Teach me leiomyomya for gyanecology mbbs level
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have enough rich content from Berek & Novak's Gynecology to write a comprehensive MBBS-level teaching note on leiomyoma. Let me compile everything.
Uterine Leiomyoma (Fibroids) - MBBS Gynecology
Source: Berek & Novak's Gynecology
1. Definition and Basic Science
Uterine leiomyomas (also called fibroids, myomas, or fibromyomas) are benign, monoclonal tumors of uterine smooth muscle cells (myometrium). They contain large aggregates of extracellular matrix composed of collagen, elastin, fibronectin, and proteoglycan.
- They are the most common benign tumors of the female genital tract
- The most frequent indication for hysterectomy (~240,000/year in the US)
- They are not premalignant - malignant transformation to leiomyosarcoma is very rare
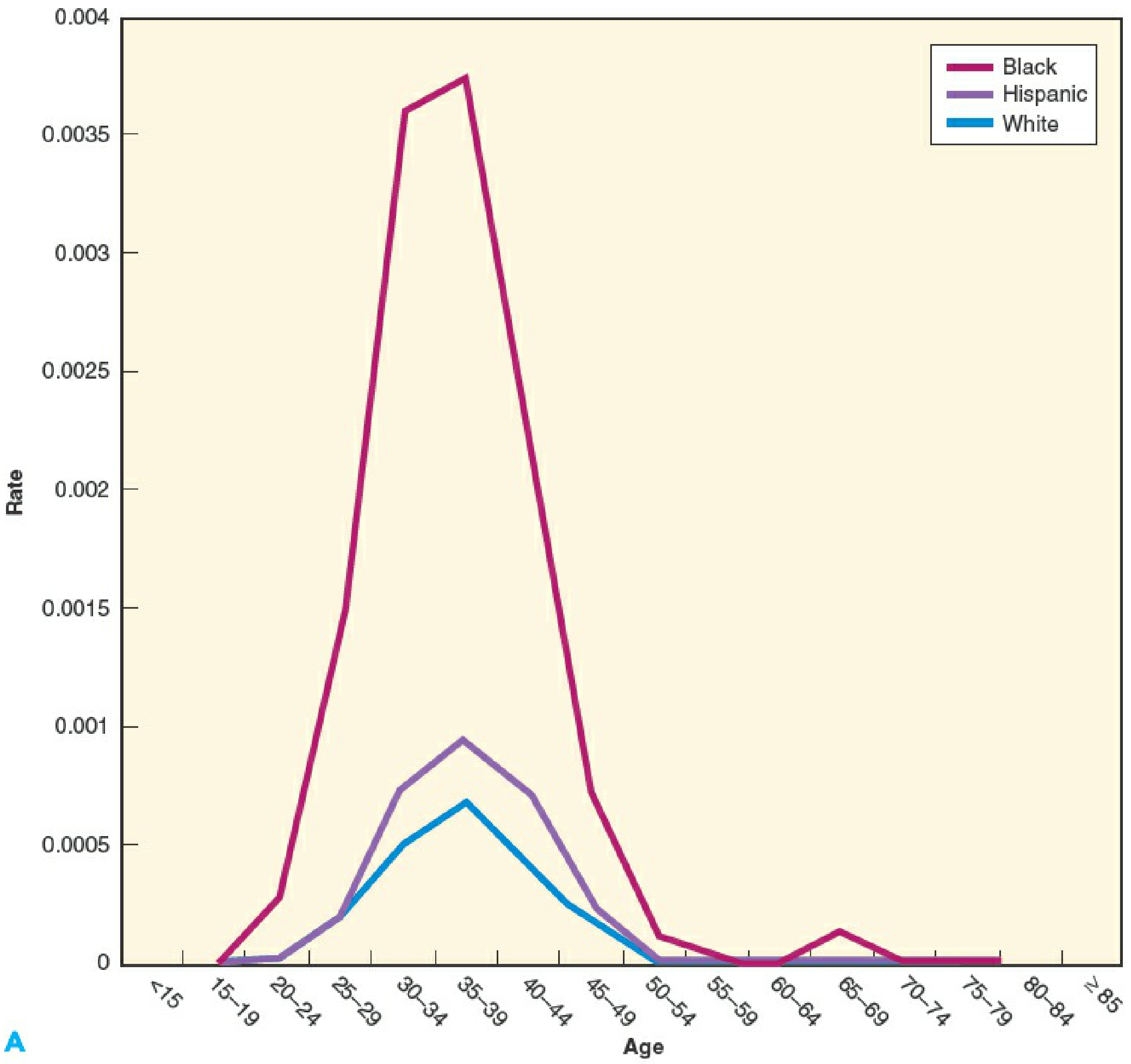
2. Incidence / Epidemiology
Fibroids are remarkably common:
| Population | By age 35 | By age 50 |
|---|---|---|
| African American women | 60% | >80% |
| White women | 40% | ~70% |
- Incidence rises with age: 4.3 per 1,000 woman-years at age 25-29, rising to 22.5 per 1,000 at age 40-44
- Never seen before puberty; regress after menopause
3. Pathogenesis / Etiology
Hormonal Role (KEY)
- Fibroids are estrogen and progesterone dependent
- Serum levels of both hormones are the same in women with and without fibroids, BUT:
- Fibroids have increased aromatase → higher local de novo estradiol production
- Fibroids have increased progesterone receptors A and B compared to normal myometrium
- Highest mitotic counts are found at the peak of progesterone production
- GnRH agonists shrink fibroids; concurrent progestins block this shrinkage
- The antiprogestin RU-486 (mifepristone) blocks fibroid growth
Growth Factors
Local growth factors stimulate fibroid growth by increasing extracellular matrix:
- TGF-β, bFGF → smooth muscle proliferation + ECM synthesis
- EGF, PDGF → increase DNA synthesis
- VEGF, bFGF → promote angiogenesis
4. Risk Factors
| Increases Risk | Decreases Risk |
|---|---|
| African American ethnicity | Smoking (reduces estrogen bioavailability) |
| Increasing age (reproductive years) | Increased parity |
| Early menarche (<10 years) | Exercise |
| Obesity | Late menarche |
| Family history (2.5x risk in 1st-degree relatives) | Oral contraceptives (no consistent effect) |
| Nulliparity | Menopause |
5. Classification by Location (FIGO System)
This is the FIGO fibroid classification - memorize the types:
| Type | Description |
|---|---|
| Type 0 | Intracavitary (pedunculated submucosal, entirely within cavity) |
| Type 1 | <50% diameter within myometrium (submucosal) |
| Type 2 | ≥50% diameter within myometrium (submucosal) |
| Type 3 | Abuts endometrium, no intracavitary component (intramural) |
| Type 4 | Entirely intramural, no extension to endometrium or serosa |
| Type 5 | Subserosal, ≥50% intramural |
| Type 6 | Subserosal, <50% intramural |
| Type 7 | Subserosal pedunculated (attached by stalk) |
| Type 8 | No myometrial involvement (cervical, broad ligament, "parasitic") |
Clinical shorthand:
- Submucosal (Types 0-2): bulge into uterine cavity → most likely to cause bleeding and infertility
- Intramural (Type 4): within muscle wall → most common type
- Subserosal (Types 5-7): project outward → cause pressure symptoms
6. Fibroid Variants (Gross Pathology)
Fibroids can undergo degeneration as they outgrow their blood supply:
| Type of Degeneration | Features |
|---|---|
| Hyaline | Most common; fibrous tissue replaces muscle |
| Cystic | Liquefaction of hyaline areas |
| Calcific | Calcium deposition; "womb stone" seen on X-ray |
| Red/Carneous | Hemorrhagic; seen in pregnancy - causes acute severe pain |
| Myxomatous | Gelatinous material |
| Sarcomatous | Very rare malignant change |
Exam pearl: Red degeneration (carneous degeneration) occurs specifically during pregnancy. It presents with acute localized pain + fever + tenderness over the fibroid. Managed conservatively with analgesics.
7. Clinical Features
Symptoms (remember: ~50% are asymptomatic)
1. Abnormal Uterine Bleeding (most common)
- Heavy/prolonged menstrual bleeding (menorrhagia)
- Submucosal fibroids are the most likely culprit
- The number and size of fibroids do NOT predict bleeding severity - location matters most
- Mechanism: distorted endometrium, impaired contractility, vascular changes
2. Pelvic Pain/Pressure
- Dull, dragging lower abdominal pain
- Dysmenorrhea
- Degeneration causes acute pain
- Torsion of pedunculated subserosal fibroid → acute abdomen requiring surgery
3. Pressure Symptoms
- Urinary frequency/urgency (anterior fibroid compressing bladder - most common)
- Hydronephrosis (lateral fibroid compressing ureter)
- Constipation, tenesmus (posterior fibroid)
4. Infertility / Reproductive Effects (less common)
- Submucous fibroids are most likely to impair fertility
- Other types rarely cause infertility alone
8. Effects in Pregnancy
Fibroids are found in ~2-4% of pregnancies. Complications include:
- Fibroid degeneration (red degeneration) - in ~5-9%, causes severe pain
- Increased cesarean section rate (49% vs 21% without fibroids)
- Increased preterm delivery risk (19.2% vs 12.7%)
- Placenta previa (3.5% vs 1.8%)
- Postpartum hemorrhage (8.3% vs 2.9%)
- Rarely: placental abruption (especially retroplacental fibroids)
- Fetal injury from mechanical compression is uncommon
9. Diagnosis
Clinical Examination
- Bimanual pelvic examination: enlarged, irregularly shaped, firm, nontender uterus
- Correlates well with uterine size at pathology even in obese women
Investigations (in order of preference)
| Investigation | Findings / Notes |
|---|---|
| Transvaginal Ultrasound (TVS) | First line; shows hypoechoic, discrete lesions with shadowing |
| Saline Infusion Sonography (SIS) | Best for submucosal fibroids; outlines intracavitary extent |
| MRI | Gold standard for mapping; best before myomectomy |
| Hysteroscopy | Diagnostic + therapeutic for submucosal fibroids |
| X-ray | Calcified fibroids ("womb stones") - incidental finding |
Routine sonographic examination is not necessary when clinical diagnosis is almost certain on bimanual examination.
10. Natural History
- Most fibroids grow slowly - median growth rate ~9% over 12 months
- Multiple fibroids in the same woman can have highly variable growth rates
- Growth rates decline with age in white women but not African American women
- 7% of fibroids regress spontaneously
- All fibroids shrink after menopause
Rapid Growth
- "Rapid uterine growth" in premenopausal women RARELY = sarcoma
- Only 1 sarcoma found among 371 women operated on for rapid growth (0.26%)
- Uterine sarcoma is a concern mainly in postmenopausal women with pain and bleeding
11. Management
A. Conservative (Observation)
- Asymptomatic women: regular follow-up
- No routine serial ultrasound needed for stable, asymptomatic fibroids
B. Medical Treatment
| Drug | Mechanism | Notes |
|---|---|---|
| GnRH Agonists (leuprolide, goserelin) | Suppress estrogen → shrink fibroids | Reduces volume 30-35%; used preoperatively; max 6 months (bone loss). Regrow after stopping |
| GnRH Antagonists (ganirelix) | Immediate GnRH suppression | 29% volume reduction in 3 weeks |
| Tranexamic acid | Antifibrinolytic | 1.3g TDS x 3-5 days during menses; reduces blood loss |
| NSAIDs | Reduce prostaglandins | Reduce bleeding and dysmenorrhea |
| Progestins / Levonorgestrel IUD (Mirena) | Progestin-mediated | Reduce bleeding; may not shrink fibroid |
| Mifepristone (RU-486) | Antiprogestin | Reduces size; not widely used in clinical practice |
| Ulipristal acetate | Selective progesterone receptor modulator (SPRM) | Used in Europe; shrinks fibroids; liver toxicity concern |
GnRH agonist preoperatively: Shrinks fibroid, corrects anemia, reduces intraoperative blood loss before myomectomy/hysterectomy
C. Surgical Treatment
Indications for Surgery:
- Heavy bleeding causing anemia not responding to medical treatment
- Significant pressure symptoms compromising quality of life
- Infertility with submucosal fibroid
- Acute pain (degeneration, torsion)
- Ureteral obstruction
- Desire for definitive treatment
Options:
| Procedure | Indication / Notes |
|---|---|
| Hysteroscopic myomectomy | Submucosal fibroids (Types 0-2); diagnostic + therapeutic |
| Abdominal myomectomy | Multiple or large fibroids; fertility-preserving |
| Laparoscopic myomectomy | Subserosal/intramural; less blood loss, faster recovery |
| Laparoscopic radiofrequency ablation | Newer technique |
| Hysterectomy | Definitive; no desire for future pregnancy; multiple failed treatments |
| Endometrial ablation | Reduces bleeding; not for submucosal type 0-1 or fertility-seeking |
Myomectomy vs Hysterectomy:
- Myomectomy is a safe alternative to hysterectomy, even for large fibroids
- 80% symptom relief reported after myomectomy
- Risk of uterine rupture in subsequent pregnancy: 0.47% (similar to VBAC)
- Fibroids can recur after myomectomy
D. Interventional Radiology
Uterine Artery Embolization (UAE):
- Embolizes uterine arteries → infarction of fibroids
- Reduces mean uterine volume by 35%
- Urinary frequency and urgency: greatly/moderately improved in 68%
- Effects on ovarian reserve, fertility, and future pregnancy are unclear - counsel patients appropriately
12. Preoperative Anemia Management
Before surgery in women with significant anemia (Hb < 9 g/dL):
- IV iron is superior to oral iron (Hb increase 3.0 vs 0.8 g/dL)
- Epoetin 250 IU/kg/week x 3 weeks reduces transfusion rates
- GnRH agonist + oral iron for 12 weeks: 74% achieve Hb >12g (vs 46% with iron alone)
13. PALM-COEIN Classification (AUB)
In the context of Abnormal Uterine Bleeding (AUB), leiomyoma is coded as AUB-L. It falls under the PALM (structural) category:
Polyp | Adenomyosis | Leiomyoma | Malignancy/Hyperplasia | Coagulopathy | Ovulatory dysfunction | Endometrial | Iatrogenic | Not classified
14. Key Exam Points to Remember
- Most common benign tumor of the female genital tract
- Monoclonal origin from a single smooth muscle cell
- Most common symptom = menorrhagia (especially submucosal)
- Pressure symptoms: urinary frequency is most common (anterior fibroid)
- Submucosal fibroid = most likely to cause bleeding and infertility
- Red degeneration = occurs in pregnancy; managed conservatively
- Rapid growth in premenopausal women is NOT a sign of malignancy
- GnRH agonists: shrink fibroids by 30-35% but only temporarily
- UAE is effective but avoid in women wanting future pregnancy
- Fibroid in PALM-COEIN = AUB-L
- Never seen before puberty; regress after menopause (estrogen/progesterone dependent)
- Malignant transformation is very rare (<1 in 1,000)
Source: Berek & Novak's Gynecology (Berek & Novak's Gynecology, Chapter 11)
This is a shared conversation. Sign in to Orris to start your own chat.