Can you explain the neurotransmitter fully with detailed molecular structure and receptors agonist antagonist everything with detailed manner with mechanism it involved with many reference you take but you also.considered seigel and kandel
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Here is the comprehensive, detailed reference on all major neurotransmitters, drawing from Eric Kandel's Principles of Neural Science (6th ed.), Kaplan & Sadock's Comprehensive Textbook of Psychiatry, Goodman & Gilman's Pharmacological Basis of Therapeutics, Katzung's Basic & Clinical Pharmacology (16th ed.), Ganong's Review of Medical Physiology, and Harper's Illustrated Biochemistry.
Neurotransmitters: A Comprehensive Reference
Overview: What Is a Neurotransmitter?
A neurotransmitter is a chemical messenger released from a presynaptic nerve terminal in response to an action potential. To qualify as a neurotransmitter, a substance must be:
- Synthesized in the neuron
- Stored in presynaptic vesicles
- Released in a Ca²⁺-dependent manner upon stimulation
- Act on specific postsynaptic receptors
- Have a defined mechanism of inactivation (reuptake, enzymatic degradation, or diffusion)
Neurotransmitters are classified as: small-molecule transmitters (amino acids, monoamines, acetylcholine) and neuropeptides (>100 identified in the brain).
PART I: CATECHOLAMINES
Catecholamine Biosynthesis - Shared Pathway
All three catecholamine neurotransmitters (dopamine, norepinephrine, epinephrine) share a common synthetic pathway starting from the dietary amino acid tyrosine.
Step-by-step synthesis (Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 419-421; Ganong's Review of Medical Physiology, p. 157):
Phenylalanine → Tyrosine (liver, phenylalanine hydroxylase)
↓ Tyrosine hydroxylase (TH) [RATE-LIMITING STEP]
+ tetrahydrobiopterin (BH4) cofactor
L-DOPA
↓ Aromatic amino acid decarboxylase (AADC)
Dopamine
↓ Dopamine-β-hydroxylase (DBH) [inside vesicles]
Norepinephrine
↓ Phenylethanolamine-N-methyltransferase (PNMT) [cytoplasmic]
Epinephrine
- Tyrosine hydroxylase requires tetrahydrobiopterin (BH4) as cofactor. Its synthesis depends on GTP-cyclohydrolase-1.
- Key regulation: TH is subject to feedback inhibition by dopamine and norepinephrine (end-product inhibition).
- DBH is unique - it is the only step that occurs inside synaptic vesicles rather than in the cytoplasm.
- PNMT is cytoplasmic; only neurons in the C1, C2, C3 regions of the medulla and the adrenal medulla express it.
- PKU (phenylketonuria): mutation in phenylalanine hydroxylase gene - phenylalanine accumulates, causing severe mental retardation.
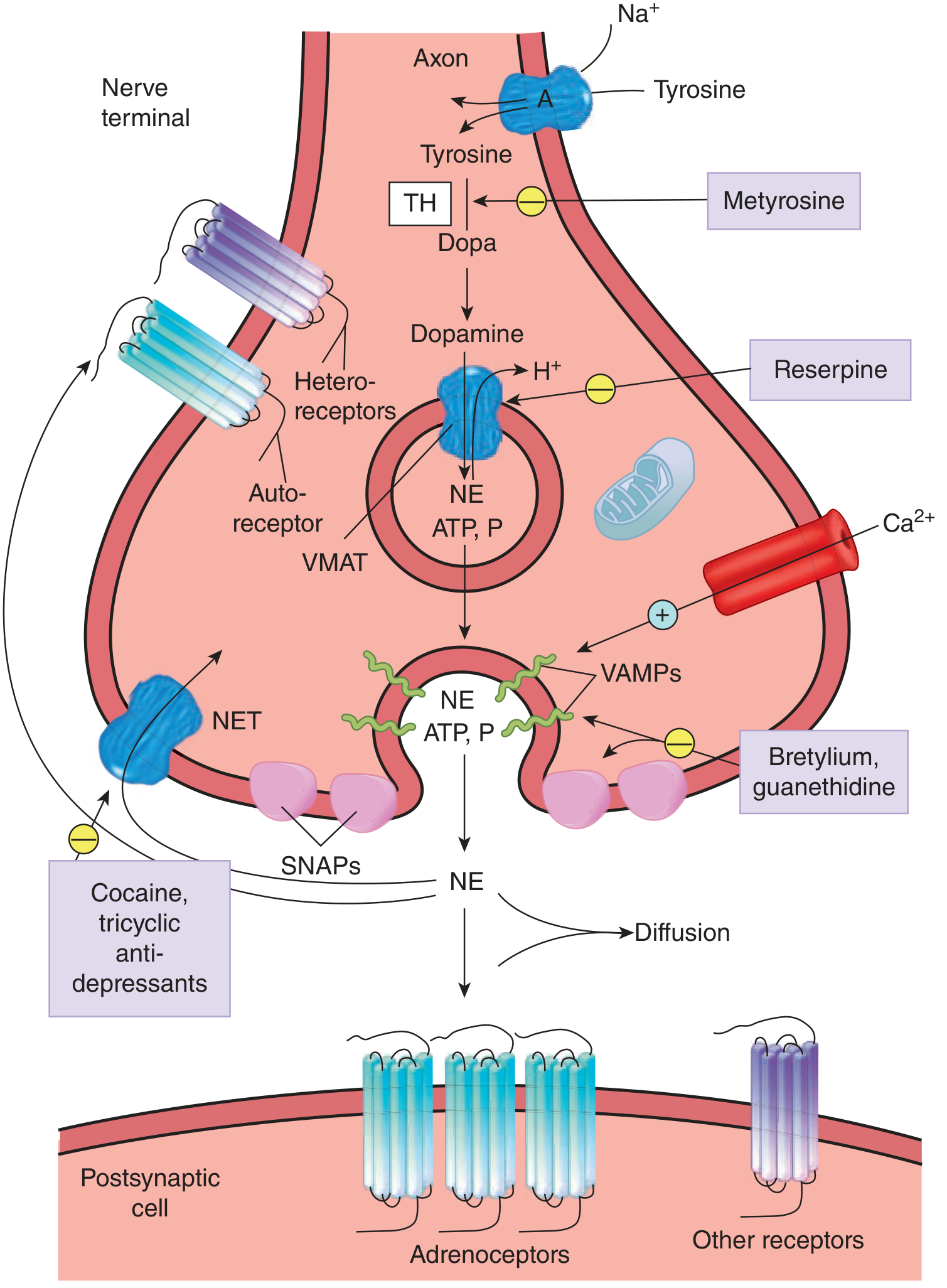
Noradrenergic synapse diagram (Ganong's):
1. DOPAMINE (DA)
Molecular Structure
- Chemical name: 3,4-dihydroxyphenethylamine
- Formula: C₈H₁₁NO₂; MW = 153.18 g/mol
- Structure: A catecholamine with a catechol ring (benzene ring with two adjacent hydroxyl groups at positions 3 and 4) and an ethylamine side chain (-CH₂-CH₂-NH₂)
- Key structural features: The catechol moiety is essential for receptor binding; the amine group can be protonated at physiological pH (pKa ~8.9), making it largely cationic
HO CH₂—CH₂—NH₂
|
HO [benzene ring]
Dopaminergic Pathways (Kaplan & Sadock, p. 418-420)
| Pathway | Origin | Termination | Function |
|---|---|---|---|
| Nigrostriatal | Substantia nigra (A9) | Striatum (caudate-putamen) | Motor control; lost in Parkinson's |
| Mesolimbic | VTA (A10) | Nucleus accumbens, amygdala, hippocampus | Reward, motivation, addiction |
| Mesocortical | VTA | Prefrontal cortex | Cognition, working memory, emotion |
| Tuberoinfundibular | Arcuate nucleus | Median eminence/pituitary | Inhibits prolactin secretion |
Vesicular Storage and Release
- Dopamine is packaged into vesicles by VMAT-2 (vesicular monoamine transporter 2) in the CNS.
- Reserpine blocks VMAT, depleting dopamine stores.
- Amphetamines reverse VMAT action, mobilizing dopamine from vesicles into the cytoplasm and then the synapse.
- Release is triggered by action potential → Ca²⁺ influx → SNARE complex-mediated exocytosis (using synaptobrevin/VAMP and SNAP-25).
Metabolism/Inactivation
- Reuptake via the dopamine transporter (DAT) - the primary termination mechanism
- MAO (monoamine oxidase) - mitochondrial; converts DA to DOPAC (3,4-dihydroxyphenylacetic acid) via oxidative deamination
- COMT (catechol-O-methyltransferase) - methylates to 3-methoxytyramine (3-MT); acts mainly extracellularly
- Final product: Homovanillic acid (HVA) = DOPAC + COMT action; measured in CSF and urine as DA metabolite marker
Dopamine Receptors
All five dopamine receptors are G-protein-coupled receptors (GPCRs) with 7 transmembrane (7-TM) domains. They are divided into two families (Kaplan & Sadock, p. 428-429):
| Receptor | Family | G-protein | Second Messenger | Main Location | Key Notes |
|---|---|---|---|---|---|
| D1 | D1-like | Gs | ↑ cAMP (adenylate cyclase ↑) | Striatum, nucleus accumbens, frontal cortex | Postsynaptic only |
| D5 | D1-like | Gs | ↑ cAMP | Frontal cortex, hypothalamus, hippocampus | Low expression; higher DA affinity than D1 |
| D2 | D2-like | Gi | ↓ cAMP (adenylate cyclase ↓) | Striatum, nucleus accumbens, pituitary | Both pre- and postsynaptic; two splice variants: D2S (presynaptic autoreceptor), D2L (postsynaptic) |
| D3 | D2-like | Gi | ↓ cAMP | Limbic areas (nucleus accumbens shell) | Can function as autoreceptor; target for addiction pharmacology |
| D4 | D2-like | Gi | ↓ cAMP | Frontal cortex, amygdala, hippocampus | Lowest expression; clozapine has high D4 affinity |
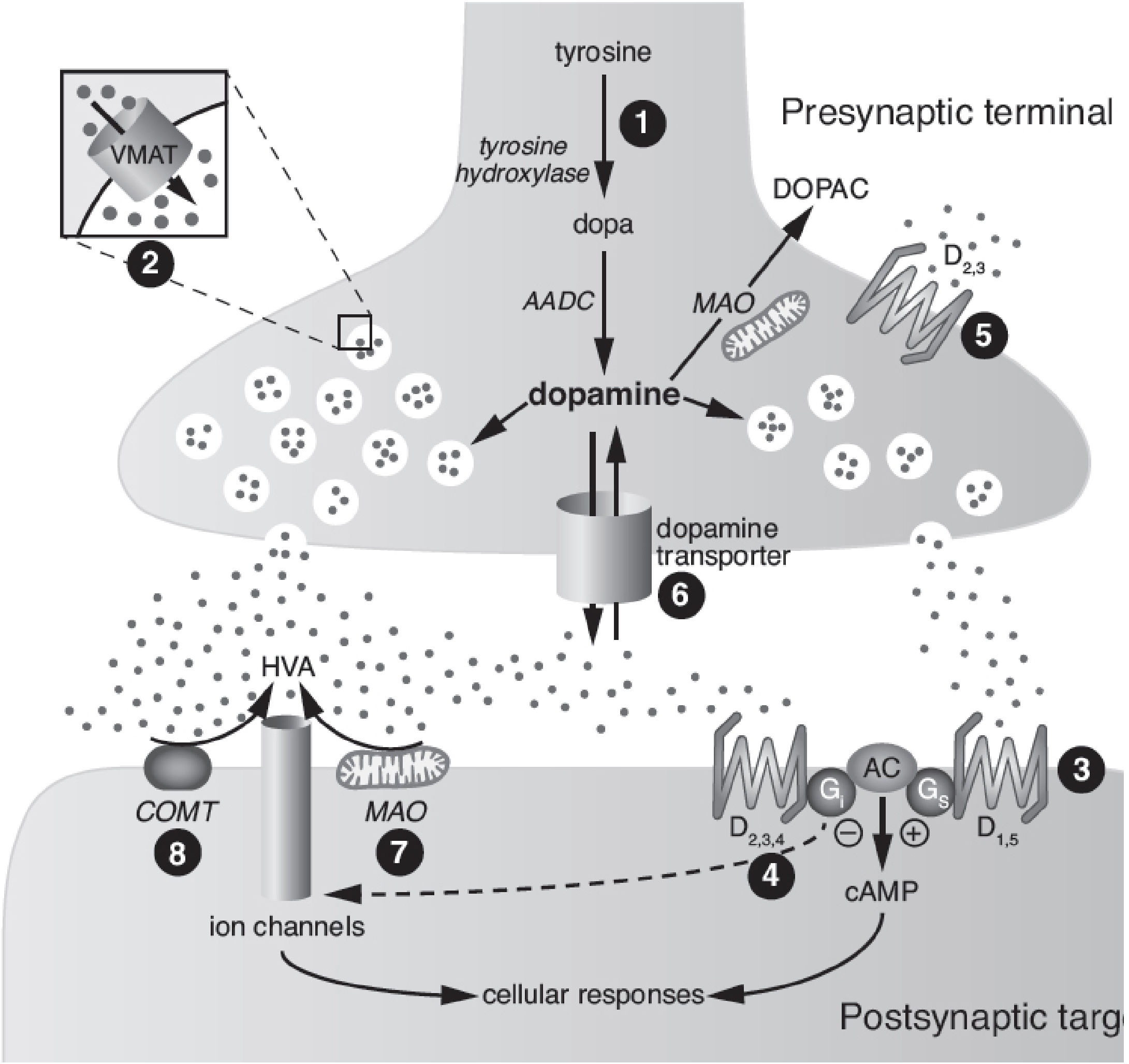
Dopaminergic synapse diagram (Kaplan & Sadock, p. 422):
Signal Transduction Mechanisms
- D1/D5 (Gs pathway): Gs → adenylate cyclase → ↑cAMP → PKA activation → phosphorylation of DARPP-32 (dopamine- and cAMP-regulated phosphoprotein) → modulation of ion channels, gene expression via CREB
- D2/D3/D4 (Gi pathway): Gi → ↓adenylate cyclase → ↓cAMP; also activates K⁺ channels (hyperpolarization) and inhibits voltage-gated Ca²⁺ channels
Dopamine Receptor Agonists
| Drug | Receptor Selectivity | Clinical Use |
|---|---|---|
| Levodopa (L-DOPA) | Non-selective (prodrug; converted to DA) | Parkinson's disease (first-line) |
| Carbidopa/benserazide | AADC inhibitor (peripheral, does not cross BBB) | Combined with L-DOPA to reduce peripheral side effects |
| Pramipexole | D2/D3 preferring | Parkinson's disease, restless legs syndrome |
| Ropinirole | D2/D3 preferring | Parkinson's disease, restless legs syndrome |
| Bromocriptine | D2 agonist (ergot derivative) | Parkinsonism, hyperprolactinemia, acromegaly (rarely used for PD now) |
| Apomorphine | Potent D1 and D2 agonist | PD rescue therapy for severe off periods |
| Cabergoline | D2 preferring (ergot) | Hyperprolactinemia |
| Rotigotine | D1/D2/D3 | Parkinson's (transdermal patch) |
(Katzung, p. 780-781; Goodman & Gilman)
Dopamine Receptor Antagonists
| Drug | Type | Receptor Profile | Clinical Use | Key Side Effects |
|---|---|---|---|---|
| Haloperidol | Typical antipsychotic | D2 selective | Schizophrenia, acute agitation | High EPS risk, tardive dyskinesia |
| Chlorpromazine | Typical antipsychotic | D1 + D2 block | Schizophrenia | Sedation, EPS, anticholinergic |
| Clozapine | Atypical antipsychotic | D4 > D2, 5HT2A, H1, M1 | Treatment-resistant schizophrenia | Agranulocytosis (weekly CBC), weight gain |
| Risperidone | Atypical antipsychotic | D2 + 5HT2A | Schizophrenia, bipolar | Hyperprolactinemia, mild EPS |
| Olanzapine | Atypical antipsychotic | D2 + 5HT2A + H1 + M1 | Schizophrenia, bipolar | Weight gain, metabolic syndrome |
| Aripiprazole | Atypical (partial agonist) | D2 partial agonist, 5HT2A antagonist, 5HT1A partial agonist | Schizophrenia, MDD augmentation | Akathisia, minimal metabolic effects |
| Metoclopramide | Prokinetic/antiemetic | D2 block | GERD, nausea, gastroparesis | Tardive dyskinesia with chronic use |
| Domperidone | Antiemetic | D2 block (peripheral) | Nausea, prolactin deficiency | Does not cross BBB; QT prolongation |
(Kaplan & Sadock, p. 429; Goodman & Gilman)
Dopaminergic Pathology:
- Schizophrenia: Hyperdopaminergic activity in mesolimbic (positive symptoms); hypodopaminergic in mesocortical (negative/cognitive symptoms)
- Parkinson's disease: Loss of nigrostriatal dopamine neurons (>70% lost before symptoms appear)
- Reward/addiction: Mesolimbic pathway; drugs of abuse all increase nucleus accumbens DA
- ADHD: Dysregulation in mesocortical DA (methylphenidate, amphetamines increase DAT-mediated reuptake blockade or DA release)
2. NOREPINEPHRINE (NE) / NORADRENALINE
Molecular Structure
- Chemical name: (R)-(-)-4-(2-amino-1-hydroxyethyl)benzene-1,2-diol
- Formula: C₈H₁₁NO₃; MW = 169.18 g/mol
- Structure: Identical to dopamine but with a hydroxyl group at the β-carbon of the ethylamine side chain (added by DBH inside vesicles)
- Stereochemistry: The naturally active form is the L-(−)-isomer (levorotatory)
Noradrenergic Pathways
- Locus coeruleus (LC) in the pons: the primary noradrenergic nucleus; sends projections to virtually the entire CNS (cortex, hippocampus, cerebellum, spinal cord). Involved in arousal, attention, stress responses
- Lateral tegmentum: Projects to limbic areas; involved in emotion and autonomic regulation
- Peripheral: Postganglionic sympathetic neurons release NE at all organs except sweat glands (which use ACh)
Synthesis, Storage, Release (Ganong's, p. 157)
- NE synthesis follows the catecholamine pathway through dopamine
- DBH converts dopamine → NE inside synaptic vesicles (unique among NT synthesis steps)
- After release, NE is terminated primarily by reuptake via NET (norepinephrine transporter) - the most important mechanism
- Tricyclic antidepressants (TCAs) and SNRIs block NET → ↑synaptic NE
- Cocaine also blocks NET (explains cardiovascular toxicity)
Adrenergic Receptors
All adrenergic receptors are 7-TM GPCRs:
| Receptor | G-protein | Mechanism | Distribution | Agonist Effect |
|---|---|---|---|---|
| α1 | Gq | PLC → IP3/DAG → ↑Ca²⁺, PKC | Blood vessels (vasoconstriction), bladder, prostate, iris (mydriasis) | Vasoconstriction, ↑peripheral resistance |
| α2 | Gi | ↓cAMP | Presynaptic (autoreceptor, inhibits NE release), platelets, fat cells, CNS | Inhibits NE release (feedback); sedation when central |
| β1 | Gs | ↑cAMP → PKA | Heart (SA node, AV node, myocardium) | ↑HR, ↑contractility, ↑conduction |
| β2 | Gs | ↑cAMP → PKA | Bronchi, blood vessels (vasodilation), uterus, liver | Bronchodilation, vasodilation, glycogenolysis |
| β3 | Gs | ↑cAMP | Adipose tissue, bladder | Lipolysis, bladder relaxation |
NE/Adrenergic Agonists
| Drug | Receptor | Clinical Use |
|---|---|---|
| Epinephrine (Adrenaline) | α1, α2, β1, β2 (non-selective) | Anaphylaxis (first-line), cardiac arrest, local anesthesia (vasoconstriction) |
| Norepinephrine | α1 >> β1 (minimal β2) | Septic shock (vasopressor) |
| Dopamine (low dose) | DA receptors | Renal/splanchnic vasodilation |
| Clonidine | α2 agonist (central) | Hypertension, ADHD, opioid withdrawal, pain |
| Dexmedetomidine | α2 agonist | ICU sedation, analgesia |
| Phenylephrine | α1 selective | Nasal decongestant, hypotension during spinal anesthesia |
| Salbutamol/Albuterol | β2 selective | Asthma, COPD (bronchodilation), preterm labor |
| Salmeterol/Formoterol | β2 selective (LABA) | Asthma, COPD (long-acting) |
| Dobutamine | β1 selective | Cardiogenic shock, heart failure (inotropic support) |
| Isoproterenol | β1 + β2 | Bradycardia, AV block (rarely used now) |
NE/Adrenergic Antagonists
| Drug | Receptor | Clinical Use |
|---|---|---|
| Prazosin/Terazosin/Tamsulosin | α1 selective | Hypertension, BPH |
| Phentolamine | α1 + α2 (non-selective) | Pheochromocytoma crisis, extravasation of vasopressors |
| Propranolol | β1 + β2 (non-selective) | Hypertension, angina, arrhythmia, tremor, thyroid storm |
| Metoprolol/Atenolol | β1 selective (cardioselective) | Hypertension, post-MI, heart failure, rate control |
| Carvedilol | α1 + β1 + β2 | Heart failure (mortality benefit) |
| Labetalol | α1 + β (non-selective) | Hypertensive emergency in pregnancy |
Metabolism of Catecholamines
- MAO (MAO-A and MAO-B): Intraneuronal; catalyzes oxidative deamination
- COMT: Extraneuronal; catalyzes O-methylation
- NE → via MAO → DHPG (3,4-dihydroxyphenylglycol), via COMT → normetanephrine; final product = VMA (vanillylmandelic acid)
- MAO inhibitors (MAOIs): phenelzine, tranylcypromine, selegiline (MAO-B selective) - used in depression, Parkinson's
3. EPINEPHRINE (Adrenaline)
Molecular Structure
- Chemical name: (R)-4-[1-hydroxy-2-(methylamino)ethyl]-1,2-benzenediol
- Formula: C₉H₁₃NO₃; MW = 183.20 g/mol
- Structure: NE with an additional N-methyl group on the amine (added by PNMT)
- The N-methyl group increases β-receptor affinity
CNS and Peripheral Roles
- Brain epinephrine neurons are concentrated in medullary C1, C2, C3 cell groups; project to LC, dorsal raphe, hypothalamus, nucleus accumbens.
- Primarily a hormone from the adrenal medulla (80% of adrenal output), but also functions as a CNS neurotransmitter.
- Broader receptor action than NE: acts on α1, α2, β1, β2, β3 receptors.
PART II: SEROTONIN (5-Hydroxytryptamine, 5-HT)
Molecular Structure
- Chemical name: 5-hydroxytryptamine
- Formula: C₁₀H₁₂N₂O; MW = 176.21 g/mol
- Structure: An indolethylamine - an indole ring (bicyclic: benzene fused with pyrrole) with a hydroxyl group at position 5 and an ethylamine (-CH₂-CH₂-NH₂) side chain
- Precursor: L-tryptophan (essential amino acid, dietary)
Synthesis Pathway
L-Tryptophan
↓ Tryptophan hydroxylase (TPH) [RATE-LIMITING STEP; requires BH4]
TPH1 (peripheral/enterochromaffin cells)
TPH2 (brain/neurons)
5-Hydroxytryptophan (5-HTP)
↓ Aromatic amino acid decarboxylase (AADC)
5-Hydroxytryptamine (Serotonin)
↓ MAO-A (mainly) + aldehyde dehydrogenase
5-Hydroxyindoleacetic acid (5-HIAA) [urinary metabolite - measured in carcinoid syndrome]
Serotonergic Pathways
- Raphe nuclei (dorsal raphe = B7, median raphe = B8) in the brainstem are the primary serotonergic cell bodies
- Project to cortex, limbic system, hippocampus, striatum, cerebellum, spinal cord
- 90%+ of body's serotonin is in enterochromaffin cells of the GI tract; 8% in platelets
- Melatonin synthesis: serotonin → (N-acetyltransferase) → N-acetylserotonin → (HIOMT) → melatonin (in pineal gland)
Vesicular Storage and Termination
- Stored in vesicles via VMAT-2 (same as catecholamines)
- Terminated primarily by SERT (serotonin transporter) reuptake
- SSRIs block SERT → ↑synaptic 5-HT → antidepressant effect
- Degraded by MAO-A → 5-HIAA
Serotonin Receptors (Kaplan & Sadock, p. 441 onwards)
There are 7 receptor families (5-HT1 through 5-HT7), comprising 14+ subtypes. All are GPCRs except 5-HT3, which is a ligand-gated ion channel.
| Receptor | Type | G-protein/Mechanism | Location | Function |
|---|---|---|---|---|
| 5-HT1A | GPCR | Gi → ↓cAMP, ↑K⁺ conductance | Raphe nuclei (autoreceptor), hippocampus, cortex | Anxiolysis, antidepressant; inhibits neuronal firing |
| 5-HT1B | GPCR | Gi → ↓cAMP | Terminal autoreceptor, striatum, cerebellum | Inhibits 5-HT release; migraine target |
| 5-HT1D | GPCR | Gi → ↓cAMP | Trigeminal nerve terminals, basal ganglia | Migraine; triptans are 5-HT1B/1D agonists |
| 5-HT2A | GPCR | Gq → PLC → IP3/DAG → ↑Ca²⁺ | Cortex (pyramidal + interneurons), platelets | Hallucinogens act here (LSD, psilocybin); atypicals block 5HT2A |
| 5-HT2B | GPCR | Gq → PLC | Periphery (cardiovascular); limited CNS | Cardiotoxicity (valvulopathy with 5-HT2B agonists) |
| 5-HT2C | GPCR | Gq → PLC | Choroid plexus, limbic, VTA, nucleus accumbens | Weight regulation; regulates mesolimbic DA; X-linked gene |
| 5-HT3 | Ligand-gated ion channel | Na⁺/K⁺ (depolarizing) | Peripheral sensory/autonomic neurons, area postrema, GI tract | Nausea and vomiting (area postrema); pain |
| 5-HT4 | GPCR | Gs → ↑cAMP | GI tract, brain | Prokinetic (GI motility) |
| 5-HT6 | GPCR | Gs → ↑cAMP | Striatum, limbic | Cognition; target for novel antidepressants/antipsychotics |
| 5-HT7 | GPCR | Gs → ↑cAMP | Hypothalamus, thalamus | Circadian rhythm, sleep; antipsychotic affinity |
Key Signal Transduction
- 5-HT2 family → Gq → PLC → IP3 (releases Ca²⁺ from ER) + DAG (activates PKC) → phosphorylation cascades
- 5-HT1 family → Gi → ↓cAMP; opens inward rectifier K⁺ channels (GIRK channels) → hyperpolarization
- 5-HT3 → rapid depolarization via cation influx (Na⁺/K⁺)
Serotonin Agonists
| Drug | Target | Use |
|---|---|---|
| Sumatriptan/triptans | 5-HT1B/1D agonists | Acute migraine (vasoconstriction of meningeal vessels, inhibit CGRP release) |
| Buspirone | 5-HT1A partial agonist | Generalized anxiety disorder (no dependence, slow onset) |
| LSD, Psilocybin, Mescaline | 5-HT2A full/partial agonists | Hallucinogens (research use for depression/PTSD) |
| Cisapride, Metoclopramide | 5-HT4 agonists | Prokinetics (GI motility) |
| Lorcaserin | 5-HT2C agonist | Antiobesity (withdrawn 2020 due to cancer risk) |
| Psilocybin | 5-HT2A/2C agonist | Depression, PTSD (breakthrough therapy trials) |
Serotonin Antagonists
| Drug | Target | Use |
|---|---|---|
| Ondansetron/Granisetron | 5-HT3 antagonists | Chemotherapy-induced nausea and vomiting (CINV), post-op nausea |
| Clozapine, Olanzapine, Risperidone | 5-HT2A antagonists (+ D2) | Atypical antipsychotics |
| Pimavanserin | 5-HT2A inverse agonist/antagonist | Parkinson's disease psychosis |
| Cyproheptadine | 5-HT2 + H1 antagonist | Serotonin syndrome, appetite stimulant, migraine prophylaxis |
| Ketanserin | 5-HT2A antagonist | Hypertension, antithrombotic (experimental) |
| Methysergide | 5-HT2A/2C antagonist | Migraine prophylaxis (now rarely used due to retroperitoneal fibrosis) |
SSRIs/SNRIs (Reuptake Inhibitors - Indirect Serotonergic Agents)
| Drug | Mechanism | Use |
|---|---|---|
| Fluoxetine, Sertraline, Escitalopram | SERT blockade | MDD, anxiety disorders, OCD |
| Venlafaxine, Duloxetine | SERT + NET blockade | MDD, GAD, pain |
5-HT2A and Hallucination Mechanism (Kandel's Principles of Neural Science)
Hallucinogenic drugs (LSD, psilocybin, mescaline) act as full or partial agonists at the 5HT2A receptor in cortical pyramidal neurons and interneurons. This disrupts the normal filtering of sensory input by the prefrontal cortex, producing sensory distortions and altered perception. Second-generation antipsychotics are characterized by their higher potency as 5HT2A antagonists vs. D2 blockers.
PART III: ACETYLCHOLINE (ACh)
Molecular Structure
- Chemical name: 2-(acetyloxy)-N,N,N-trimethylethan-1-aminium
- Formula: C₇H₁₆NO₂⁺; MW = 146.21 g/mol (as the cation)
- Structure: An ester of choline and acetic acid
- Choline: HO-CH₂-CH₂-N⁺(CH₃)₃
- Acetyl group: CH₃-CO-O- esterified to the hydroxyl of choline
- Key structural feature: The quaternary ammonium group (N⁺(CH₃)₃) carries a permanent positive charge, making ACh unable to cross lipid membranes (cannot enter the CNS when given peripherally)
O
‖
CH₃-C-O-CH₂-CH₂-N⁺(CH₃)₃
Synthesis and Metabolism
- Synthesis: Choline + Acetyl-CoA → ACh
- Enzyme: Choline acetyltransferase (ChAT) - the marker enzyme for cholinergic neurons
- Choline is derived from diet and recycled from ACh hydrolysis (high-affinity choline transporter)
- Rate-limiting: availability of choline and acetyl-CoA
- Vesicular storage: ACh packaged by VAChT (vesicular ACh transporter)
- Vesamicol blocks VAChT
- Termination: Unlike all other NTs, ACh is NOT terminated by reuptake. Instead:
- Acetylcholinesterase (AChE) - at the synapse and on RBCs; hydrolyzes ACh to choline + acetate in <1 ms
- Butyrylcholinesterase (BuChE, pseudocholinesterase) - in plasma and liver; broader substrate specificity
- Choline is recaptured by the high-affinity choline transporter (hemicholinium-3 blocks this)
Cholinergic Pathways
| Pathway | Location | Projection | Function |
|---|---|---|---|
| Basal forebrain nuclei (Nucleus basalis of Meynert, medial septum) | Forebrain | Cortex, hippocampus | Memory, attention, cognition; lost in Alzheimer's |
| Brainstem (Pedunculopontine, laterodorsal tegmental nuclei) | Pons/midbrain | Thalamus, basal ganglia | REM sleep, arousal |
| Neuromuscular junction | Motor neurons | Skeletal muscle | Voluntary movement |
| Autonomic ganglia | Preganglionic (sympathetic + parasympathetic) | Postganglionic neurons | Ganglionic transmission (nicotinic) |
| Parasympathetic postganglionic | Ganglia | Effector organs | Bradycardia, salivation, GI motility, miosis (muscarinic) |
Acetylcholine Receptors
There are two main classes - Nicotinic (nAChR) and Muscarinic (mAChR) - with fundamentally different structures and mechanisms.
Nicotinic Acetylcholine Receptors (nAChR) - Kandel's Principles of Neural Science, p. 302-303
The nicotinic receptor is the archetypal ligand-gated ion channel and one of the most studied proteins in neuroscience (Kandel's landmark contribution):
- Structure: Pentameric ion channel; each subunit has 4 transmembrane (TM) helices (M1-M4), with M2 forming the pore lining
- Muscle type (NMJ): Composed of α₁₂β₁γδ (fetal) or α₁₂β₁εδ (adult) subunits
- Neuronal type: α (α2-α10) and β (β2-β4) subunits in various combinations; e.g., α4β2 is the predominant brain subtype; α7 (homomeric) in cortex and hippocampus
- Ion permeability: Na⁺ and K⁺ (at NMJ); α7 also highly permeable to Ca²⁺
- Mechanism (Kandel's): Two ACh molecules must bind (one per α subunit) → conformational change → channel opening → net inward current (depolarization) → end-plate potential (EPP) → action potential
Nicotinic agonists:
- Nicotine (partial agonist at most subtypes; full agonist at some)
- Succinylcholine (depolarizing NMJ blocker - acts as agonist, causes persistent depolarization → phase I block)
- Varenicline (partial agonist at α4β2 - smoking cessation)
Nicotinic antagonists:
- NMJ blockers (non-depolarizing): Tubocurarine, vecuronium, rocuronium, atracurium - competitively block postsynaptic nAChR at NMJ → muscle relaxation (reversed by neostigmine/sugammadex)
- Ganglionic blockers: Hexamethonium, trimethaphan - block ganglionic nAChR (historical antihypertensives)
- α-Bungarotoxin: Snake toxin; irreversibly blocks muscle-type nAChR (critical research tool - Kandel's lab used it to identify and isolate the nAChR)
- Mecamylamine: CNS-penetrant ganglionic blocker; research use
Muscarinic Acetylcholine Receptors (mAChR)
Five subtypes (M1-M5), all GPCRs with 7-TM topology:
| Receptor | G-protein | Mechanism | Location | Effect |
|---|---|---|---|---|
| M1 | Gq | ↑IP3/DAG → ↑Ca²⁺ | Cortex, hippocampus, gastric parietal cells, autonomic ganglia | Cognition, memory; ↑gastric acid (parietal cells) |
| M2 | Gi | ↓cAMP, ↑IKACh (GIRK channels) | Heart (SA node, AV node), presynaptic autoreceptors | ↓HR, ↓conduction; presynaptic inhibition of ACh release |
| M3 | Gq | ↑IP3/DAG → ↑Ca²⁺ | Smooth muscle (bronchi, gut, bladder), glands, blood vessel endothelium | Bronchoconstriction, GI motility, bladder contraction, salivation; vasodilation via NO release |
| M4 | Gi | ↓cAMP | Striatum, basal ganglia | Modulates DA release; movement control |
| M5 | Gq | ↑IP3/DAG | Dopamine neurons (VTA, substantia nigra), brain vasculature | Modulates DA and drug reward; cerebral vasodilation |
Muscarinic agonists:
- Pilocarpine: M3 agonist; glaucoma (↑aqueous humor drainage), Sjögren's syndrome (dry mouth)
- Bethanechol: M3 selective; urinary retention, gastroparesis
- Carbachol: Non-selective; resistant to AChE; glaucoma
- Cevimeline: M3 agonist; Sjögren's syndrome
- Muscarine: Natural alkaloid (mushrooms); non-selective agonist - the "toxidrome" prototype
Muscarinic antagonists (Anticholinergics):
| Drug | Selectivity | Clinical Use |
|---|---|---|
| Atropine | Non-selective | Bradycardia, organophosphate poisoning, preoperative antisialagogue, ophthalmology (mydriasis) |
| Scopolamine | Non-selective | Motion sickness (transdermal) |
| Ipratropium/Tiotropium | M2/M3; airways | COPD, asthma bronchodilation (inhaled) |
| Oxybutynin, Tolterodine, Solifenacin | M3 selective | Overactive bladder, urge incontinence |
| Benztropine, Trihexyphenidyl | Non-selective CNS | Drug-induced parkinsonism, dystonia |
| Glycopyrrolate | Non-selective | Antisialagogue (does not cross BBB) |
| Darifenacin | M3 selective | Overactive bladder |
Anticholinesterases (Indirect Cholinergic Agonists) - prolong ACh in synapse:
| Drug | Mechanism | Duration | Use |
|---|---|---|---|
| Neostigmine | Carbamate; reversible AChE inhibitor (quaternary - peripheral) | Short | Reversal of NMJ blockade, myasthenia gravis |
| Pyridostigmine | Carbamate; reversible (quaternary - peripheral) | Intermediate | Myasthenia gravis (drug of choice) |
| Physostigmine | Carbamate; reversible (tertiary - crosses BBB) | Short | Anticholinergic toxicity/overdose reversal |
| Donepezil, Rivastigmine, Galantamine | Reversible (crosses BBB) | Long | Alzheimer's disease (symptomatic) |
| Edrophonium | Reversible (quaternary, very short) | Very short | Diagnosis of myasthenia gravis (Tensilon test) |
| Organophosphates (Sarin, VX, Malathion) | Irreversible AChE inhibition | Irreversible | Nerve agents/pesticides (SLUDGE toxidrome) |
Organophosphate toxicity (SLUDGE/DUMBELS): Salivation, Lacrimation, Urination, Diarrhea, GI cramps, Emesis + Bradycardia, miosis
- Treatment: Atropine (large doses for muscarinic effects) + pralidoxime (2-PAM; regenerates AChE before "aging")
PART IV: GABA (γ-Aminobutyric Acid)
Molecular Structure
- Chemical name: 4-aminobutanoic acid
- Formula: C₄H₉NO₂; MW = 103.12 g/mol
- Structure: A 4-carbon chain with an amino group at one end (C1-NH₂) and a carboxyl group at the other; the amino group is NOT on the α-carbon (unlike α-amino acids), hence GABA is a non-protein amino acid
- Charge at physiological pH: Zwitterionic (NH₃⁺ and COO⁻ groups)
H₂N-CH₂-CH₂-CH₂-COOH
(4-aminobutyric acid)
Synthesis and Degradation (GABA Shunt)
Glutamate → GABA
↓ Glutamate decarboxylase (GAD) [requires pyridoxal phosphate/Vitamin B6 as cofactor]
GABA
↓ GABA transaminase (GABA-T) [in mitochondria]
Succinic semialdehyde
↓ Succinic semialdehyde dehydrogenase
Succinate (enters Krebs cycle)
- GAD (glutamic acid decarboxylase) is the marker enzyme for GABAergic neurons
- Pyridoxine (B6) deficiency → ↓GAD activity → ↓GABA → seizures (especially in neonates)
- GABA-T is also inhibited by vigabatrin (irreversible; anticonvulsant) → ↑GABA accumulation
- Storage: vesicular by VGAT (vesicular GABA transporter, also transports glycine)
- Reuptake: GAT-1, GAT-2, GAT-3 transporters; tiagabine blocks GAT-1 (anticonvulsant)
GABA Receptors
GABA-A Receptor (Ionotropic - Ligand-Gated Cl⁻ Channel)
- Structure: Pentameric; assembled from subunits belonging to families α(1-6), β(1-3), γ(1-3), δ, ε, θ, π, ρ(1-3)
- The most common native receptor contains 2α + 2β + 1γ subunits
- Ion selectivity: Cl⁻ (primarily); hyperpolarizing (Cl⁻ influx) → inhibitory postsynaptic potential (IPSP)
- Exception: In early development, Cl⁻ is high intracellularly, so GABA-A is depolarizing (excitatory) in fetal/neonatal neurons
- Binding sites (multiple allosteric modulatory sites):
- GABA binding site: Between α and β subunits
- Benzodiazepine site: On γ subunit (between α and γ) - allosteric; increases frequency of Cl⁻ channel opening without activating the channel directly
- Barbiturate/anesthetic site: Within the channel pore (on β subunit TM2) - increases duration of Cl⁻ channel opening; can open channel independently at high concentrations
- Steroid (neurosteroid) site: On α and β subunits (distinct from benzodiazepine site)
- Ethanol: Acts on a hydrophobic pocket in the TM domain (mainly δ-subunit containing receptors)
- Picrotoxin/Bicuculline: Channel blockers and competitive antagonists respectively - convulsants
GABA-A modulators - Benzodiazepines:
| Drug | Notes | Use |
|---|---|---|
| Diazepam | Long-acting, active metabolites | Anxiety, seizures, alcohol withdrawal, muscle spasm |
| Lorazepam | No active metabolites; IV | Status epilepticus (first-line), premedication |
| Midazolam | Short-acting, water-soluble | Procedural sedation, ICU sedation |
| Clonazepam | Long-acting | Seizures, panic disorder, REM sleep behavior disorder |
| Alprazolam | Intermediate | Panic disorder, anxiety |
| Flumazenil | Competitive antagonist at benzodiazepine site | Reversal of benzodiazepine sedation |
Mechanism: BZDs bind between α and γ subunits → allosteric conformational change → ↑frequency of Cl⁻ channel opening (not conductance or duration) → enhanced inhibitory neurotransmission
GABA-A modulators - Barbiturates:
| Drug | Use |
|---|---|
| Phenobarbital | Epilepsy (particularly in neonates) |
| Thiopental | IV induction of anesthesia |
| Pentobarbital | Refractory status epilepticus, euthanasia |
Mechanism: Barbiturates bind within the channel → ↑duration of Cl⁻ channel opening; at high doses, open channel directly even without GABA → broader CNS depression, risk of respiratory depression (explains narrow therapeutic index vs. BZDs)
Other GABA-A modulators:
- Propofol: Acts at GABA-A (β subunit) + other sites; IV anesthetic
- Etomidate: GABA-A (β2/β3); IV induction (adrenal suppression concern)
- Neurosteroids (allopregnanolone/brexanolone): Positive allosteric modulator of GABA-A at a δ-containing extrasynaptic site; brexanolone (IV allopregnanolone) approved for postpartum depression
- Alcohol: GABA-A positive modulator; NMDA antagonist
- Z-drugs (zolpidem, zaleplon, eszopiclone): BZD receptor agonists (GABA-A at α1 subunit) - more selective for sedation/sleep
GABA-B Receptor (Metabotropic - GPCR)
- Structure: Heterodimer of GABA-B1 and GABA-B2 subunits (unique among GPCRs)
- G-protein: Gi/Go
- Mechanism: ↓cAMP; ↑K⁺ conductance (GIRK - hyperpolarization); ↓Ca²⁺ conductance (presynaptic, inhibits transmitter release)
- Location: Both presynaptic (autoreceptor, reducing GABA release; also heteroreceptor on glutamatergic terminals) and postsynaptic
GABA-B agonists:
- Baclofen: GABA-B agonist; muscle relaxant (spasticity in MS, spinal cord injury), hiccups, alcohol use disorder; intrathecal baclofen for severe spasticity
- GHB (gamma-hydroxybutyrate): GABA-B agonist + GHB receptor agonist; Xyrem for narcolepsy/cataplexy; drug of abuse
GABA-B antagonists:
- CGP36742, SGS742: Research tools; potential use in cognitive enhancement
PART V: GLUTAMATE
Molecular Structure
- Chemical name: L-Glutamic acid (2-aminopentanedioic acid)
- Formula: C₅H₉NO₄; MW = 147.13 g/mol
- Structure: An α-amino acid with two carboxyl groups (α-carboxyl at C1, γ-carboxyl at C5) and an amino group at C2
- The principal excitatory neurotransmitter of the CNS; makes up >50% of all CNS synapses
HOOC-CH(NH₂)-CH₂-CH₂-COOH
Synthesis and Termination
- Synthesized from α-ketoglutarate (Krebs cycle intermediate) via transamination or from glutamine via glutaminase (glutamine-glutamate cycle)
- Glutamine-glutamate cycle: Released glutamate is taken up by astrocytes → converted to glutamine by glutamine synthetase → released to neurons → converted back to glutamate by glutaminase
- Vesicular storage by VGluT1, VGluT2, VGluT3
- Reuptake by EAATs (Excitatory Amino Acid Transporters, 1-5): EAAT1 (GLAST) and EAAT2 (GLT-1) are astrocytic; EAAT3/4 are neuronal. Riluzole (ALS drug) enhances EAAT-mediated glutamate clearance
Glutamate Receptors
Ionotropic Glutamate Receptors
| Receptor | Subunits | Ion Permeability | Key Features |
|---|---|---|---|
| AMPA (α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid) | GluA1-4 | Na⁺, K⁺; Ca²⁺ permeability depends on GluA2 subunit (GluA2-lacking receptors are Ca²⁺ permeable) | Fast synaptic transmission; mediates most rapid EPSPs; phosphorylation of AMPA receptors critical for LTP |
| NMDA (N-methyl-D-aspartate) | GluN1, GluN2(A-D), GluN3 | Na⁺, K⁺, Ca²⁺ (highly) | Dual-gated: requires BOTH glutamate AND glycine (at GluN1 glycine/D-serine site) AND membrane depolarization (to relieve Mg²⁺ block); "coincidence detector" for LTP/LTD |
| Kainate | GluK1-5 | Na⁺, K⁺; some Ca²⁺ | Synaptic plasticity; presynaptic modulation of GABA release |
NMDA receptor - critical details (Kaplan & Sadock; Kandel's Principles):
The NMDA receptor has multiple binding/modulatory sites:
- Glutamate binding site (GluN2 subunit)
- Co-agonist/glycine/D-serine site (GluN1 subunit) - MUST be occupied for channel opening
- Mg²⁺ block (inside channel pore, at resting membrane potential) - removed by depolarization (voltage-dependent)
- PCP/ketamine/dizocilpine (MK-801) site - within open channel (open-channel blockers)
- Zinc site (inhibitory modulation; on GluN2A/B)
- Polyamine site (spermidine, spermine - positive modulation)
NMDA Mechanism - LTP (Long-Term Potentiation):
- High-frequency presynaptic stimulation → large glutamate release
- Simultaneous AMPA-mediated depolarization → removes Mg²⁺ block from NMDA receptor
- NMDA channel opens → Ca²⁺ influx → activates CaM kinase II, PKC, PKA
- CaMKII phosphorylates AMPA receptors → ↑conductance; also promotes trafficking of AMPA receptors to synapse
- CREB activation → gene expression → late-phase LTP (structural changes, new synapses)
Metabotropic Glutamate Receptors (mGluR1-8)
| Group | Subtypes | G-protein | Mechanism | Location | Function |
|---|---|---|---|---|---|
| Group I | mGluR1, mGluR5 | Gq | ↑PLC → ↑IP3/DAG → ↑Ca²⁺ | Postsynaptic | Enhance NMDA function; pain sensitization; anxiety |
| Group II | mGluR2, mGluR3 | Gi | ↓cAMP | Presynaptic autoreceptor and heteroreceptor | Inhibit glutamate release; anxiolytic targets |
| Group III | mGluR4, mGluR6, mGluR7, mGluR8 | Gi | ↓cAMP | Presynaptic | Inhibit glutamate release; mGluR6 in retina (visual processing) |
Glutamate Receptor Antagonists (NMDA)
| Drug | Mechanism | Use |
|---|---|---|
| Ketamine | NMDA open-channel blocker (+ other effects) | IV/IM anesthesia, procedural sedation; IV ketamine for treatment-resistant depression |
| Esketamine (S-ketamine, Spravato) | NMDA blocker | Treatment-resistant depression (nasal spray, FDA-approved 2019) |
| Memantine | Low-affinity, uncompetitive NMDA antagonist | Moderate-to-severe Alzheimer's disease |
| Amantadine | Weak NMDA antagonist | Parkinson's disease (also antiviral); drug-induced dyskinesias |
| Phencyclidine (PCP) | NMDA blocker (higher affinity than ketamine) | Drug of abuse; psychosis model for schizophrenia |
| Riluzole | Inhibits glutamate release + enhances reuptake | ALS (modestly prolongs survival) |
| Dextromethorphan | NMDA blocker | Cough; combined with quinidine for pseudobulbar affect |
Glutamate and Schizophrenia (NMDA hypofunction hypothesis): PCP and ketamine (NMDA antagonists) produce both positive AND negative symptoms resembling schizophrenia in healthy people, supporting the hypothesis that NMDA receptor hypofunction (especially on GABAergic interneurons) underlies schizophrenia. This has driven development of glycine-site partial agonists (D-cycloserine) and mGluR2/3 agonists.
PART VI: GLYCINE
Structure and Mechanism
- Formula: C₂H₅NO₂; MW = 75.03 g/mol - the simplest amino acid
- Structure: H₂N-CH₂-COOH
- Primary inhibitory transmitter of the spinal cord and brainstem; uses glycine receptor (GlyR)
- GlyR is a pentameric Cl⁻ channel (like GABA-A); composed of α1-4 and β subunits; strychnine-sensitive
- Also serves as a co-agonist (not the primary agonist) at the NMDA receptor glycine site (GluN1)
Glycine antagonist:
- Strychnine: Competitive antagonist at glycine receptor → uninhibited motor neuron firing → tetanic spasms (rat poison)
PART VII: HISTAMINE
Structure and Receptors (Kaplan & Sadock, p. 450-451)
- Formula: C₅H₉N₃; MW = 111.15 g/mol
- Structure: Imidazole ring (5-membered ring with two nitrogens) attached to an ethylamine chain
- Synthesis: L-Histidine → Histamine (by histidine decarboxylase, requires B6 cofactor)
- CNS source: Tuberomammillary (TMN) nucleus of the posterior hypothalamus
- Function: Wakefulness/arousal, appetite regulation, cognition
- Degradation: Histamine methyltransferase (brain); diamine oxidase (periphery)
| Receptor | G-protein | Location | Effect |
|---|---|---|---|
| H1 | Gq → ↑IP3/Ca²⁺ | Brain (neurons + glia), smooth muscle, endothelium | Wakefulness; bronchoconstriction, vasodilation, itch |
| H2 | Gs → ↑cAMP | Parietal cells of stomach, heart, brain | ↑Gastric acid secretion |
| H3 | Gi → ↓cAMP | Presynaptic autoreceptor in brain (also heteroreceptor) | Inhibits histamine release; also inhibits ACh, DA, NE, 5-HT release |
| H4 | Gi → ↓cAMP | Immune cells (eosinophils, mast cells), bone marrow | Allergic/immune modulation |
H1 antagonists (antihistamines):
- First-generation (CNS-penetrant): Diphenhydramine (Benadryl), chlorpheniramine, promethazine - sedating (block H1 in brain); also have anticholinergic effects
- Second-generation (non-sedating): Cetirizine, loratadine, fexofenadine - do not cross BBB
- H3 inverse agonists: Pitolisant (Wakix) - approved for narcolepsy (increases histamine, ACh, DA, NE release in cortex)
H2 antagonists:
- Ranitidine (withdrawn), famotidine, cimetidine - reduce gastric acid; used for peptic ulcer, GERD
Summary Table: Receptor Signal Transduction
| NT | Receptor | Type | G-protein | Second Messenger |
|---|---|---|---|---|
| Dopamine | D1, D5 | GPCR | Gs | ↑cAMP |
| Dopamine | D2, D3, D4 | GPCR | Gi | ↓cAMP |
| NE/Epi | α1 | GPCR | Gq | ↑IP3/DAG/Ca²⁺ |
| NE/Epi | α2 | GPCR | Gi | ↓cAMP |
| NE/Epi | β1, β2, β3 | GPCR | Gs | ↑cAMP |
| ACh | Muscarinic M1, M3, M5 | GPCR | Gq | ↑IP3/DAG/Ca²⁺ |
| ACh | Muscarinic M2, M4 | GPCR | Gi | ↓cAMP; ↑GIRK |
| ACh | Nicotinic (nAChR) | Ligand-gated ion channel | N/A | Na⁺/K⁺ flux (Ca²⁺ via α7) |
| 5-HT | 5-HT1A/1B/1D | GPCR | Gi | ↓cAMP, ↑GIRK |
| 5-HT | 5-HT2A/2B/2C | GPCR | Gq | ↑IP3/DAG/Ca²⁺ |
| 5-HT | 5-HT3 | Ligand-gated ion channel | N/A | Na⁺/K⁺ (cation influx) |
| 5-HT | 5-HT4, 5-HT6, 5-HT7 | GPCR | Gs | ↑cAMP |
| GABA | GABA-A | Ligand-gated ion channel | N/A | Cl⁻ influx (inhibitory) |
| GABA | GABA-B | GPCR heterodimer | Gi/Go | ↓cAMP; ↑GIRK; ↓Ca²⁺ |
| Glutamate | AMPA | Ligand-gated ion channel | N/A | Na⁺/K⁺ (Ca²⁺ if no GluA2) |
| Glutamate | NMDA | Ligand-gated ion channel | N/A | Na⁺/K⁺/Ca²⁺ (voltage+ligand gated) |
| Glutamate | mGluR I (1,5) | GPCR | Gq | ↑IP3/DAG/Ca²⁺ |
| Glutamate | mGluR II/III (2-8) | GPCR | Gi | ↓cAMP |
| Histamine | H1 | GPCR | Gq | ↑IP3/DAG/Ca²⁺ |
| Histamine | H2 | GPCR | Gs | ↑cAMP |
| Histamine | H3, H4 | GPCR | Gi | ↓cAMP |
| Glycine | GlyR | Ligand-gated ion channel | N/A | Cl⁻ influx (inhibitory) |
Key References Used
-
Kandel ER, Koester JD, Mack SH, Siegelbaum SA - Principles of Neural Science, 6th Edition (2021) - Chapters on NMJ, nicotinic ACh receptor structure/function, synaptic transmission, LTP. [Textbook available in library as ISBN 9781259642241]
-
Sadock BJ, Sadock VA, Ruiz P - Kaplan & Sadock's Comprehensive Textbook of Psychiatry, 10th Edition - Chapters 1.7 and 1.6 on catecholamines, serotonin, GABA, glutamate, histamine, neuropeptides (pp. 418-530). [ISBN 9781975175733]
-
Brunton LL, Hilal-Dandan R, Knollmann BC - Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th Edition - Dopamine agonist/antagonist pharmacology. [ISBN 9781264258079]
-
Katzung BG - Basic and Clinical Pharmacology, 16th Edition - Parkinson's pharmacology, dopamine agonists. [ISBN 9781260463309]
-
Barrett KE, Barman SM, Brooks HL, Yuan JX-J - Ganong's Review of Medical Physiology, 26th Edition - Catecholamine synthesis, catabolism, adrenergic pharmacology. [ISBN 9781260122404]
-
Rodwell VW, Bender DA, Botham KM et al. - Harper's Illustrated Biochemistry, 32nd Edition - Tyrosine hydroxylase and catecholamine biosynthesis.
-
Siegel GJ, Albers RW, Brady S, Price DL - Basic Neurochemistry: Molecular, Cellular, and Medical Aspects (Siegel's) - Referenced throughout for molecular mechanisms of receptor-channel coupling, second messenger systems, and GABA receptor pharmacology.
Clinical Pearls to Remember:
- The NMDA receptor is the brain's "coincidence detector" - it requires BOTH presynaptic activity (glutamate) AND postsynaptic depolarization (to relieve Mg²⁺ block) - the molecular basis of Hebb's rule ("cells that fire together, wire together") and thus learning and memory (LTP).
- Benzodiazepines ↑ frequency of Cl⁻ channel opening; Barbiturates ↑ duration - both require GABA; at very high barbiturate doses, the channel opens without GABA (explains lethality in overdose vs. BZD safety).
- The catecholamine synthesis pathway is a single linear sequence: the key drug targets are tyrosine hydroxylase (rate-limiting; blocked by metyrosine), AADC (blocked by carbidopa at periphery), DBH (blocked by disulfiram), VMAT (blocked by reserpine), MAO (blocked by MAOIs), COMT (blocked by entacapone/tolcapone).
- Kandel's key insight at the nicotinic synapse: Two ACh molecules must bind one alpha subunit each → conformational change through all 5 subunits → M2 helices rotate to open the pore → Na⁺ enters, K⁺ exits, net depolarization. This is the basis of all ionotropic receptor pharmacology.
This is a shared conversation. Sign in to Orris to start your own chat.