Non vascular findings in venous doppler
Reading File
Finding Sources
Finding Sources
Searching the Web
non-vascular incidental findings venous doppler ultrasound DVT scan
Reading Web Page
https://radiologykey.com/nonvascular-findings-encountered-du…
Finding Sources
Finding Sources
Here is a thorough, organized overview of non-vascular findings encountered during venous Doppler (duplex) ultrasound:
Non-Vascular Findings in Venous Doppler Ultrasound
During a venous Doppler exam (typically done to rule out DVT), a variety of incidental non-vascular pathologies can be identified. These may be the actual cause of the patient's presenting complaint - limb pain, swelling, or tenderness. About 13% of patients undergoing DVT ultrasound have at least one incidental non-vascular finding; Baker's cyst is the most common (accounting for ~40% of incidentals).
They are broadly divided into:
COMMON Findings
1. Soft Tissue Edema
- Fluid collects in the subcutaneous fat
- Sonographic appearance: marbled or reticulated pattern with anechoic fluid collections between echogenic fat lobules
- Causes include elevated hydrostatic pressure (CHF, fluid overload, DVT, venous compression/obstruction) or reduced oncotic pressure
- Does not contain internal vascularity
- Lymphedema appears identical on ultrasound but results from lymphatic obstruction (malignancy, surgery, trauma, filariasis); may or may not be accompanied by lymph node enlargement
2. Hematoma
- History of trauma, vigorous exercise, surgery, or anticoagulation is typical
- Appearance varies by age:
- Acute - may appear anechoic or hyperechoic
- Subacute/organizing - complex, heterogeneous, may appear solid
- Chronic - can mimic a solid mass; retraction and fibrosis develop over time
- Key feature: no internal vascularity on color Doppler - distinguishes it from solid tumors and lymph nodes
- May compress or displace adjacent veins; if large enough, adjacent veins may be difficult to visualize
3. Lymph Nodes
- Most commonly encountered in the groin (inguinal), axilla, and cervical regions; also perivascular (around aorta, IVC, iliac vessels)
- Normal node: almond/kidney-bean shaped, hypoechoic peripheral mantle, echogenic central hilum with fat and vessels, usually <1 cm in short axis
- Color Doppler: arterial flow in hilum, branching from center to periphery (centripetal flow)
Distinguishing Inflammatory vs. Malignant Nodes
| Feature | Inflammatory/Benign | Malignant |
|---|---|---|
| Shape | Ovoid (short axis < half of long axis) | Rounder |
| Hilum | Central echogenic hilum intact | Hilum lost |
| Vascularity | Central hilar branching | Irregular, disordered, peripheral |
- Lymphadenopathy (enlarged nodes) can itself cause limb swelling via venous or lymphatic obstruction, and can be painful when inflamed
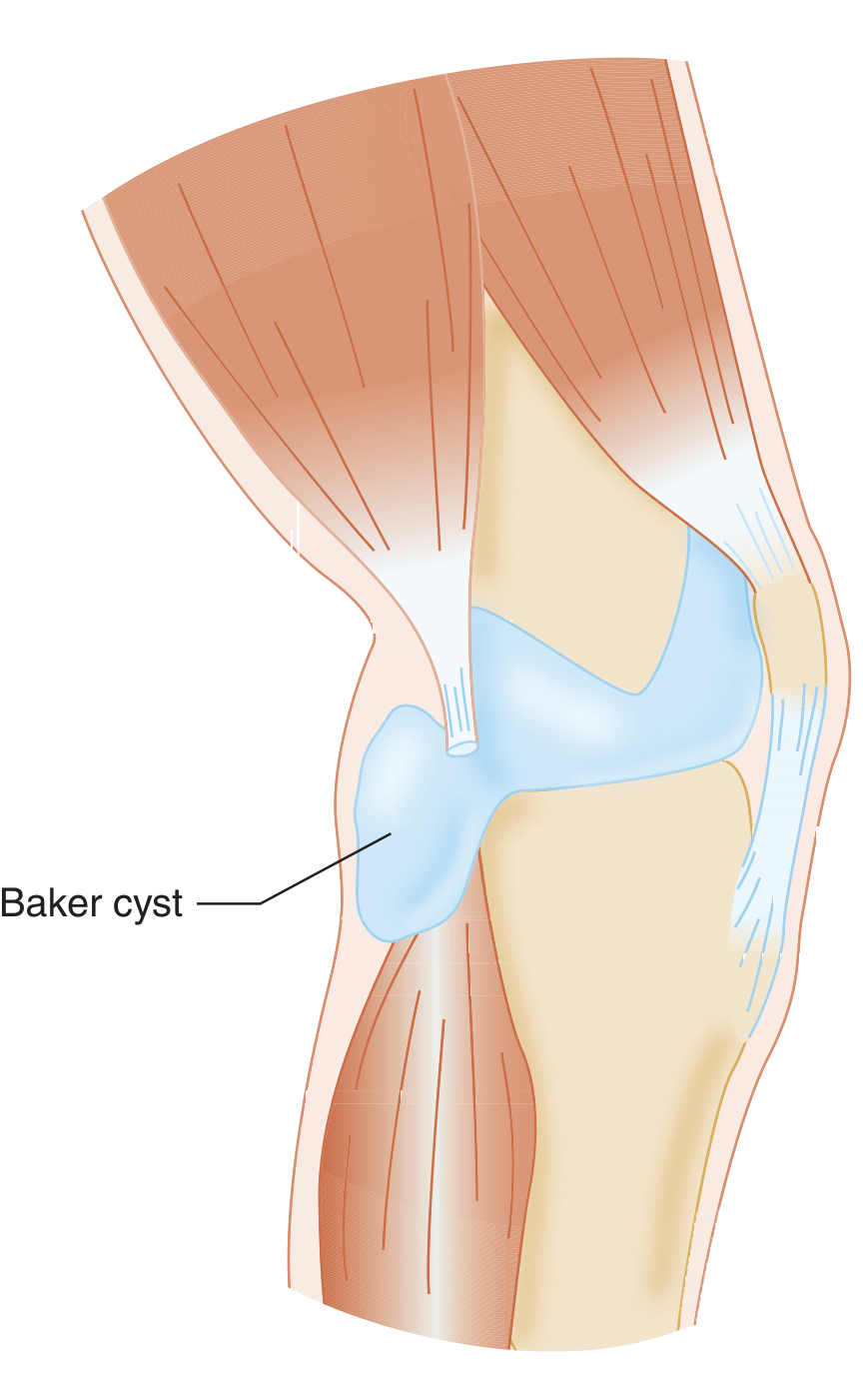
4. Popliteal (Baker's) Cyst
- Most common incidental finding on lower limb venous Doppler
- Located in the posteromedial popliteal fossa, between the medial head of gastrocnemius and the semimembranosus tendon
- Sonographic appearance: well-defined, thin-walled, anechoic cystic structure; may have internal debris if complicated
- Non-compressible and larger than adjacent veins
- Tracks toward the knee joint (helpful distinguishing feature)
- A ruptured Baker's cyst causes calf pain and swelling that can closely mimic DVT ("pseudothrombophlebitis syndrome"); may show ill-defined fluid tracking down the calf
- No internal vascularity
LESS COMMON Findings
5. Abscess
- Well-defined collection in soft tissues
- Appearance: simple to complex; may be purely fluid or contain internal echoes, septae, debris
- Gas bubbles appear as bright, echogenic foci with posterior shadowing (highly specific for gas-forming organisms)
- Peripheral vascularity in the wall on color Doppler
- Surrounding echogenic (inflamed) fat
- Must be distinguished from hematoma - abscess has peripheral wall vascularity; hematoma does not
6. Cellulitis
- Diffuse soft tissue inflammation of skin and subcutaneous tissues
- Skin thickening, diffuse soft tissue edema with the marbled/reticulated pattern
- Important: must exclude underlying DVT as cellulitis and DVT frequently coexist
- No discrete fluid collection (this helps differentiate from abscess)
7. Joint Effusion
- Distension of the joint capsule with fluid
- Can be simple (anechoic) or complex (internal echoes, septations) depending on the cause (inflammatory, infectious, traumatic)
- Aspiration/sampling can be guided under ultrasound
8. Muscle Injury (Strain/Tear)
- Mechanism: blunt contusion, penetrating injury, or a muscle "pull" (tear of muscle bundles from vigorous exercise)
- Sonographic evolution by time:
- Initially (<7 days): hyperechoic, homogeneous or heterogeneous
- By ~7 days: intermediate to low echogenicity, heterogeneous
- These findings persist for at least 3 weeks
- Focal abnormalities often correspond to associated hematoma and edema
- No internal vascularity
9. Tumors (Soft Tissue Masses)
Can cause leg swelling and tenderness. Solid masses in soft tissue must be distinguished from superficial veins and DVT.
Benign Tumors
- Include: lipomas, hemangiomas, fibromas, desmoid tumors, neurofibromas, leiomyomas
- Lipoma - most common; iso- or hyperechoic relative to surrounding fat; scant internal vascularity
- Often require CT or MRI for full characterization
Malignant Tumors
- Primary: sarcoma and lymphoma
- Metastatic: lymphoma, leukemia, melanoma
- Appearance: solid or complex masses
- Doppler hallmark: high velocity (>25 cm/s), low-resistance arterial flow pattern within the mass
- Any suspicious solid mass should prompt further imaging (CT/MRI) and possible biopsy
Summary Table
| Finding | Key Sonographic Feature | Vascularity on Doppler |
|---|---|---|
| Soft tissue edema | Marbled, reticulated subcutaneous fat | None |
| Hematoma | Cystic/complex mass, evolves over time | None |
| Normal lymph node | Ovoid, echogenic hilum, <1 cm | Central hilar flow |
| Lymphadenopathy | Enlarged, round, lost hilum | Disordered peripheral flow |
| Baker's cyst | Posteromedial popliteal, thin-walled, anechoic | None |
| Abscess | Complex collection, may contain gas | Peripheral wall vascularity |
| Cellulitis | Skin thickening, diffuse edema | None (diffuse) |
| Joint effusion | Distended joint capsule with fluid | None |
| Muscle tear | Hyperechoic then hypoechoic, heterogeneous | None |
| Benign tumor (lipoma) | Hyperechoic, well-defined | Scant |
| Malignant tumor | Solid/complex mass | High velocity, low resistance |
Clinical takeaway: Recognition of these findings is essential because they can be the actual cause of the patient's symptoms, or may coexist with venous pathology. Integration of the clinical history with the sonographic findings guides appropriate management and follow-up imaging.
Search for ultrasound images of Baker's cyst and other common non-vascular findings
Finding Sources
Searching the Web
Baker's cyst ultrasound image popliteal sonography
Searching the Web
hematoma lymph node soft tissue edema abscess ultrasound images non-vascular findings
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Searching the Web
inguinal lymph node ultrasound normal vs malignant sonography image
Searching the Web
soft tissue hematoma ultrasound image muscle tear edema sonography
Loading Image
Loading Image
Loading Image
Here is a visual guide to the key non-vascular findings you'll encounter on venous Doppler ultrasound:
Ultrasound Images: Non-Vascular Findings in Venous Doppler
1. Baker's (Popliteal) Cyst
Anatomy - where it forms:
Ultrasound - transverse view showing the cyst between the two muscles:

Ultrasound - measured Baker's cyst (textbook image, Tintinalli's Emergency Medicine):
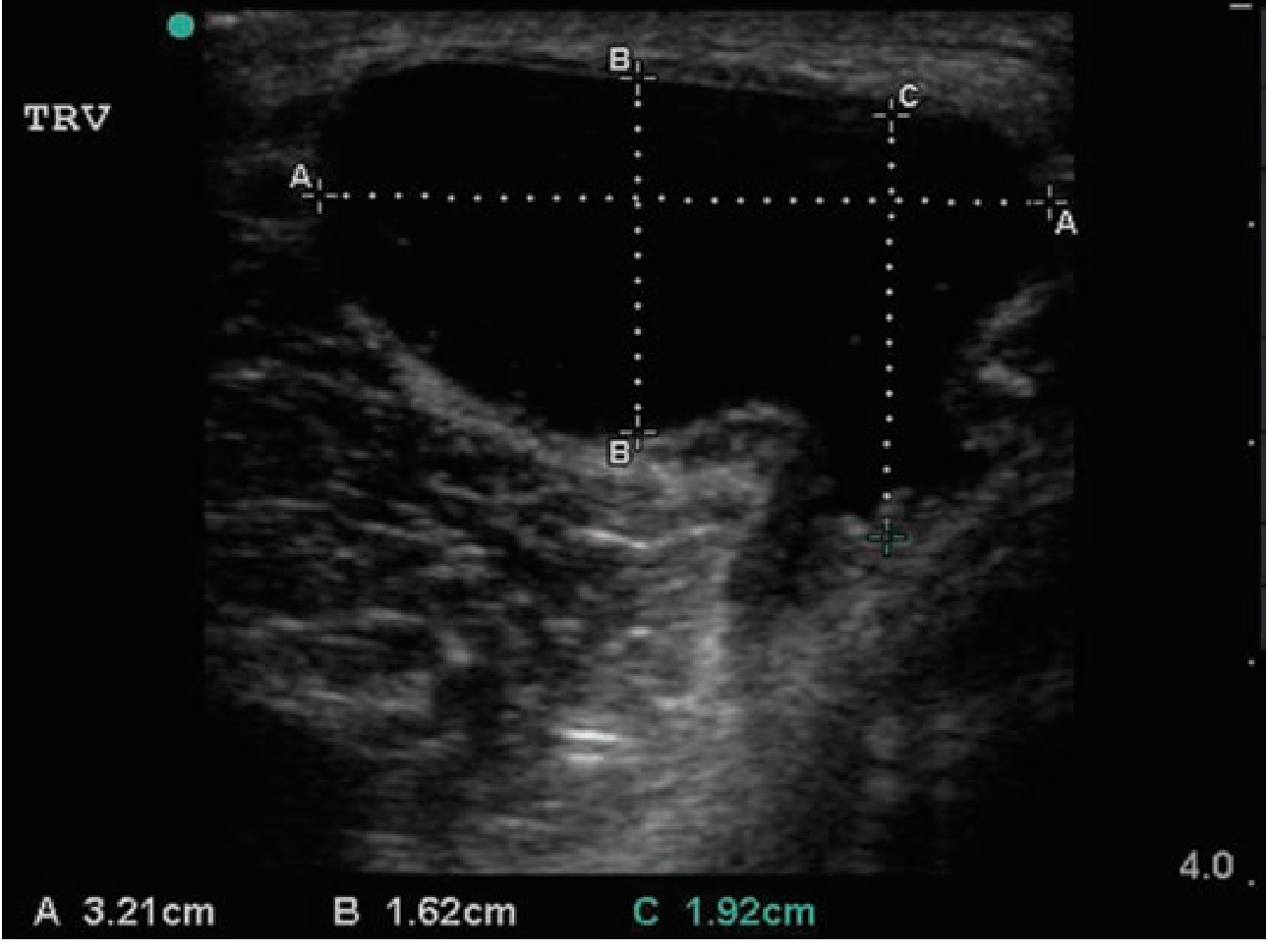
Key features to know:
- Located posteromedially in the popliteal fossa
- Anechoic (fluid-filled), thin-walled, no internal flow
- Non-compressible - differentiates it from adjacent veins which compress normally
- A neck tracking toward the knee joint is pathognomonic
- Ruptured cyst - fluid tracks inferiorly along the medial calf between gastrocnemius heads, mimicking DVT
2. Hematoma
Hematomas are avascular on color Doppler - this is the key feature distinguishing them from solid tumors.

Sonographic evolution by age:
| Stage | Appearance |
|---|---|
| Acute (hours) | Hyperechoic or isoechoic |
| Early subacute | Mixed echogenicity, heterogeneous |
| Late subacute (~1 wk) | Hypoechoic, may show fluid-fluid levels |
| Chronic | Retracted, may become hyperechoic with fibrosis |
Key point: Color Doppler shows absent internal vascularity in all stages - this differentiates hematoma from lymph nodes and tumors.
3. Lymph Nodes

Normal/Reactive node:
- Ovoid/kidney-bean shape (short axis < half the long axis)
- Hypoechoic cortex with echogenic central hilum
- Central hilar flow on Doppler (centripetal branching)
- Usually <1 cm short axis in the groin
Malignant node:
- Rounder (short axis approaches long axis)
- Loss of echogenic hilum
- Disordered, peripheral, or chaotic vascularity on Doppler
- May show central necrosis (mimics abscess, but no surrounding inflammation)
4. Soft Tissue Edema
- Subcutaneous fat takes on a marbled or reticulated appearance
- Anechoic fluid pockets interspersed between echogenic fat lobules
- No discrete mass, no vascularity
- Causes: CHF, DVT, venous obstruction, hypoalbuminemia, lymphedema
- Lymphedema is sonographically identical to venous edema - clinical context differentiates them
5. Abscess vs Cellulitis
Cellulitis: Skin and subcutaneous thickening, diffuse cobblestone/marbled echogenicity, no discrete fluid collection.
Abscess: Well-defined hypoechoic/complex collection with:
- Internal echoes and debris
- Possible gas bubbles (bright echogenic foci with posterior shadowing - highly specific)
- Peripheral wall vascularity on Doppler (unlike hematoma, which is avascular throughout)
- Surrounding echogenic, inflamed fat
6. Summary: Color Doppler Vascularity Pattern
| Finding | Internal Vascularity |
|---|---|
| Baker's cyst | None |
| Hematoma | None |
| Soft tissue edema | None |
| Normal lymph node | Central hilar flow |
| Reactive lymphadenopathy | Increased central hilar flow |
| Malignant lymph node | Peripheral/disordered flow |
| Abscess | Peripheral wall only |
| Lipoma (benign tumor) | Scant |
| Malignant tumor/sarcoma | High-velocity, low-resistance arterial flow |
The Doppler vascularity pattern is the single most useful discriminator among these findings. A mass with no internal flow is almost always benign (cyst, hematoma, edema); disordered high-velocity arterial flow inside a solid mass raises concern for malignancy.
This is a shared conversation. Sign in to Orris to start your own chat.