What is anencephaly
Reading File
search_medical_text
anencephaly neural tube defect definition etiology pathophysiology
search_medical_image
anencephaly fetal neural tube defect
GradeResponse
GradeResponse
Anencephaly
Anencephaly is a lethal congenital neural tube defect (NTD) characterized by the absence of a major portion of the brain, skull, and scalp. It results from failure of the rostral (head) end of the neural tube to close during early embryonic development, typically by the 23rd–26th day after conception.
Pathophysiology
The neural tube normally closes by the 4th week of gestation. In anencephaly, the anterior neuropore fails to close, leading to:
- Absence of the cranial vault (acrania)
- Absence of the cerebral hemispheres (the brain tissue that does form is exposed and degenerates)
- Intact brainstem in most cases (which is why some reflexes are preserved)
Etiology & Risk Factors
| Factor | Details |
|---|---|
| Folic acid deficiency | Most important modifiable risk factor |
| Genetic factors | Mutations in folate metabolism genes (e.g., MTHFR); recurrence risk ~4–5% after one affected pregnancy |
| Maternal diabetes | Poorly controlled periconceptional diabetes increases NTD risk |
| Antiepileptic drugs | Valproate and carbamazepine are teratogenic NTD risks |
| Hyperthermia | Fever or hot tub use in early pregnancy |
| Race/ethnicity | Higher incidence in Hispanics; lower in Black populations |
Diagnosis
Prenatal:
- Maternal serum AFP (MSAFP): markedly elevated (open defect leaks AFP into amniotic fluid and maternal blood)
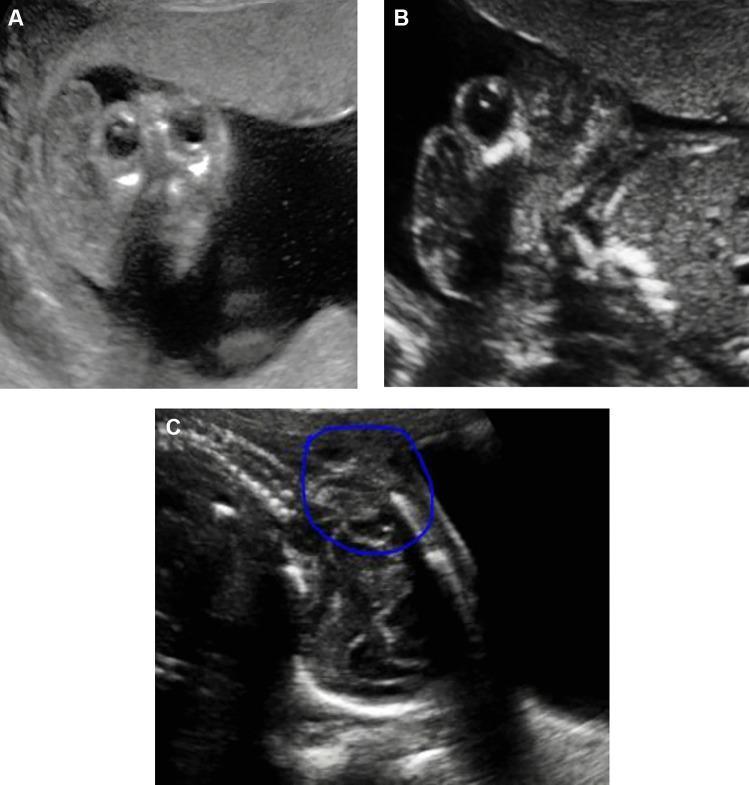
- Ultrasound: Diagnosis possible as early as 11–14 weeks; the classic sign is absence of the cranial vault and cerebral hemispheres with protruding orbits — the "frog-eye" or "Mickey Mouse" sign on coronal view
Postnatally:
- Clinical diagnosis: absence of the top of the skull and most brain tissue; the face is present but the head appears flattened
Clinical Features
- Polyhydramnios in ~50% of cases (due to impaired fetal swallowing from absent cortical control)
- Absent or rudimentary forebrain; brainstem may be intact
- Infants may have some primitive reflexes (sucking, response to pain) due to brainstem preservation
- Cannot maintain homeostasis or conscious functions
Prognosis
Anencephaly is universally fatal:
- Stillbirth in ~50% of cases
- Liveborn infants survive hours to days at most
- No curative treatment exists; care is palliative/comfort-oriented
Prevention
According to Harrison's Principles of Internal Medicine (p. 2951), folic acid supplementation at the time of conception and through the first 12 weeks of pregnancy reduces NTD incidence (including anencephaly) by approximately 70%. The recommended dose is 0.4 mg/day for the general population and 4 mg/day for women with a prior NTD-affected pregnancy.
Folic acid fortification of grains and cereals, mandatory in many countries since the 1990s, has significantly reduced the prevalence of anencephaly worldwide.
Epidemiology
- Incidence: approximately 1 in 1,000–2,000 pregnancies (varies by region and folic acid fortification status)
- More common in female fetuses (~3:1 female-to-male ratio)
- One of the most common causes of perinatal mortality from congenital anomalies
Diff between anencephaly and enancephaly
search_medical_text
encephalocele definition classification types
GradeResponse
search_medical_text
encephalocele neural tube defect brain herniation skull defect
GradeResponse
Here is a clear comparison. Note that "enancephaly" is not a standard medical term — you are likely referring to encephalocele, which is a related but distinct NTD.
Anencephaly vs. Encephalocele
| Feature | Anencephaly | Encephalocele |
|---|---|---|
| Definition | Absence of the cranial vault and cerebral hemispheres due to failure of the anterior neuropore to close | Herniation of brain tissue and/or meninges through a defect (gap) in the skull |
| Embryological defect | Anterior neuropore fails to close entirely | Incomplete fusion of the skull (cranium bifidum) after neural tube closure |
| Skull | Absent (acrania) — no cranial vault formed | Skull is present but has a focal defect/gap through which tissue protrudes |
| Brain tissue | Cerebral hemispheres absent; exposed brain degenerates | Brain may or may not herniate — if only meninges/CSF herniate, it is a meningocele; if brain substance herniates, it is an encephalocele |
| Location | Always involves the top/front of the skull | Most commonly occipital (75%); can also be frontal, parietal, or basal |
| Prognosis | Universally fatal (hours to days after birth) | Variable — depends on size, location, and how much brain tissue is involved; surgical repair is possible |
| Survival | None; lethal condition | Possible with surgery; neurological outcome varies widely |
| Associated findings | Polyhydramnios (~50%), frog-eye appearance | May be associated with hydrocephalus, microcephaly, other CNS anomalies |
| Prenatal diagnosis | Ultrasound: absent cranial vault ("Mickey Mouse" sign); elevated MSAFP | Ultrasound: sac-like protrusion through occipital bone; elevated MSAFP |
Key Conceptual Distinction
- Anencephaly: The neural tube never closed at the front — so the brain and skull simply never formed properly. It is a failure of formation.
- Encephalocele: The neural tube did close, but the skull did not fuse properly at one spot, creating a window through which brain tissue bulges out. It is a failure of containment.
Both are neural tube defects and share the same risk factors (folic acid deficiency, genetic predisposition, teratogen exposure), but anencephaly is invariably lethal while encephalocele carries a survivable prognosis in many cases — particularly small occipital encephaloceles without major brain tissue involvement.
According to Bailey and Love's Short Practice of Surgery (p. 740), this distinction maps directly onto the skull: the same spectrum seen in spinal dysraphism (meningocele → myelomeningocele) is replicated at the cranial level (meningocele → encephalocele), with anencephaly representing the most extreme end.
This is a shared conversation. Sign in to Orris to start your own chat.