injuries only? | Category |
|---|---|---|
| Yes | Yes | 🟢 MINIMAL |
| Yes | No | 🟡 DELAYED |
| Any "No" | Likely to survive given current resources? Yes | 🔴 IMMEDIATE |
| Any "No" | Likely to survive given current resources? No | ⚫/🩶 EXPECTANT |
Step 4: TREATMENT/TRANSPORT
Reassess continuously, considering patient conditions, available resources, and scene safety.
SALT's 5 Categories (vs. START's 4)
SALT adds a distinct EXPECTANT category (grey) for patients who are still alive but have unsurvivable injuries given available resources - keeping them separate from the dead (BLACK). This is a key difference from START.
Side-by-Side Comparison
| Feature | START | SALT |
|---|---|---|
| Year | 1983 | 2008 |
| Origin | Hoag Hospital / Newport Beach FD | CDC-sponsored national panel |
| Steps | Global sort then RPM assessment | Sort → Assess → LSI → Treat/Transport |
| Assessment basis | Respirations, Perfusion, Mental status | Commands/movement, pulse, respiratory distress, hemorrhage control |
| Categories | 4 (Red/Yellow/Green/Black) | 5 (Immediate/Delayed/Minimal/Expectant/Dead) |
| Lifesaving interventions | Airway only + direct pressure | Hemorrhage control, airway, chest decompression |
| Expectant category | Grouped with Dead (Black) | Separate (Grey) |
| Pediatric modification | JumpSTART | Built-in (2 rescue breaths for apneic children) |
| Evidence in real disasters | Validated (2002 Placentia Linda crash) | Less real-disaster evidence as of latest guidelines |
| National endorsement | Widely used by EMS | Endorsed by ACEP, ACS-COT, NAEMSP |
Key Clinical Points
- Triage is dynamic - patients must be reassessed at each level of care as conditions evolve.
- No CPR during disaster triage - resources must be allocated to salvageable patients.
- SALT balances sensitivity and specificity better than START per evidence reviewed by Tintinalli's, but START has more real-world validation data.
- SAVE system (Secondary Assessment of Victim Endpoint) can be layered on top of START/SALT for catastrophic/compartmentalized disasters where patients remain on scene for extended periods.
- Command and control is mandatory - triage requires a single designated triage point, a triage algorithm, a triage officer, and a PACE (Primary, Alternate, Contingency, Emergency) response plan.
Sources: Tintinalli's Emergency Medicine, p. 2055 | Rosen's Emergency Medicine, p. 3745-3746 | Current Surgical Therapy 14e | CDC SALT 2008 original paper
This is a shared conversation. Sign in to Orris to start your own chat.