Tell me hypo and hyper natremia and kalemia in detail with proper understanding with photos medicine mbbs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I have enough data to compile a comprehensive answer. Let me now write the complete detailed response.
Disorders of Sodium and Potassium: Complete MBBS Guide
PART 1: SODIUM DISORDERS
Normal Values
| Parameter | Normal Range |
|---|---|
| Serum Na+ | 136-145 mmol/L |
| Plasma Osmolality | 280-295 mOsm/kg |
| Urine Osmolality | 50-1200 mOsm/kg |
HYPONATREMIA (Na+ < 136 mmol/L)
Definition & Epidemiology
Hyponatremia is the most commonly encountered electrolyte disorder, with incidences as high as 15-30% in hospitalized patients. It is defined as plasma Na+ < 135-136 mmol/L and is a marker for worse outcomes - a serum sodium < 135 mmol/L is associated with ~45% relative increase in ICU admission rates.
- Tietz Textbook of Laboratory Medicine, 7th Ed
- Goldman-Cecil Medicine
Step 1: Classify by Plasma Osmolality
The first step is always to measure plasma osmolality. This divides hyponatremia into three types:
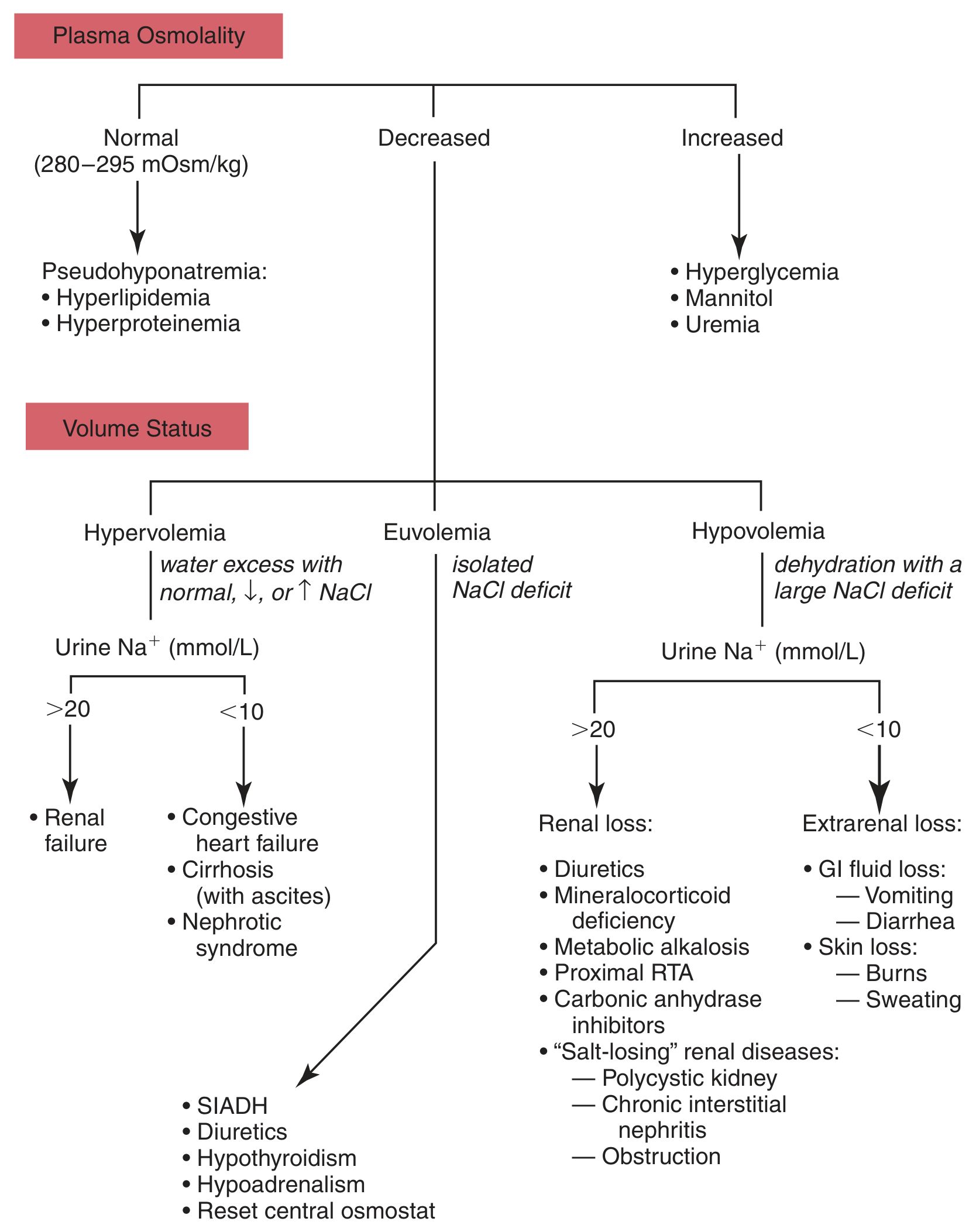
Fig. Differential diagnosis of hyponatremia by plasma osmolality and volume status (Tietz Textbook of Laboratory Medicine)
A. Isotonic Hyponatremia (Pseudo-hyponatremia)
- Plasma osmolality = NORMAL (280-295 mOsm/kg)
- No true water excess; artifact of measurement
- Causes: Hyperlipidemia, Hyperproteinemia (multiple myeloma, Waldenstrom's macroglobulinemia)
- No treatment needed for the Na+ itself
B. Hypertonic Hyponatremia
- Plasma osmolality = INCREASED (>295 mOsm/kg)
- Another osmotically active solute draws water out of cells, diluting Na+
- Causes: Hyperglycemia (for every 100 mg/dL rise in glucose above normal, Na+ drops ~1.6 mEq/L), Mannitol, Uremia
C. Hypotonic Hyponatremia (the true hyponatremia you must treat)
- Plasma osmolality = DECREASED (<280 mOsm/kg)
- Always reflects an underlying disorder with abnormal retention of body water
Step 2: Classify Hypotonic Hyponatremia by Volume Status
| Volume Status | ECF | Mechanism | Key Causes |
|---|---|---|---|
| Hypovolemic | Low | Na+ loss > water loss | Diarrhea, vomiting, burns, sweating (extrarenal); diuretics, mineralocorticoid deficiency, salt-losing nephropathy (renal) |
| Euvolemic | Normal | Water retention with normal/low Na+ | SIADH, hypothyroidism, hypoadrenalism, reset osmostat, excess water intake |
| Hypervolemic | High | Water excess with normal or elevated Na+ | CHF, cirrhosis with ascites, nephrotic syndrome, renal failure |
Key lab differentiator - Urine Na+:
- Urine Na+ >20 mmol/L = renal losses (diuretics, SIADH, renal failure, mineralocorticoid deficiency)
- Urine Na+ <10 mmol/L = extrarenal losses (CHF, cirrhosis, vomiting, diarrhea)
SIADH (Syndrome of Inappropriate ADH Secretion)
This is the most common cause of euvolemic hyponatremia and deserves special attention.
Diagnostic criteria:
- Hypo-osmolar hyponatremia (plasma Osm <280)
- Urine osmolality > plasma osmolality (inappropriately concentrated urine, usually >100 mOsm/kg)
- Urine Na+ >20-40 mmol/L
- Normal renal, adrenal, thyroid function
- Patient is euvolemic
Causes of SIADH (mnemonic - SIADH itself):
- CNS disorders: meningitis, SAH, head trauma, stroke
- Pulmonary: pneumonia, TB, abscess, SCLC
- Drugs: SSRIs, carbamazepine, cyclophosphamide, NSAIDs, morphine, oxytocin
- Tumors: small cell lung cancer (ectopic ADH), pancreatic ca
- Misc: pain, nausea, postoperative state
Clinical Features of Hyponatremia
Symptoms are primarily neurological due to osmotic water shift INTO brain cells (cerebral edema):
| Plasma Na+ (mmol/L) | Symptoms |
|---|---|
| 130-135 | Often asymptomatic; nausea, malaise |
| 125-130 | Headache, lethargy, confusion |
| 120-125 | Generalized weakness, mental confusion |
| <120 | Severe confusion, stupor, seizures |
| <105 | Coma, respiratory arrest, death |
Important: Symptoms develop faster with acute hyponatremia (hours-days) vs. chronic (>48 hrs). In chronic hyponatremia, the brain adapts by extruding osmolytes, so symptoms may be minimal even at Na+ <120.
Women between menarche and menopause are at greater risk for fatal cerebral edema from acute hyponatremia.
Osmotic Demyelination Syndrome (ODS) / Central Pontine Myelinolysis (CPM)
This is the most feared complication of overcorrecting hyponatremia too rapidly.
Mechanism: Rapid correction of chronic hyponatremia causes the brain (which has adapted by extruding osmolytes) to undergo sudden dehydration. This damages myelin sheaths - predominantly in the central pons.
Risk factors:
- Severe chronic hyponatremia (Na+ <120, duration >48 hrs)
- Alcoholism, malnutrition, liver transplantation (incidence 13-29% at autopsy), hypokalemia
Clinical picture (BIPHASIC):
- Initial improvement with correction
- 2-3 days later: behavioral changes, cranial nerve palsies, progressive quadriplegia, "locked-in syndrome"
MRI: T2 hyperintense non-enhancing pontine and extrapontine lesions (may not appear for 2 weeks)
Prevention:
- Correct Na+ by no more than 8-10 mEq/L per 24 hours (max 18 mEq/L per 48 hrs)
- In high-risk patients: max 8 mEq/L per 24 hrs
Treatment of Hyponatremia
General principle: Rate of correction depends on duration and severity of symptoms
| Scenario | Correction Strategy |
|---|---|
| Acute symptomatic (<48 hrs, seizures/coma) | 3% hypertonic saline IV; raise Na+ by 1-2 mEq/L/hr until symptoms resolve (max ~5 mEq in first 1-2 hrs); then slow to <8-10 mEq/24hrs |
| Chronic symptomatic (mild-moderate) | Fluid restriction ± 3% saline; max 8-10 mEq/L/24 hrs |
| Hypovolemic | 0.9% normal saline (corrects volume, allows ADH to suppress, kidneys excrete free water) |
| SIADH | Fluid restriction (800-1000 mL/day); vaptans (tolvaptan, conivaptan) if persistent |
| Hypervolemic (CHF, cirrhosis) | Fluid restriction, treat underlying cause, loop diuretics |
Vaptans (V2 receptor antagonists): Tolvaptan, conivaptan - block ADH at V2 receptor in collecting duct, promote free water excretion (aquaresis) without sodium loss. Used in SIADH and hypervolemic hyponatremia.
HYPERNATREMIA (Na+ > 144-145 mmol/L)
Definition & Key Concept
Hypernatremia ALWAYS reflects hypertonicity - water deficit relative to sodium. It always means the body has too little water relative to its solute load. The primary defense is thirst - failure of this mechanism is almost always required for hypernatremia to persist.
Goldman-Cecil Medicine
Causes - Classified by Volume Status
| Category | Mechanism | Examples |
|---|---|---|
| Hypovolemic | Water lost > Na+ lost | Diarrhea, vomiting, burns, sweating, loop diuretics, osmotic diuresis |
| Euvolemic (Near-normovolemic) | Pure water loss | Diabetes insipidus (central or nephrogenic), fever/insensible loss, inadequate water intake (adipsia/hypodipsia) |
| Hypervolemic | Excess Na+ gain | Hypertonic saline, sodium bicarbonate excess, hyperaldosteronism, Cushing's |
Diabetes Insipidus (DI) - Key Cause of Hypernatremia
| Feature | Central DI | Nephrogenic DI |
|---|---|---|
| Defect | ADH production/release (pituitary/hypothalamus) | Renal tubule unresponsive to ADH |
| Causes | Head trauma, neurosurgery, tumors, infiltrative (sarcoid, histio X), idiopathic | Lithium, demeclocycline, hypercalcemia, hypokalemia, CKD, genetic (V2R mutation) |
| Urine Osm after water deprivation | Low (<200); rises with DDAVP | Low (<200); NO rise with DDAVP |
| Treatment | DDAVP (desmopressin) | Treat cause; thiazide diuretics + low Na diet; NSAIDs; amiloride (lithium-induced) |
Diagnosis: Urine osmolality <100-200 mOsm/kg + polyuria (>3 L/day) in the setting of hypernatremia strongly suggests DI
Clinical Features of Hypernatremia
Primary symptoms are neurological (due to water shifting OUT of brain cells - cell shrinkage):
- Early: Thirst, restlessness, irritability
- Moderate: Confusion, weakness, focal neurologic deficits, muscle twitching
- Severe: Decreasing consciousness → seizures → coma
- Brain cell shrinkage can rupture bridging veins → subdural hemorrhage
In patients with hypernatremia of sufficient duration, brain cells compensate by generating "idiogenic osmoles" (organic osmolytes), reducing clinical manifestations.
Treatment of Hypernatremia
Free Water Deficit Formula:
Water deficit = TBW × [(plasma Na+ / 140) - 1] TBW = 0.6 × lean body weight (men) or 0.5 × lean body weight (women)
Example: 70 kg man, Na+ = 160 mEq/L
- TBW = 0.6 × 70 = 42 L
- Water deficit = 42 × (160/140 - 1) = 42 × 0.143 = 6 L
| Priority | Action |
|---|---|
| 1. Hemodynamic instability | 0.9% saline first to restore volume |
| 2. Calculate water deficit | Use formula above |
| 3. Choose replacement fluid | D5W (free water), 0.45% saline, or oral water |
| 4. Rate of correction | Max 0.5-1 mEq/L/hour (max 10-12 mEq/L/day) to avoid cerebral edema from rapid rehydration |
| 5. Treat underlying cause | Stop offending agents, treat DI, etc. |
Warning: Correcting too fast (>0.7 mEq/L/hr) is dangerous and can lead to cerebral edema. The brain's accumulated idiogenic osmoles retain water rapidly when plasma osmolality drops.
National Kidney Foundation Primer on Kidney Diseases, 8th Ed
PART 2: POTASSIUM DISORDERS
Normal Values & Physiology
| Parameter | Value |
|---|---|
| Normal serum K+ | 3.5-5.0 mEq/L |
| Intracellular K+ | ~140 mEq/L |
| Extracellular K+ | ~4 mEq/L |
| Total body K+ | ~3500 mEq (98% intracellular) |
Key physiological point: 98% of body potassium is intracellular. The serum K+ level does NOT directly reflect total body K+ stores. Transcellular shifts can change serum K+ dramatically with no change in total body K+.
What moves K+ INTO cells (lowers serum K+):
- Insulin
- Beta-2 adrenergic stimulation (catecholamines)
- Alkalosis
- Thyroid hormone
What moves K+ OUT of cells (raises serum K+):
- Acidosis (especially metabolic/hyperchloremic)
- Insulin deficiency
- Beta-blockade
- Hypertonicity/hyperglycemia
- Cell destruction
Medical Physiology (Boron & Boulpaep); Harrison's Principles of Internal Medicine 22E
HYPOKALEMIA (K+ < 3.5 mEq/L)
Causes
1. RENAL LOSSES (most common; urine K+ >20 mEq/L)
| Category | Examples |
|---|---|
| Diuretics | Loop diuretics (furosemide), thiazides - most common cause |
| Mineralocorticoid excess | Primary hyperaldosteronism (Conn's), secondary aldosteronism, Cushing's |
| Renal tubular disorders | RTA type 1 & 2, Fanconi syndrome |
| Magnesium deficiency | Refractory hypokalemia - always check Mg2+ |
| Drugs | Amphotericin B, aminoglycosides, cisplatin |
| Bartter and Gitelman syndromes | Genetic tubular disorders |
2. GASTROINTESTINAL LOSSES (urine K+ <20 mEq/L)
- Severe diarrhea (secretory diarrhea - high K+ content)
- Vomiting (indirect - metabolic alkalosis drives renal K+ wasting + low Cl-)
- Laxative abuse
- Malabsorption, fistulas, ileostomy
3. POOR INTAKE
- Starvation, alcoholism, anorexia
- Pica (clay ingestion binds K+ in GI tract)
- IV fluids without K+ replacement
4. TRANSCELLULAR SHIFT (total body K+ normal)
- Alkalosis
- Insulin administration (especially during DKA treatment)
- Beta-2 agonists (albuterol, salbutamol, ritodrine)
- Thyrotoxic periodic paralysis (TPP) - common in Asian males
- Familial hypokalemic periodic paralysis (KCNJ2/CACNA1A mutations)
- Barium poisoning
Clinical Features of Hypokalemia
Severity increases with degree of hypokalemia:
| Serum K+ | Features |
|---|---|
| 3.0-3.5 | Often asymptomatic; minor ECG changes (U waves), mild fatigue |
| 2.5-3.0 | Muscle weakness, cramps, constipation, ventricular ectopy |
| <2.5 | Generalized muscle weakness, torsades de pointes, rhabdomyolysis, ascending paralysis |
| <2.0 | Respiratory muscle weakness, potentially fatal arrhythmias |
ECG changes in Hypokaemia:
- Flattening/inversion of T waves
- Prominent U waves (most characteristic - appears after the T wave)
- ST depression
- Prolonged QU interval
- Risk of torsades de pointes (particularly if also taking QT-prolonging drugs)
Other effects:
- Renal: Nephrogenic DI (polyuria/polydipsia), metabolic alkalosis, hypokalemic nephropathy
- GI: Ileus, constipation
- Metabolic: Impaired insulin secretion, altered glucose homeostasis
- Hypomagnesemia is commonly concurrent and causes refractory hypokalemia - must replace Mg2+ first
Treatment of Hypokalemia
| Severity | Treatment |
|---|---|
| K+ 3.0-3.5 (mild, asymptomatic) | Dietary K+ increase (bananas, oranges, potatoes); oral KCl 40-100 mEq/day |
| K+ 2.5-3.0 (moderate) | Oral KCl; if unable to take orally, IV KCl |
| K+ <2.5 or symptomatic | IV KCl; max infusion rate 10-20 mEq/hr (40 mEq/hr only in severe with continuous cardiac monitoring) - NEVER bolus IV potassium |
| Concurrent hypomagnesemia | Replace Mg2+ first (IV MgSO4); otherwise K+ replacement will fail |
Preferred salt: KCl (potassium chloride) in most patients; potassium citrate/bicarbonate in patients with metabolic acidosis or renal stones
Potassium-sparing diuretics (spironolactone, eplerenone, amiloride, triamterene): Add to thiazide/loop diuretics to prevent ongoing K+ wasting.
National Kidney Foundation Primer, 8th Ed; Comprehensive Clinical Nephrology, 7th Ed
HYPERKALEMIA (K+ > 5.0 mEq/L)
Definition & Risk
Hyperkalemia is uncommon in healthy individuals (< 1% prevalence) due to potent renal excretion mechanisms. Chronic hyperkalemia should always raise suspicion for impaired renal K+ excretion.
Severity classification:
- Mild: 5.0-5.9 mEq/L
- Moderate: 6.0-6.4 mEq/L
- Severe: ≥ 6.5 mEq/L
Causes
1. PSEUDOHYPERKALEMIA (Spurious - no true elevation)
- Hemolysis during blood draw (most common cause of elevated K+ on labs!)
- Severe leukocytosis (WBC >70,000) or thrombocytosis (platelets >500-1000 × 10⁹/L)
- Prolonged tourniquet time, fist clenching
- Diagnosis: Plasma K+ is >0.3 mmol/L lower than simultaneous serum K+
- Always repeat with atraumatic draw before treating
2. TRANSCELLULAR SHIFT (extracellular shift)
- Acidosis (metabolic > respiratory)
- Insulin deficiency / DKA (hypertonicity + insulin lack)
- Beta-blockade
- Digitalis toxicity (inhibits Na-K-ATPase)
- Hyperkalemic periodic paralysis (rare)
- Massive cell destruction: rhabdomyolysis, tumor lysis syndrome, severe hemolysis, massive blood transfusion, crush injuries, burns
3. INCREASED INTAKE (rarely causes persistent hyperkalemia alone)
- IV potassium excess
- K+-containing salt substitutes
- Blood transfusions
4. DECREASED RENAL EXCRETION (the most common cause of sustained hyperkalemia)
- CKD/ESRD (primary cause)
- Hypoaldosteronism: Addison's disease, hyporeninemic hypoaldosteronism (type 4 RTA in diabetic nephropathy)
- Drugs blocking K+ excretion: ACE inhibitors, ARBs, potassium-sparing diuretics (spironolactone, eplerenone, amiloride), NSAIDs, heparin, trimethoprim-sulfamethoxazole
- Obstructive uropathy
ECG Changes in Hyperkalemia (Most Important Feature)
ECG changes are the key to clinical management and represent a medical emergency:
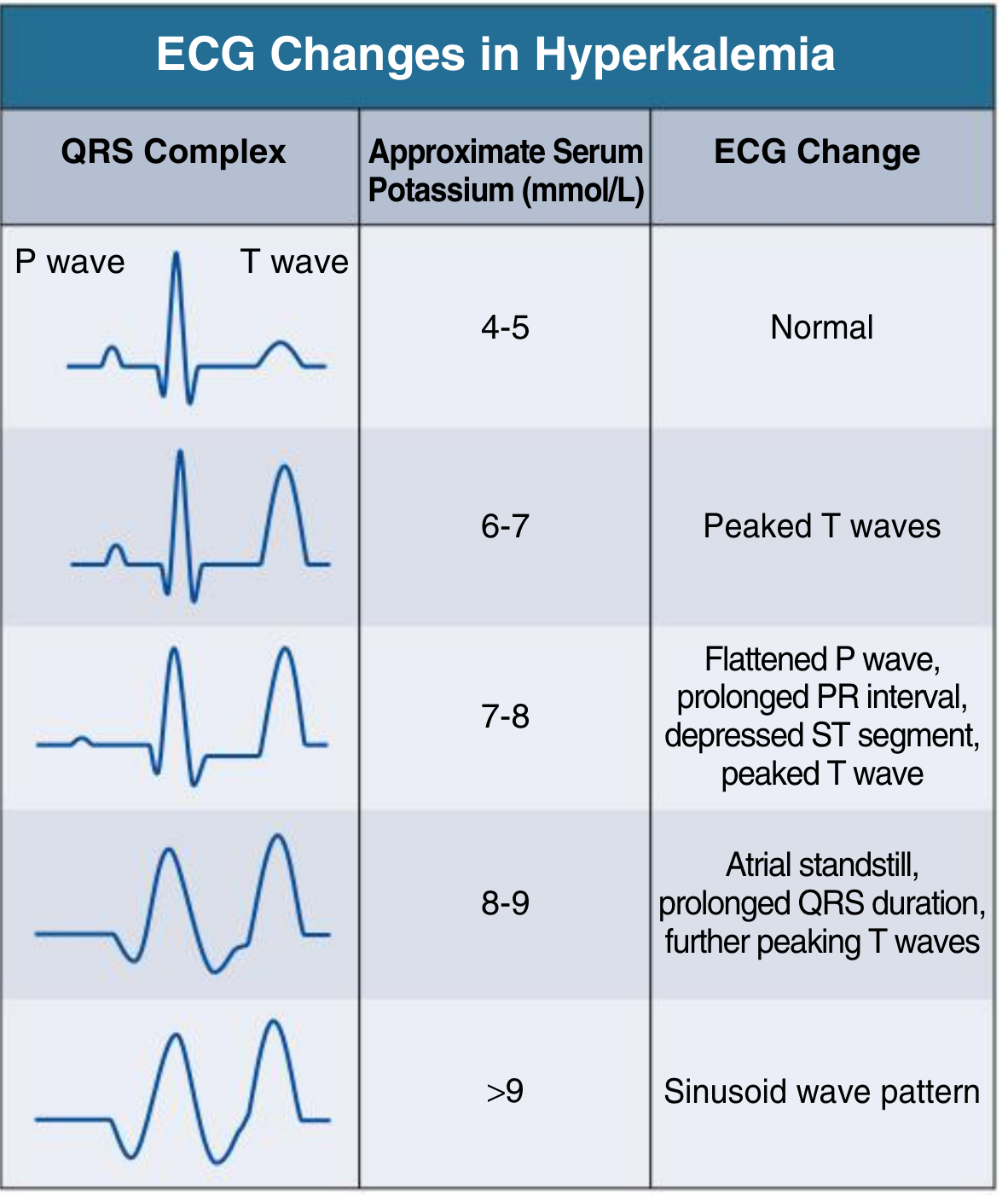
Electrocardiographic Changes in Hyperkalemia - Comprehensive Clinical Nephrology, 7th Ed
| Serum K+ (mEq/L) | ECG Change |
|---|---|
| 4-5 | Normal |
| 5-6 | Tall, peaked ("tented") T waves - first sign |
| 6-7 | Peaked T waves; PR prolongation |
| 7-8 | Flattened P waves, widened QRS, depressed ST |
| 8-9 | Absent P waves (atrial standstill), further QRS widening |
| >9 | Sine wave pattern → Ventricular fibrillation → cardiac arrest |
The ECG provides the urgency signal for treatment. ECG changes can precede symptoms and do not always correlate linearly with serum K+ levels.
Non-cardiac effects: Generalized muscle weakness, ascending paralysis, and in severe cases, diaphragmatic weakness causing respiratory failure.
Evaluation of Hyperkalemia
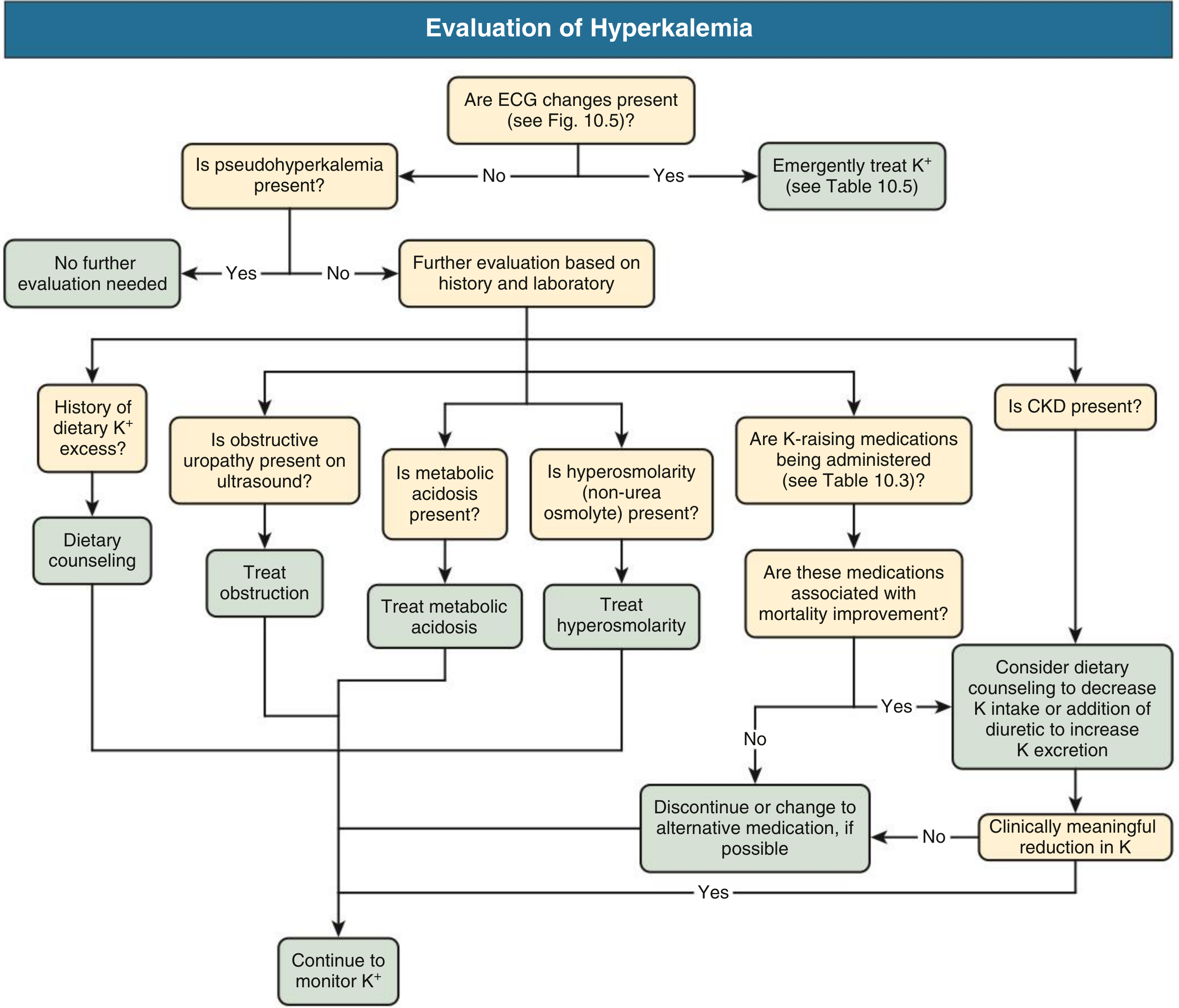
Fig. Workup of hyperkalemia - Comprehensive Clinical Nephrology, 7th Ed
Treatment of Hyperkalemia
Treatment has three sequential goals:
Stage 1: Cardiac Membrane Stabilization (FASTEST - acts in minutes)
IV Calcium Gluconate (10 mL of 10% solution over 2-3 min)
- Mechanism: Raises action potential threshold, restores normal excitability
- Onset: 1-3 minutes; Duration: 30-60 minutes
- Does NOT lower K+ - only protects the heart while you lower K+
- Caution: Potentiates digoxin toxicity - dilute and infuse slowly over 20-30 min if patient is on digoxin
- Repeat if no ECG improvement or if ECG changes recur
Stage 2: Redistribute K+ Into Cells (30-60 min to act)
| Drug | Dose | Mechanism | Onset | Duration |
|---|---|---|---|---|
| Insulin + Dextrose | 10 U regular insulin IV + 50 mL D50W (25g glucose) | Activates Na-K-ATPase | 10-20 min | 4-6 hrs |
| Nebulized Albuterol | 10-20 mg nebulized over 10 min | Beta-2 stimulation → cellular K+ uptake | 30 min | 2-6 hrs |
| NaHCO3 | 150 mEq in 1L D5W infused over hours | Corrects acidosis (adjunct only) | Hours | Several hours |
- Insulin + glucose is the first-line redistributive treatment
- Albuterol and insulin have additive effects; ~20% of ESRD patients are resistant to albuterol alone
- Bicarbonate has no role in acute treatment but may help in metabolic acidosis over hours
- Follow glucose closely after insulin - hypoglycemia is common; use D10W infusion at 50-75 mL/hr after bolus
Stage 3: Remove K+ From the Body
| Method | Notes |
|---|---|
| Loop diuretics (furosemide) | If renal function allows; promotes kaliuresis |
| Sodium polystyrene sulfonate (Kayexalate) | Cation exchange resin; onset hours; enteral |
| Patiromer (newer) | K+-binding resin; well tolerated; oral; chronic use |
| Sodium zirconium cyclosilicate (ZS-9) | Newer selective K+ exchanger; rapid onset (~1 hr) |
| Dialysis (hemodialysis) | Fastest and most reliable removal; for severe/refractory or ESRD |
Harrison's Principles of Internal Medicine 22E; Comprehensive Clinical Nephrology, 7th Ed
Summary Comparison Table
| Feature | Hyponatremia | Hypernatremia | Hypokalemia | Hyperkalemia |
|---|---|---|---|---|
| Definition | Na+ <136 | Na+ >144 | K+ <3.5 | K+ >5.0 |
| Key mechanism | Water excess or Na+ loss | Water deficit | Losses / shifts / intake | Impaired excretion / shifts |
| Pathophysiology | Brain cell swelling (↓ osmolality) | Brain cell shrinkage (↑ osmolality) | RMP more negative → hyperpolarization | RMP less negative → depolarization blockade |
| Main symptoms | Headache, confusion, seizures, coma | Thirst, confusion, seizures, coma | Weakness, cramps, arrhythmias | Weakness, ECG changes, VF/arrest |
| Key lab | Measure plasma osmolality + urine Na+ | Urine osmolality, urine Na+, ADH | Urine K+, Mg2+, pH, aldosterone | ECG, plasma vs serum K+, aldosterone |
| Most feared complication | Cerebral edema (acute); ODS if overcorrected | Cerebral hemorrhage (bridging vein rupture) | Torsades de pointes, paralysis | Ventricular fibrillation |
| Rate of correction | Max 8-10 mEq/L per 24 hrs | Max 10-12 mEq/L per 24 hrs | Gradual (IV max 20 mEq/hr) | Urgent if ECG changes |
| Emergency Rx | 3% hypertonic saline (acute + symptomatic) | D5W / 0.45% NS; free water orally | IV KCl (with monitoring) | IV Ca-gluconate → insulin/dextrose → dialysis |
Key Mnemonics for MBBS Exams
Causes of SIADH - "SIADH":
- S - Surgery / SSRIs
- I - Intracranial (meningitis, SAH, stroke)
- A - Acute respiratory (TB, pneumonia)
- D - Drugs (carbamazepine, cyclophosphamide, morphine)
- H - Hormones / Hypothyroid / Hypoadrenalism / Hemorrhage
Causes of Hyperkalemia - "RAID":
- R - Renal failure / Redistribution (acidosis)
- A - Addison's disease (hypoaldosteronism)
- I - Intake excess / Iatrogenic / drugs (ACEi, ARB, K-sparing diuretics)
- D - Destruction of cells (rhabdo, tumor lysis, hemolysis)
Hyperkalemia ECG progression (ascending K+):
- "TPAQSV" - T peaked → P flattened → QRS widened → Atrial standstill → Sine wave → Ventricular fibrillation
Sources: Goldman-Cecil Medicine International Edition; Harrison's Principles of Internal Medicine 22E (2025); Comprehensive Clinical Nephrology 7th Ed; National Kidney Foundation Primer on Kidney Diseases 8th Ed; Tietz Textbook of Laboratory Medicine 7th Ed; Medical Physiology (Boron & Boulpaep); Brenner & Rector's The Kidney
Please continue writing
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the content needed for a thorough continuation. Here is the detailed continuation:
CONTINUATION: Deeper Clinical Coverage
PART 3: ADVANCED CLINICAL DETAILS - HYPONATREMIA
The Adrogue-Madias Formula (Infusate Effect on Serum Na+)
When treating hyponatremia with any IV fluid, this formula estimates how much each liter of infusate will change the serum Na+:
Change in serum [Na+] per liter of infusate = (Infusate [Na+] - Serum [Na+]) / (TBW + 1)
| Infusate | Na+ Content (mEq/L) |
|---|---|
| 3% NaCl (hypertonic saline) | 513 |
| 0.9% NaCl (normal saline) | 154 |
| Ringer's Lactate | 130 |
| 0.45% NaCl (half normal) | 77 |
| D5W (5% dextrose in water) | 0 (free water) |
Example: Patient with serum Na+ = 115, TBW = 35 L (70 kg man × 0.5 due to illness)
- Using 3% NaCl: change per liter = (513 - 115) / (35 + 1) = 398/36 = +11 mEq/L per liter
- To raise Na+ by 5 mEq, you need: 5/11 = ~0.45 L = 450 mL of 3% NaCl
Practical point: This formula underestimates the actual rise because it does not account for ongoing free water excretion as ADH is suppressed. Monitor serum Na+ every 2 hours during active correction.
Comprehensive Clinical Nephrology, 7th Ed
Treatment Protocol for Hyponatremia - Step by Step
Acute Symptomatic Hyponatremia (<48 hrs, with seizures/coma)
- Bolus 100 mL of 3% NaCl IV over 10 minutes - can repeat ×2 (total up to 300 mL) until seizures stop
- Target: raise Na+ by 4-6 mEq/L in first 6 hours (enough to reverse cerebral edema)
- Then slow the rate to stay within 8-10 mEq/L per 24 hours
- Add furosemide to enhance free water excretion if needed
Chronic Asymptomatic or Mildly Symptomatic Hyponatremia
| Treatment Option | Mechanism | Dose | Notes |
|---|---|---|---|
| Fluid restriction | Reduces free water intake | 500-800 mL/day | First line for SIADH; cheap, effective |
| 0.9% NaCl | Volume replacement | Guided by deficit | Only for hypovolemic hyponatremia |
| Demeclocycline | Induces nephrogenic DI (blocks ADH at tubule) | 300-600 mg twice daily | Chronic SIADH; risk nephrotoxicity, photosensitivity |
| Tolvaptan (V2 antagonist, oral) | Aquaresis - free water excretion without Na+ loss | 15 mg daily; titrate up | SIADH, CHF, cirrhosis; do NOT use >30 days (hepatotoxicity) |
| Conivaptan (V1a + V2 antagonist, IV) | Aquaresis | 20 mg IV loading, then infusion | Hospital use only; SIADH |
| Urea | Osmotic diuresis | 15-60 g/day orally | Alternative to vaptans; cheap |
| Salt tablets + fluid restriction | Direct Na+ supplementation | 2-3 g salt tablets | Low urine Osm patients |
Treating underlying cause is always primary:
- CHF: ACE inhibitors, diuretics, optimizing cardiac output
- Hypothyroidism: Levothyroxine
- Adrenal insufficiency: Glucocorticoids/mineralocorticoids (correct first - giving saline before cortisol can cause dangerous over-correction)
- SIADH: Remove offending drugs, treat infection/malignancy
Cerebral Salt Wasting (CSW) vs. SIADH - Critical Distinction
Both cause euvolemic-appearing hyponatremia with elevated urine Na+. Clinically important because their treatments are opposite:
| Feature | SIADH | Cerebral Salt Wasting |
|---|---|---|
| Setting | Many causes | Primarily subarachnoid hemorrhage, TBI, neurosurgery |
| Mechanism | Inappropriate ADH → water retention | Brain natriuretic peptide → renal Na+ wasting → volume contraction → secondary ADH |
| Volume status | Euvolemic (clinically) | Hypovolemic (key difference) |
| BUN/Creatinine | Low (diluted) | Normal to slightly elevated |
| Uric acid | Low | Low |
| Urine Na+ | High (>40) | High (>40) |
| Treatment | FLUID RESTRICTION | IV saline (volume replacement + Na+ replacement) |
Treating CSW with fluid restriction (as you would SIADH) will worsen hypovolemia and cause cerebral vasospasm in SAH - potentially catastrophic. Always assess volume status carefully.
Comprehensive Clinical Nephrology, 7th Ed; Bradley & Daroff's Neurology in Clinical Practice
Special Populations: Hyponatremia
Exercise-Associated Hyponatremia (EAH):
- Common in marathon runners, military recruits
- Caused by excessive hypotonic fluid intake during prolonged exercise
- Compounded by non-osmotic ADH release (pain, nausea, stress)
- Can be rapidly fatal from cerebral herniation
- Treatment: Hypertonic saline (3%) - even in field settings if severe
Post-operative Hyponatremia:
- Hypotonic IV fluids + non-osmotic ADH release from pain/stress/nausea
- Pre-menopausal women and children at highest risk
- Prevention: use isotonic (0.9% NaCl) for routine IV fluid replacement
Beer Potomania / Tea-and-Toast Syndrome:
- Extremely low dietary solute intake (malnourished patients, heavy beer drinkers)
- Kidneys cannot generate enough urine to excrete free water without solute
- Even normal water intake dilutes Na+
- Treatment: Increase dietary solutes; fluid restriction
PART 4: ADVANCED CLINICAL DETAILS - HYPERNATREMIA
Diagnostic Algorithm for Hypernatremia
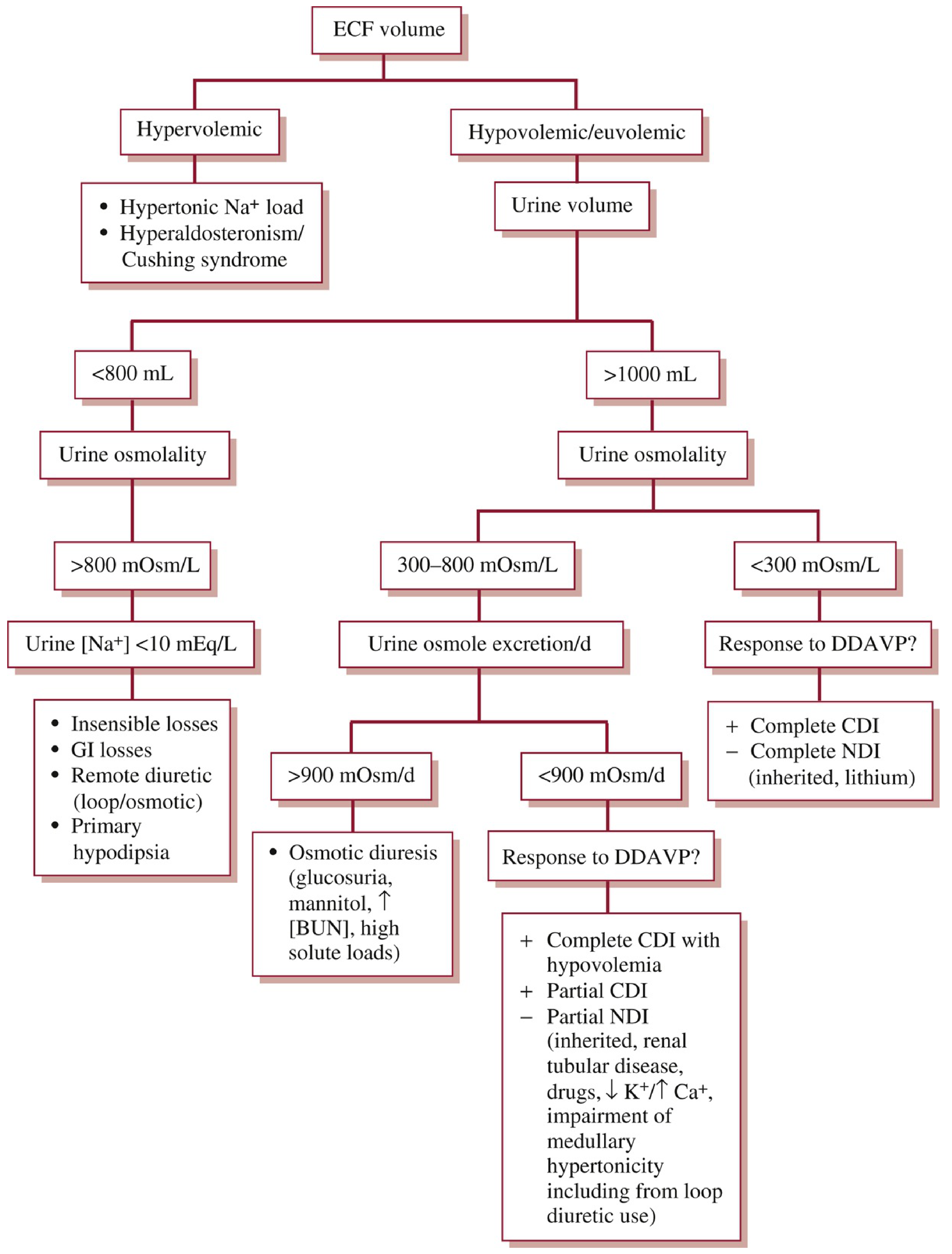
Fig. Diagnostic approach to hypernatremia - Washington Manual of Medical Therapeutics
Interpretation of urine osmolality in hypernatremia:
| Urine Osm | Diagnosis |
|---|---|
| >800 mOsm/L | Normal renal response - extrarenal water loss (GI, insensible, skin), or primary hypodipsia |
| 300-800 mOsm/L | Partial DI, or osmotic diuresis (check 24-hr urine osmoles: if >900 mOsm/day = osmotic diuresis) |
| <300 mOsm/L + DDAVP response + | Central DI |
| <300 mOsm/L + DDAVP no response - | Nephrogenic DI |
Central DI vs. Nephrogenic DI - Deep Dive
Water Deprivation Test:
- Withhold water for 4-18 hours (under supervision)
- Measure urine osmolality hourly
- When urine Osm plateaus (or weight drops 3-5%), administer DDAVP (10 mcg intranasal)
- Measure urine Osm 1-2 hours after DDAVP
| Result | Diagnosis |
|---|---|
| Urine Osm >800 after deprivation alone | Normal (primary polydipsia or reset osmostat) |
| Urine Osm rises >50% after DDAVP | Central DI |
| Urine Osm rises <10% after DDAVP | Nephrogenic DI |
| Intermediate rise (10-50%) | Partial central or nephrogenic DI |
Treatment of Nephrogenic DI:
| Drug | Mechanism |
|---|---|
| Thiazide diuretics (paradoxical) | Volume contraction → proximal Na+/water reabsorption → less water delivered distally |
| Low Na+ / low protein diet | Reduces urine solute load, less obligate water loss |
| NSAIDs (indomethacin) | Reduce prostaglandin-mediated inhibition of ADH in tubule |
| Amiloride | Specifically for lithium-induced NDI - blocks lithium entry into collecting duct cells |
| DDAVP | Useless in complete NDI; may help partial NDI |
Hypernatremia Treatment - Full Protocol
Correction Rate: Max 0.5 mEq/L/hr (or 10-12 mEq/L per day) for chronic hypernatremia. For acute sodium loading, up to 1 mEq/L/hr may be safer.
Step-by-step approach:
- Hemodynamic instability first: Give 0.9% NaCl to restore circulating volume (even though it contains Na+, the priority is perfusion)
- Calculate free water deficit: TBW × [(actual Na+ / 140) - 1]
- Add ongoing losses (insensible, urine, GI) to daily replacement needs
- Choose fluid:
- D5W: delivers pure free water (used when Na+ balance is positive or normal)
- 0.45% NaCl: half isotonic; used when some Na+ replacement also needed
- Oral/enteral water: safest and easiest to titrate in conscious patients
- Monitor serum Na+ every 4-6 hours during active correction
- Treat the cause: DDAVP for central DI; thiazide + low-solute diet for nephrogenic DI; stop offending drugs
Total Body Water Fractions by Population:
| Population | TBW Fraction |
|---|---|
| Children + adult men | 0.6 × weight (kg) |
| Adult women | 0.5 × weight (kg) |
| Elderly men | 0.5 × weight (kg) |
| Elderly women | 0.45 × weight (kg) |
Washington Manual of Medical Therapeutics; National Kidney Foundation Primer, 8th Ed
PART 5: ADVANCED CLINICAL DETAILS - HYPOKALEMIA
Renal vs. Extra-renal Loss - Diagnostic Approach
Transtubular Potassium Gradient (TTKG):
TTKG = (Urine K+ / Plasma K+) / (Urine Osm / Plasma Osm)
| TTKG | Interpretation |
|---|---|
| >4 (in hypokalemia) | Renal K+ wasting (inappropriate renal losses) |
| <2 (in hypokalemia) | Extra-renal losses (GI, skin, inadequate intake) |
Simpler rule - Urine K+:
- Random urine K+ >20-25 mEq/L = renal losses
- Random urine K+ <20 mEq/L = extra-renal losses
Causes of Hypokalemia with Hypertension
This is a classic MBBS exam scenario:
| Condition | Aldosterone | Renin | Other Features |
|---|---|---|---|
| Primary hyperaldosteronism (Conn's) | High | Low | Most common cause; adrenal adenoma or hyperplasia; MRI adrenals |
| Secondary hyperaldosteronism (RAS, RVH, renin-secreting tumor) | High | High | Renovascular hypertension |
| Cushing's syndrome (cortisol excess) | High | Low | Central obesity, striae, buffalo hump; cortisol has mineralocorticoid activity |
| Liddle syndrome (gain-of-function ENaC) | Low | Low | Genetic; pseudohyperaldosteronism; treat with amiloride |
| Apparent mineralocorticoid excess (11β-HSD2 deficiency) | Low | Low | Licorice ingestion (glycyrrhizin) inhibits 11β-HSD2; carbenoxolone |
| Glucocorticoid-remediable aldosteronism | High | Low | Familial; aldosterone production driven by ACTH; responds to dexamethasone |
Hypokalemic Periodic Paralysis - Full Picture
A clinically tested topic in MBBS:
Types:
| Type | Gene Mutation | Trigger | K+ during attack | Notes |
|---|---|---|---|---|
| Familial HypoPP Type 1 | CACNA1A (L-type Ca channel) | Carbohydrate meal, rest after exercise, cold | Very low (<2) | Autosomal dominant; treat with K+ supplementation |
| Familial HypoPP Type 2 | SCN4A (skeletal Na channel) | Same as above | Very low | |
| Thyrotoxic PP (TPP) | Kir2.6 / KCNJ2 | Carbohydrate, stress, exertion | Very low | Asian males (90%), non-inherited; treat hyperthyroidism + propranolol (3 mg/kg); K+ replacement cautiously |
| Hyperkalemic PP | SCN4A (gain-of-function) | Fasting, rest after exercise, cold | High/normal | Shorter attacks; Mexiletine for prophylaxis |
Clinical features of attack:
- Acute onset of proximal > distal flaccid weakness, especially lower limbs
- Usually begins in early morning after large carbohydrate meal
- Bulbar, ocular, and respiratory muscles usually spared
- ECG shows hypokalemia changes: flat/inverted T waves, prominent U waves, prolonged QU interval
- Resolves spontaneously or with K+ replacement
Caution in TPP: Total body K+ is NOT depleted - K+ has merely shifted intracellularly. Overzealous replacement causes rebound hyperkalemia after thyroid treatment. Give IV K+ sparingly (10 mEq boluses, not rapid large doses).
Rosen's Emergency Medicine; Harrison's Principles of Internal Medicine 22E
Magnesium and Potassium: The Critical Link
Hypomagnesemia is one of the most commonly missed causes of refractory hypokalemia. It must always be checked and corrected before attempting K+ repletion.
Mechanism: Mg2+ is required for Na-K-ATPase function and for keeping K+ inside cells. It also suppresses the ROMK channel (responsible for tubular K+ secretion) in the thick ascending limb. Without Mg2+, urinary K+ wasting continues regardless of how much K+ you give.
Rule: If a patient's K+ fails to correct despite IV replacement, check and replace Mg2+ (IV MgSO4).
PART 6: ADVANCED CLINICAL DETAILS - HYPERKALEMIA
Drug-Induced Hyperkalemia - Comprehensive List
Understanding which drugs raise K+ is essential clinically:
| Drug Class | Mechanism |
|---|---|
| ACE inhibitors / ARBs | Block angiotensin II → reduce aldosterone → reduce tubular K+ secretion |
| Potassium-sparing diuretics (spironolactone, eplerenone) | Block aldosterone receptor → same as above |
| Amiloride, triamterene | Block ENaC directly → reduce K+ secretion |
| NSAIDs | Reduce prostaglandin → reduce renin → reduce aldosterone |
| Heparin | Directly inhibits aldosterone synthesis |
| Trimethoprim (high-dose) | Blocks ENaC (like amiloride) |
| Beta-blockers | Block beta-2 → prevent cellular K+ uptake |
| Digoxin (toxic levels) | Inhibits Na-K-ATPase → K+ leaks out of cells |
| Succinylcholine | Triggers massive K+ efflux from muscle (dangerous in burns, crush, denervation, prolonged immobility) |
| Cyclosporine / Tacrolimus | Reduce aldosterone activity |
| Penicillin G (high-dose potassium salt) | Direct K+ load |
New Oral Potassium Binders
These agents have largely replaced the old Kayexalate for chronic hyperkalemia management:
| Agent | Mechanism | Onset | Key Use |
|---|---|---|---|
| Patiromer (Veltassa) | Ca2+-sorbitol cation exchanger; binds K+ in colon | 6-7 hours | Chronic hyperkalemia in CKD, HF; cannot use in emergencies |
| Sodium Zirconium Cyclosilicate (Lokelma/SZC) | Selective ion exchanger; binds K+ in gut (all segments) | ~1 hour (fastest oral agent) | Both acute and chronic settings; reduces K+ >6.0 to <5.5 in median 4 hours |
| Sodium Polystyrene Sulfonate (Kayexalate) | Exchanges Na+ for K+ in colon | Unpredictable | No longer recommended for emergency use due to risk of colonic necrosis |
Barash Clinical Anesthesia, 9th Ed; National Kidney Foundation Primer, 8th Ed
Hyperkalemia in Special Settings
Diabetic Ketoacidosis (DKA) and Potassium:
- On presentation: serum K+ is often NORMAL or HIGH despite massive total body K+ deficit
- This is because: insulin deficiency + hypertonicity shift K+ from ICF to ECF
- As you treat DKA with insulin + fluids: K+ rapidly drops → can cause dangerous hypokalemia
- Rule: Start K+ replacement when serum K+ falls below 5.0 mEq/L, and MUST replace before insulin if K+ < 3.5
Tumor Lysis Syndrome (TLS):
- Massive cell destruction (chemotherapy for lymphoma, leukemia, bulky tumors)
- Releases K+, phosphate, uric acid, and nucleic acids
- Classic biochemical triad: hyperkalemia + hyperphosphatemia + hypocalcemia + hyperuricemia
- Can lead to fatal arrhythmia from hyperkalemia
- Prevention: aggressive hydration + allopurinol or rasburicase before chemotherapy
Rhabdomyolysis:
- Massive muscle breakdown → K+ release + myoglobin → AKI (which worsens hyperkalemia further)
- Other electrolytes: hyperphosphatemia, hypocalcemia (early), hypercalcemia (late recovery)
- Treatment: aggressive IV hydration (target urine output >200-300 mL/hr), urinary alkalinization
Succinylcholine-Induced Hyperkalemia:
- In normal patients, succinylcholine raises K+ by only ~0.5-1.0 mEq/L (acceptable)
- In denervated muscle (burns, crush injury, spinal cord injury, prolonged ICU stay, stroke): massive K+ efflux can cause K+ to rise by 5-10 mEq/L → cardiac arrest
- Contraindicated in these conditions; use non-depolarizing NMBAs instead
PART 7: PHYSIOLOGY DEEP DIVE - Why These Electrolytes Matter
Sodium and Osmolality - The Core Concept
Sodium is the main determinant of plasma osmolality:
Plasma Osmolality = 2 × Na+ + (Glucose/18) + (BUN/2.8)
Normal = 280-295 mOsm/kg. Sodium accounts for ~90% of ECF osmolality.
Osmoreceptors in the hypothalamus (OVLT neurons) detect a rise in osmolality as small as 1-2 mOsm/kg and:
- Trigger ADH (vasopressin) release from posterior pituitary → water retention in collecting duct (V2 receptors → aquaporin-2 insertion)
- Stimulate thirst → water intake
Baroreceptors in the carotid sinus and aorta detect volume changes and:
- Trigger renin-angiotensin-aldosterone system → Na+ (and water) retention
- Provide a non-osmotic stimulus for ADH release (takes priority over osmolality in severe volume depletion)
Potassium and the Resting Membrane Potential - Why K+ Changes Are Dangerous
The resting membrane potential (RMP) of most cells is approximately -90 mV and is primarily determined by the ratio of intracellular to extracellular K+:
RMP ≈ -61 × log([K+]i / [K+]e) (Nernst equation)
In Hypokalemia (low extracellular K+):
- The K+ gradient becomes steeper → RMP becomes more negative (hyperpolarized), e.g., -100 mV
- Cell is harder to excite - threshold is harder to reach
- Paradoxically, this causes: reduced excitability of skeletal muscle (weakness), but also increased excitability of cardiac conduction tissue and pacemaker cells
- Clinical result: U waves on ECG, torsades de pointes, ventricular fibrillation
In Hyperkalemia (high extracellular K+):
- K+ gradient narrows → RMP becomes less negative (depolarized), e.g., -70 mV
- Cell is initially more excitable, then undergoes depolarization blockade (Na+ channels are inactivated)
- Clinical result: peaked T waves → widened QRS → loss of P waves → sine wave → VF
- Skeletal muscle: weakness and flaccid paralysis (depolarization blockade)
PART 8: EXAM-FOCUSED HIGH-YIELD POINTS
Most Commonly Tested Exam Facts
Hyponatremia:
- Most common electrolyte disorder in hospitalized patients
- First step in workup: measure plasma osmolality
- Most common cause of SIADH: small cell lung cancer (ectopic ADH), and drugs (SSRIs)
- Rate of correction: never exceed 8-10 mEq/L in 24 hours (risk ODS/CPM)
- Overcorrection treatment: give free water (D5W) or DDAVP to re-lower Na+ if correction was too fast
Hypernatremia:
- Always reflects free water deficit (not sodium excess, usually)
- Always accompanied by hypertonicity
- Symptoms = brain cell shrinkage (opposite of hyponatremia)
- Key formula: Free water deficit = TBW × [(Na+ / 140) - 1]
- Must correct hemodynamic instability with 0.9% NaCl FIRST, then address water deficit
Hypokalemia:
- Most common cause: loop and thiazide diuretics
- Always check and replace Mg2+ - hypomagnesemia causes refractory hypokalemia
- Never give IV K+ as bolus - max infusion 10-20 mEq/hr
- Danger: K+ < 2.5 → torsades de pointes, rhabdomyolysis
- DKA treatment: watch K+ fall as insulin drives it intracellularly
Hyperkalemia:
- Most common spurious cause: hemolysis during blood draw
- Most common true cause: CKD / impaired renal excretion
- ECG is your urgency guide - presence of ECG changes = medical emergency
- First treatment: IV Calcium gluconate (cardiac protection, does not lower K+)
- Second: Insulin + dextrose (shifts K+ in, fastest acting)
- Third: Remove K+ - dialysis is the most reliable and definitive
Quick Comparison: ECG Changes
| Disorder | ECG Findings |
|---|---|
| Hypokalemia | Flattened/inverted T waves, prominent U waves, ST depression, prolonged QU interval |
| Hyperkalemia | Tall peaked T waves → PR prolongation → wide QRS → absent P → sine wave → VF |
| Hyponatremia | Non-specific (rarely causes primary ECG changes; effects are neurological) |
| Hypernatremia | Non-specific; may see tachycardia from volume depletion |
One-Line High-Yield Associations for MCQs
| Clinical Clue | Diagnosis |
|---|---|
| SAH + hyponatremia + hypovolemia | Cerebral salt wasting |
| SCLC + hyponatremia + no edema + urine Na >40 | SIADH |
| Hypertension + hypokalemia + low renin + high aldo | Primary hyperaldosteronism (Conn's) |
| Asian male + hypokalemia + acute weakness + high T4 | Thyrotoxic periodic paralysis |
| Lithium use + polyuria + hypernatremia + no DDAVP response | Nephrogenic DI |
| DKA treatment → falling K+ | Insulin driving K+ intracellularly - replace K+ |
| Hemolyzed sample + "high K+" | Pseudohyperkalemia - repeat test |
| Rapid correction of chronic hyponatremia → quadriplegia | Osmotic demyelination syndrome (CPM) |
| Burns/crush injury patient + succinylcholine → cardiac arrest | Hyperkalemia from succinylcholine |
| Chemotherapy + high K+, high PO4, low Ca2+ | Tumor lysis syndrome |
| Licorice excess + hypertension + hypokalemia + low renin + low aldo | Apparent mineralocorticoid excess |
| Marathon runner drinking excessive water → hyponatremia | Exercise-associated hyponatremia |
Sources used throughout this guide:
- Goldman-Cecil Medicine International Edition, 2-Volume Set
- Harrison's Principles of Internal Medicine 22E (2025)
- Comprehensive Clinical Nephrology, 7th Edition
- National Kidney Foundation Primer on Kidney Diseases, 8th Edition
- Tietz Textbook of Laboratory Medicine, 7th Edition
- Medical Physiology (Boron & Boulpaep)
- Rosen's Emergency Medicine
- Washington Manual of Medical Therapeutics
- Brenner & Rector's The Kidney, 2-Volume Set
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Edition
- Bradley & Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.