Carcinod syndrome of gastrointestinal tract
Reading File
Finding Sources
Searching PubMed
"carcinoid syndrome" AND "gastrointestinal" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple major textbooks. Let me compile the complete answer.
Carcinoid Syndrome of the Gastrointestinal Tract
Definition and Background
Carcinoid syndrome is a clinical constellation of symptoms caused by functional neuroendocrine tumors (NETs), also called carcinoid tumors, that secrete excessive biologically active substances - predominantly serotonin - into the systemic circulation. It develops in approximately 8-30% of patients with GI-NETs, almost exclusively in the setting of hepatic metastases (>90% of cases), because the liver normally inactivates vasoactive substances before they reach systemic circulation.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Sabiston Textbook of Surgery
Tumor Origin and Epidemiology
GI carcinoids arise from enterochromaffin (Kulchitsky) cells throughout the gut. The most common site is the small intestine (midgut/ileum), followed by the appendix and rectum. Midgut NETs most commonly cause the "typical" carcinoid syndrome because they are high serotonin producers.
- Foregut NETs (stomach, duodenum, bronchus) - more likely to cause atypical syndrome via histamine
- Midgut NETs (jejunum, ileum, right colon) - classic carcinoid syndrome
- Hindgut NETs (left colon, rectum) - rarely secrete and rarely cause syndrome
Pathophysiology
Typical Carcinoid Syndrome (Midgut)
The rate-limiting step is hydroxylation of tryptophan to 5-hydroxytryptophan (5-HTP), which is then rapidly converted to serotonin (5-HT) by aromatic L-amino acid decarboxylase. Serotonin is stored in neurosecretory granules or released into circulation. Most circulating 5-HT is:
- Taken up and stored by platelets
- Metabolized to 5-hydroxyindoleacetic acid (5-HIAA) by monoamine oxidase and aldehyde dehydrogenase
- 5-HIAA is excreted in the urine - the key diagnostic marker
Atypical Carcinoid Syndrome (Foregut/Gastric)
These tumors are deficient in aromatic L-amino acid decarboxylase and cannot convert 5-HTP to serotonin, so 5-HTP itself is secreted. Plasma serotonin is normal, but urinary 5-HT can be elevated (5-HTP is decarboxylated to 5-HT in the kidney). Histamine mediates the atypical flush.
Why Liver Metastases are Required
Serotonin, tachykinins, and metabolites are efficiently cleared by the liver via first-pass metabolism. Systemic carcinoid syndrome only manifests when:
-
Liver metastases are present (tumor secretes directly into hepatic veins)
-
Rarely: primary retroperitoneal or ovarian tumors that bypass portal circulation
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 512
Clinical Features
| Feature | At Presentation (%) | During Disease Course (%) |
|---|---|---|
| Flushing | 70 (range 23-100) | 78 (range 45-96) |
| Diarrhea | 69 (range 32-93) | 78 (range 58-100) |
| Carcinoid heart disease | 26 (range 11-40) | 30 (range 14-41) |
| Wheezing/bronchospasm | 11 (range 4-14) | 12 (range 3-18) |
| Pellagra | 2 (range 0-7) | 1 (range 0-5) |
From Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Table 34.11
1. Flushing
- Most common symptom; sudden onset deep red erythema of the face, neck, and upper chest
- May be associated with warmth, lacrimation, itching, palpitations, facial edema
- Precipitants: stress, alcohol, certain foods (cheese), exercise, catecholamines, calcium, pentagastrin
- Duration varies: brief (2-5 min) early; prolonged (hours) in later disease
- Typical (midgut) flush: salmon-pink to red, facial and neck, non-pruritic
- Gastric (atypical) flush: red, patchy, pruritic, with wheals and central clearing, provoked by food
- Repeated flushing leads to permanent telangiectasia and cyanotic discoloration
2. Diarrhea
- Usually watery; 2-30 stools/day
- Occurs with flushing in 85% of cases, alone in 15%
- Caused by increased 5-HT-mediated colonic motility and shortened intestinal transit
- Steatorrhea may occur in some patients
- Fecal output <1 L/day in most (60%) patients
3. Bronchospasm
- Wheezing and asthma-like symptoms
- Mediated by serotonin in combination with histamine
4. Carcinoid Heart Disease (Hedinger Syndrome)
This is the most serious long-term complication, occurring in up to 70% of patients with carcinoid syndrome. Serotonin is the primary pathogenetic factor, causing fibrous plaques composed of smooth muscle cells, myofibroblasts, and elastic tissue on the right-sided endocardium and valves (the right heart bears the initial burden of elevated serotonin before it is inactivated in the lungs).
Cardiac lesions:
- Tricuspid valve: plaques on ventricular side of leaflets → tricuspid regurgitation (47%); tricuspid stenosis (42%)
- Pulmonary valve: predominant lesion is stenosis (90%)
- Left-sided involvement only if patent foramen ovale is present
Clinical presentation: dyspnea, right-sided heart failure, peripheral edema
Echocardiography: thickening of tricuspid valve and subvalvular apparatus; in severe disease, leaflets are retracted and fixed with loss of coaptation
5. Pellagra
- Rare complication (~2%)
- Results from excessive tryptophan diversion toward serotonin synthesis, leading to niacin deficiency
- Manifests as dermatitis, diarrhea, and dementia (the classic "3 Ds")
Diagnosis
Biochemical Markers
| Test | Details |
|---|---|
| 24-hour urine 5-HIAA | Primary diagnostic test; elevated in >90% of carcinoid syndrome cases; normal values <10 mg/day |
| Serum Chromogranin A (CgA) | Elevated in >80% of NETs; useful for monitoring tumor burden and disease recurrence; prognostic value |
| Plasma/urine 5-HTP | Elevated in atypical (foregut) syndrome |
| Urinary 5-HT | Elevated when 5-HTP is converted in kidney (atypical syndrome) |
Dietary note: Foods that may falsely elevate 5-HIAA include bananas, avocados, eggplant, pineapples, plums, walnuts, and tomatoes. These should be avoided before the 24-hour collection.
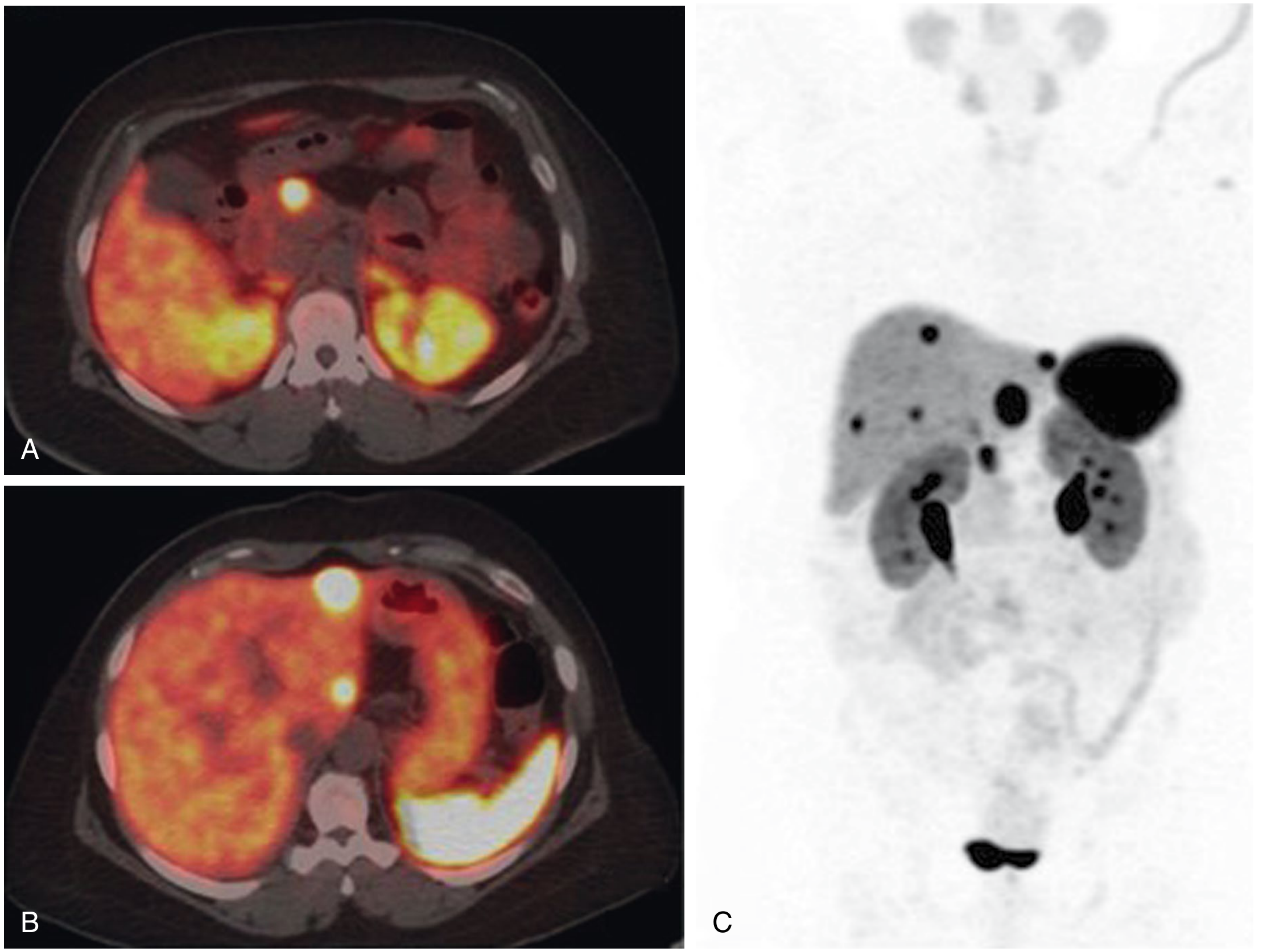
Imaging
- Somatostatin receptor scintigraphy (OctreoScan) - detects primary tumors and metastases using radiolabeled octreotide; exploits the high density of somatostatin receptors on NETs
- PET-DOTATATE scan - higher sensitivity than OctreoScan; can detect occult primaries and assess metastatic burden
- CT/MRI abdomen - assess liver metastases and primary tumor
- Echocardiography - mandatory in all patients with carcinoid syndrome to assess valvular disease
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 992
Treatment
1. Somatostatin Analogues (SSAs) - Mainstay of Medical Therapy
- Octreotide (short-acting and long-acting LAR formulation) and lanreotide are the standard of care
- Reduce both flushing and diarrhea by inhibiting secretion of vasoactive substances
- Shown to improve progression-free survival and quality of life in unresectable disease
- LAR (long-acting repeatable) formulations allow monthly dosing
2. Surgical Treatment
- Resection of primary tumor and hepatic debulking where feasible
- Even partial debulking (>90% reduction in tumor burden) can meaningfully reduce symptoms
- Octreotide cover is mandatory perioperatively to prevent carcinoid crisis (from liberation of vasoactive substances during tumor handling)
3. Peptide Receptor Radionuclide Therapy (PRRT)
- Lutetium-177-DOTATATE (^177Lu-DOTATATE) for refractory or progressive disease on SSAs
- Radiolabeled SSA delivers radiation directly to somatostatin receptor-expressing tumor cells
4. Other Modalities
- Hepatic embolization/chemoembolization for liver-dominant disease (but can precipitate carcinoid crisis - requires octreotide prophylaxis)
- Chemotherapy: generally not very sensitive; interferon-alpha may have some role
- Valve replacement surgery for severe carcinoid heart disease: operative mortality now <10%; without treatment, mean survival with carcinoid heart disease is only 1.6 years
5. Symptomatic Management
- Antidiarrheals (loperamide, codeine)
- Antihistamines (H1 + H2) for gastric (histamine-mediated) atypical flushing
- Avoid trigger foods and sympathomimetic drugs
Carcinoid Crisis
A life-threatening emergency occurring from sudden massive release of vasoactive substances, typically triggered by:
- Tumor manipulation (biopsy, surgical resection)
- Sympathomimetic drugs (amphetamines, albuterol)
- Cytolytic therapies (hepatic embolization)
- Spontaneous
Presentation: severe hemodynamic instability, profound flushing, profuse diarrhea, diffuse bronchospasm
Management: IV octreotide bolus (500 mcg) immediately; supportive hemodynamic care
- Sabiston Textbook of Surgery
Prognosis
Patients with symptomatic carcinoid syndrome have worse prognosis than those without:
- Median overall survival with carcinoid syndrome: 4.7 years
- Median overall survival without carcinoid syndrome: 7.1 years
NETs generally grow more slowly than most metastatic malignancies, and patients may live with metastatic disease for many years, particularly with modern SSA and PRRT therapy.
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Table 34.11 and section on Carcinoid Syndrome
- Sabiston Textbook of Surgery, pp. 1615-1617
- Goldman-Cecil Medicine, Chapter 47 (Carcinoid Heart Disease)
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 992
Investigation in case of malabsorption syndrome
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I have comprehensive content from multiple authoritative textbooks. Let me compile the full structured answer.
Investigations in Malabsorption Syndrome
Malabsorption results from impaired nutrient absorption at one or more of three levels: intraluminal processing (digestion), mucosal absorption, or post-mucosal transport (lymphatic/vascular). The investigation strategy is stepwise - first confirm malabsorption exists, then identify whether the defect is luminal (pancreatic/biliary), mucosal, or post-mucosal, then establish the specific cause.
STEP 1: Routine Screening Investigations
These are the first-line tests that raise suspicion for malabsorption and quantify its consequences:
Blood Tests
| Test | Finding in Malabsorption | Significance |
|---|---|---|
| CBC / Haemogram | Microcytic anaemia (iron deficiency), macrocytic anaemia (B12/folate), normocytic anaemia | Reflects deficiency of iron, folate, or B12 |
| Serum iron, ferritin, TIBC | Low iron and ferritin, raised TIBC | Iron malabsorption (proximal small bowel) |
| Serum folate / RBC folate | Reduced | Proximal jejunal mucosal disease (e.g., celiac) |
| Serum vitamin B12 | Reduced | Ileal disease or bacterial overgrowth |
| Serum albumin | Reduced (hypoalbuminaemia) | Protein malabsorption or protein-losing enteropathy |
| Serum calcium | Reduced (tetany possible) | Calcium/vitamin D malabsorption |
| Serum magnesium, phosphate | Reduced | Widespread mucosal malabsorption |
| Prothrombin time (PT/INR) | Prolonged | Vitamin K malabsorption (fat-soluble vitamin) |
| Serum cholesterol | Reduced | Fat malabsorption (low dietary fat absorption) |
| Serum carotenoids (carotene) | Reduced | Simple, useful screening test for steatorrhoea - carotene absorption depends on dietary fat; also low in liver disease and high fever |
| Liver function tests | May be elevated | Biliary/hepatic cause of maldigestion |
| ESR / CRP | Elevated | Inflammatory bowel disease, Whipple disease |
| TSH | Low or high | Hyperthyroidism (accelerated transit) or hypothyroidism (elevated carotenoids) |
Key screening panel: Haemoglobin, MCV, serum iron/ferritin, folate, B12, albumin, calcium, PT, and serum carotene. Abnormalities in these point strongly toward malabsorption and direct further testing.
- Tietz Textbook of Laboratory Medicine, 7th Edition and Henry's Clinical Diagnosis and Management by Laboratory Methods
STEP 2: Stool Examination
Qualitative Fecal Fat (Sudan III Stain)
- Stool smear stained with Sudan III or Sudan IV stain
- Presence of fat globules (>6 fat globules per high-power field, diameter >8 µm) = steatorrhoea
- Simple, cheap, rapid screening test
- Sensitivity ~75-95% for significant steatorrhoea
Quantitative Fecal Fat (72-hour fecal fat estimation)
- Gold standard for steatorrhoea
- Patient consumes a high-fat diet (70-100 g fat/day) for 2 days before and throughout the collection period
- Stool collected for 72 hours (3 days)
- Normal: <7 g fat excreted per 24 hours (i.e., >93% dietary fat absorbed)
- >7 g/day = steatorrhoea confirmed
- Borderline (8-14 g/day) may occur in secretory/osmotic diarrhoea not due to fat malabsorption
- Limitations: cumbersome, patient compliance poor, requires accurate dietary fat intake records
Fecal Reducing Substances
- Test for carbohydrate malabsorption (especially in children)
- Positive (>0.5% reducing sugars) = carbohydrate malabsorption
Stool for Ova, Cysts, and Parasites (OCP)
- Giardia lamblia is an important treatable cause of malabsorption
- PCR for Giardia or stool antigen-capture ELISA should also be done
Fecal Osmotic Gap
-
Distinguishes osmotic from secretory diarrhoea
-
Osmotic gap = 290 - 2 × (stool Na + stool K)
-
Gap >125 mOsm/kg = osmotic (carbohydrate malabsorption typical)
-
Gap <50 mOsm/kg = secretory diarrhoea
-
Goldman-Cecil Medicine, Table 126-6
STEP 3: Tests for Specific Types of Malabsorption
A. Tests for Fat Malabsorption / Pancreatic Function
Fecal Elastase-1
- Elastase-1 is a pancreatic enzyme that survives intestinal transit intact and is 5-6 times concentrated in feces
- A single 100 mg stool sample is sufficient
- Cutoff: <200 µg/g stool = pancreatic insufficiency
- Sensitivity for severe pancreatic insufficiency is high; less sensitive for mild disease
- Unaffected by pancreatic enzyme replacement therapy
- Better than fecal chymotrypsin, bentiromide (NBT-PABA), and pancreo-lauryl tests
¹³C Mixed-Chain Triglyceride Breath Test
- Patient given ¹³C-labeled medium- and long-chain fatty acids orally with a standard meal (toast and butter)
- Breath samples collected over 5 hours; exhaled ¹³CO₂ expressed as % of administered dose
- Normal: 25-40% excretion
- Sensitivity 89%, specificity 81% for pancreatic insufficiency
¹⁴C-Triolein Breath Test
- Oral ¹⁴C-labeled triglyceride → measures ¹⁴CO₂ in expired air
- Decreased expiration = decreased triglyceride absorption (steatorrhoea from any cause)
- Two-stage test: if ¹⁴CO₂ increases with oral pancreatic enzyme supplementation in the second stage → pancreatic insufficiency confirmed; no change → mucosal/other cause
- Limitation: requires scintillation counter and isotope facilities
Secretin-Cholecystokinin (CCK) Test / Direct Pancreatic Function Tests
- Gold standard for exocrine pancreatic function
- IV secretin or CCK given; duodenal aspirate collected and analyzed for bicarbonate and enzyme output
- Reduced bicarbonate concentration or enzyme output = exocrine pancreatic insufficiency
- Invasive but most sensitive for mild-moderate pancreatic insufficiency
Serum Lipase and Amylase
- Markedly elevated in acute pancreatitis; may be low or normal in chronic pancreatic insufficiency
B. Tests for Mucosal (Enterogenous) Malabsorption
D-Xylose Absorption Test
- Most valuable differential diagnostic test for distinguishing mucosal malabsorption from pancreatic maldigestion
- D-xylose (a pentose sugar not normally found in the body or diet) is passively absorbed in the small intestine without requiring pancreatic enzymes
- Procedure: 25 g D-xylose in water is given orally after overnight fast
- Urine collected for 5 hours; normal excretion >4-5 g in 5 hours
- <3 g excreted = enterogenous (mucosal) malabsorption (proximal small bowel disease)
- Normal D-xylose with steatorrhoea = pancreatic insufficiency (pancreatic enzymes not needed for xylose, so xylose absorbed normally)
- Caveat: In renal disease, urine values unreliable - measure blood D-xylose at 2 hours instead (normal: >20 mg/dL)
- False-positive (low urine xylose) also in: ascites, delayed gastric emptying, vomiting, SIBO (bacteria catabolize xylose in the gut)
Lactose Tolerance Test / Lactose Hydrogen Breath Test
- Used to diagnose lactase deficiency (most common disaccharidase deficiency)
- Lactose tolerance test: 50 g oral lactose load; blood glucose rise <20 mg/dL above fasting + symptoms = positive
- Lactose hydrogen breath test (preferred):
- 50 g lactose orally; breath H₂ measured at 0, 30, 60, 90, 120, 180 min
- Rise in H₂ ≥20 ppm above baseline = lactase deficiency (unabsorbed lactose fermented by colonic bacteria → H₂)
- Cannot differentiate primary from secondary lactase deficiency
- These two tests agree in ~95% of cases
Hydrogen Breath Test for Bacterial Overgrowth (SIBO)
- Lactulose hydrogen breath test or glucose hydrogen breath test
- Lactulose or glucose given orally; breath H₂ measured serially
- Two-peak pattern (early small bowel peak + late colonic peak) = SIBO
- Glucose breath test: early H₂ rise >12-20 ppm above baseline = SIBO
- Also: jejunal aspirate culture (>10⁵ CFU/mL = gold standard for SIBO)
Bile Acid Malabsorption Tests (ileal function)
- SeHCAT (selenium-homocholic acid taurine) scan: radiolabeled synthetic bile acid given orally; whole-body retention measured at 7 days; <15% retention = bile acid malabsorption
- Useful in terminal ileal disease (Crohn disease), post-ileal resection diarrhoea
C. Test for Terminal Ileal Function
Schilling Test (Vitamin B12 Absorption)
- Oral radioactive ¹⁴C- or ⁵⁷Co-labeled vitamin B12 → large intramuscular "flushing" dose of non-radioactive B12 given simultaneously
- Urine collected for 24 hours; radioactivity measured
- Stage 1 (B12 alone): Low urinary radioactivity = B12 malabsorption
- Stage 2 (B12 + Intrinsic Factor): If corrected by IF → pernicious anaemia / gastric cause
- If NOT corrected → ileal disease, SIBO, or pancreatic insufficiency
- Stage 3 (B12 + IF + antibiotics): If corrected → SIBO
- Largely replaced by serum B12 + IF antibody testing + Methylmalonic acid (MMA) levels in modern practice
STEP 4: Serological Tests for Specific Diseases
| Test | Disease |
|---|---|
| Anti-tissue transglutaminase IgA (anti-tTG IgA) | Celiac disease (sensitivity ~95%, specificity ~98%) |
| Anti-endomysial antibody (EMA IgA) | Celiac disease (highly specific) |
| Total serum IgA | Must be checked alongside celiac serology; IgA deficiency gives false-negative results |
| Anti-deamidated gliadin peptide (DGP IgG) | Celiac disease in IgA-deficient patients |
| Stool antigen ELISA / PCR for Giardia | Giardiasis |
| Serum gastrin | Zollinger-Ellison syndrome (gastrinoma) |
| Chromogranin A, urinary 5-HIAA | Carcinoid syndrome |
| VIP levels | VIPoma |
| Blood culture / PAS-positive macrophages on biopsy | Whipple disease (Tropheryma whipplei) |
| HIV serology | HIV enteropathy |
| Sweat chloride test | Cystic fibrosis (children) |
STEP 5: Endoscopy and Biopsy
Upper GI Endoscopy + Duodenal Biopsy
- Standard of care for suspected mucosal disease
- At least 4-6 biopsies from D2/D3 recommended for celiac disease
- Histological findings guide diagnosis:
- Celiac disease: villous atrophy, crypt hyperplasia, increased intraepithelial lymphocytes (Marsh classification)
- Whipple disease: PAS-positive foamy macrophages in lamina propria
- Giardiasis: trophozoites attached to epithelium, mild villous blunting
- Lymphoma / lymphangiectasia / amyloidosis: characteristic appearances
- SIBO: variable, often normal or mild changes
Push Enteroscopy / Video Capsule Endoscopy
- For visualization of mid/distal small bowel beyond reach of standard endoscope
- Useful for Crohn's disease, NSAID enteropathy, small bowel tumours
Colonoscopy with Terminal Ileum Biopsy
- Assess terminal ileum (Crohn's disease, TB)
STEP 6: Imaging Studies
Plain X-ray Abdomen
- Pancreatic calcification → chronic pancreatitis (exocrine insufficiency)
- Dilated loops of bowel → obstruction / SIBO predisposition
Barium Follow-Through / Small Bowel Enteroclysis
- Demonstrates structural small bowel abnormalities
- Findings: flocculation/segmentation of barium (celiac), mucosal thickening (Crohn, lymphoma), strictures, fistulae, blind loops (SIBO), jejunal diverticulosis
CT Enterography / MR Enterography
- Now largely replaced barium enteroclysis as preferred cross-sectional small bowel imaging
- Detects: mucosal changes, mesenteric lymphadenopathy, bowel wall thickening, strictures, fistulae
- CT can also show: pancreatic calcification, pancreatic atrophy, biliary dilatation
- MRI avoids radiation; preferred in younger patients and follow-up imaging
Ultrasound Abdomen
- Non-invasive, no radiation
- Biliary obstruction, pancreatic disease (calcifications, duct dilatation, stones)
- Small bowel wall thickening (Crohn's, Whipple's - hyperechoic appearance)
- Mesenteric lymph nodes
MRCP / ERCP
- MRCP: non-invasive assessment of biliary and pancreatic duct anatomy
- ERCP: gold standard for biliary/pancreatic ductal disease; also therapeutic (stenting, stone removal)
- Distinguishes chronic pancreatitis from pancreatic tumours
¹¹¹In-Octreotide Scintigraphy / PET-DOTATATE
- For neuroendocrine tumours (gastrinoma, somatostatinoma) causing malabsorption
STEP 7: Special Tests in Selected Cases
| Test | Indication |
|---|---|
| Jejunal juice culture (>10⁵ CFU/mL) | Gold standard for SIBO |
| Sweat chloride test | Cystic fibrosis |
| Lymphocyte subset analysis | Immunodeficiency (hypogammaglobulinaemia, common variable immunodeficiency) |
| Serum immunoglobulins | Hypogammaglobulinaemia, IgA deficiency |
| Fecal calprotectin | Distinguishes IBD from IBS; elevated in IBD and mucosal inflammation |
| Fecal alpha-1 antitrypsin | Protein-losing enteropathy |
| Bone density (DEXA scan) | Osteopenia/osteoporosis from calcium + vitamin D malabsorption |
| Urinary oxalate | Hyperoxaluria in fat malabsorption (enteric hyperoxaluria → renal stones) |
| Cellobiose-mannitol / lactulose-mannitol ratio | Gut permeability test for mucosal disease |
Summary Algorithm
Suspected Malabsorption
↓
Routine bloods (CBC, iron, folate, B12, albumin, Ca, PT, carotene)
+ Stool for OCP, fat (Sudan stain), reducing substances
↓
Steatorrhoea confirmed?
YES NO
↓ ↓
Fecal elastase Carbohydrate malabsorption tests
D-Xylose test (lactose/H₂ breath test)
Serum amylase/lipase Protein-losing enteropathy
(fecal alpha-1 antitrypsin)
↓
D-Xylose ABNORMAL D-Xylose NORMAL
(Mucosal disease) (Pancreatic/Biliary)
↓ ↓
Celiac serology Imaging pancreas (CT/MRCP)
Upper endoscopy + biopsy Fecal elastase
Capsule endoscopy Secretin stimulation test
↓
Specific diagnosis → targeted management
Sources:
- Henry's Clinical Diagnosis and Management by Laboratory Methods - Tests for Steatorrhoea and Malabsorption (pp. 394-396)
- Tietz Textbook of Laboratory Medicine, 7th Edition - Investigation of Maldigestion and Malabsorption (Box 52.8)
- Goldman-Cecil Medicine - Table 126-6: Tests for the Evaluation of Malabsorption
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease - Noninvasive Evaluation of GI Digestive and Absorptive Function (Ch. 104)
This is a shared conversation. Sign in to Orris to start your own chat.