In nondepolarizing skeletal muscle relaxant why tof fade whereas in depolarizing block constant but diminished in phase one while fade in phase two
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have all the information needed for a comprehensive answer. Here it is:
TOF Fade: Nondepolarizing vs. Depolarizing Block — Mechanistic Explanation
Quick Summary Table
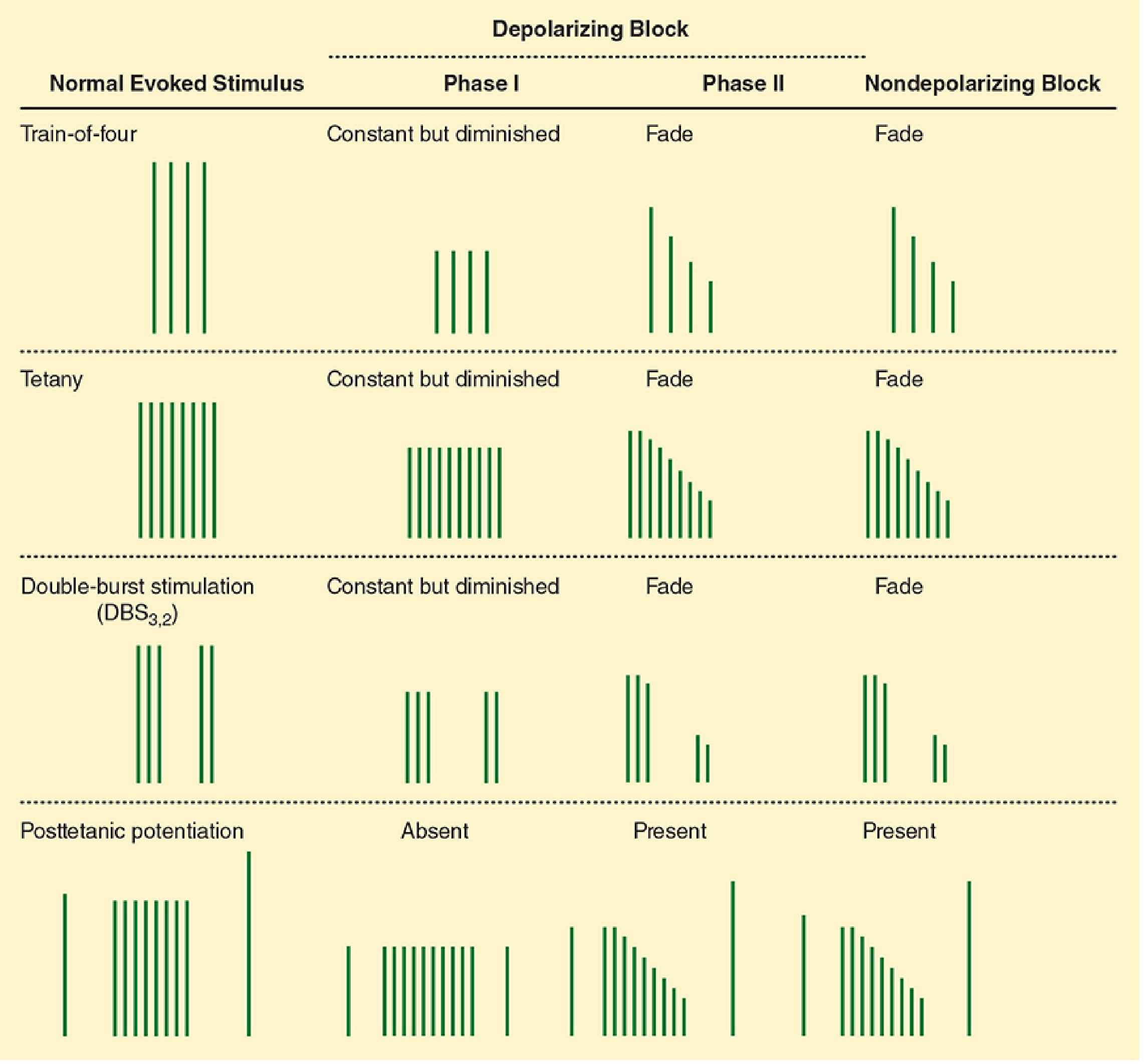
| Stimulus | No Drug | Nondepolarizing | Depolarizing Phase I | Depolarizing Phase II |
|---|---|---|---|---|
| TOF | TOF-R = 1.0 | Fade (TOF-R < 1.0) | Constant but diminished (TOF-R = 1.0) | Fade (TOF-R < 1.0) |
| Tetany | Sustained | Fade | Sustained but diminished | Fade |
| Posttetanic potentiation | Present | Present | Absent | Present |
1. Nondepolarizing Block → TOF Fades
The Prejunctional Mechanism
The key is the prejunctional (presynaptic) α3β2 neuronal nicotinic receptor on the motor nerve terminal.
Under normal conditions, this receptor acts as a positive-feedback mobilization sensor: when nerve firing rate increases (e.g., during repeated stimulation), released ACh binds to these prejunctional nicotinic receptors, signaling the nerve to mobilize ACh from the reserve pool into the readily releasable pool — maintaining transmitter supply during high-demand stimulation.
Nondepolarizing NMBDs (e.g., rocuronium, vecuronium, atracurium) have high affinity for this prejunctional α3β2 receptor and block it. Additionally, they block prejunctional sodium channels, further impairing ACh mobilization.
Consequence during TOF (4 stimuli at 2 Hz):
- T1: ACh is still sufficient from the immediately releasable pool → normal (diminished) response
- T2, T3, T4: ACh mobilization is progressively impaired because the prejunctional feedback loop is blocked → less and less ACh released with each successive stimulus → T4 < T3 < T2 < T1 = fade
- TOF ratio (T4/T1) falls well below 1.0
"Although most nondepolarizing NMBDs have a distinct affinity for the α3β2 cholinergic receptor, succinylcholine lacks this affinity. The action of nondepolarizing versus depolarizing NMBDs at this neuronal cholinergic receptor explains the typical fade phenomenon after any nondepolarizing drugs, and the lack of such effect in the clinical dose range for succinylcholine." — Miller's Anesthesia, 10e
2. Depolarizing Block Phase I → TOF Constant but Diminished (TOF-R = 1.0)
Mechanism of Phase I Block
Succinylcholine (SCh) binds postsynaptic nicotinic receptors and causes persistent depolarization of the end plate. The membrane stays depolarized and cannot repolarize (because SCh is not hydrolyzed by AChE at the cleft — only by plasma pseudocholinesterase). This produces flaccid paralysis by depolarization block (the voltage-gated Na⁺ channels in the perijunctional zone become inactivated during sustained depolarization).
Why no fade?
- SCh does not bind the prejunctional α3β2 receptor → the ACh mobilization feedback loop is intact and undisturbed
- Each of the 4 TOF stimuli still releases comparable amounts of ACh
- But the postsynaptic end plate is already depolarized/inactivated → all 4 responses are equally and uniformly reduced
- T1 = T2 = T3 = T4 → TOF-R = 1.0 (constant, just smaller in amplitude)
- No posttetanic potentiation either (the block is not competitive/surmountable by more ACh)
3. Depolarizing Block Phase II → TOF Fades (resembles nondepolarizing)
Mechanism of Phase II (Desensitization) Block
With prolonged or large-dose SCh exposure, the character of the block changes and begins to mimic a nondepolarizing block. Several mechanisms contribute:
- Receptor desensitization: The nicotinic receptor undergoes conformational change to a desensitized state — the channel closes (even though agonist is still bound) and the end plate repolarizes, but the receptor is now unresponsive to further ACh or SCh. This is a closed-channel block state.
- Open-channel block: At high concentrations, SCh can enter and plug the open ion channel, contributing to progressive block.
- Ion redistribution: Prolonged membrane depolarization leads to Na⁺ influx and K⁺ efflux, altering the electrochemical gradient.
Why fade appears in Phase II:
Because the receptor is now in a desensitized/blocked state (not simply persistently depolarized), the block becomes surmountable in a manner analogous to nondepolarizing block. ACh mobilization may now become a limiting factor, and the postsynaptic receptor population responding to each successive stimulus is progressively compromised → fade reappears, posttetanic potentiation returns, and the block can be partially reversed by neostigmine (once SCh plasma concentration is negligible).
"Phase II block is frequently referred to as a desensitization block, but it should not be because desensitization of receptors is only one of many phenomena that contribute to the process." — Miller's Anesthesia, 10e
Summary of the Logic
| Prejunctional receptor blocked? | ACh mobilization impaired? | Postsynaptic mechanism | TOF result | |
|---|---|---|---|---|
| Nondepolarizing | ✅ Yes (α3β2 blocked) | ✅ Yes | Competitive postsynaptic antagonism | Fade |
| Phase I SCh | ❌ No | ❌ No | Persistent end-plate depolarization → inactivation | Constant, diminished |
| Phase II SCh | Partially | Partially | Desensitization + channel block → nondepolarizing-like | Fade |
The single most important concept: TOF fade is a prejunctional phenomenon. Nondepolarizing drugs cause fade by blocking the presynaptic α3β2 autoreceptor that normally maintains ACh mobilization. Succinylcholine in Phase I lacks this prejunctional effect entirely — hence constant (but diminished) responses. Phase II emerges when the block character shifts toward a desensitization/channel-block pattern where progressive failure occurs with each successive stimulus.
— Miller's Anesthesia 10e, pp. 3227–3228; Morgan & Mikhail's Clinical Anesthesiology 7e, pp. 377–378; Katzung's Basic & Clinical Pharmacology 16e, p. 752
This is a shared conversation. Sign in to Orris to start your own chat.