Prompt- Create a super aesthetic, handwritten-style revision note page for the topic: • Make it look like neat exam notes written on a page (top view, clean layout, colorful headings, underlines, boxes). • Keep it crisp, high-yield, and exam-oriented. • Use clear headings and organize content like this (modify if needed for topic): ○ Definition ○ Etiology ○ Pathogenesis (flow/arrow style) ○ Clinical features ○ Radiographic features (if applicable) ○ Histopathology (if applicable) ○ Key features ○ Differential diagnosis ○ Management ○ Complications ○ Key points / last-minute revision box • Add simple diagrams or labeled sketches wherever helpful. • Highlight important keywords. • Include one memory trick / one-line summary •
acute pancreatitis etiology pathogenesis clinical features management high yield exam notes
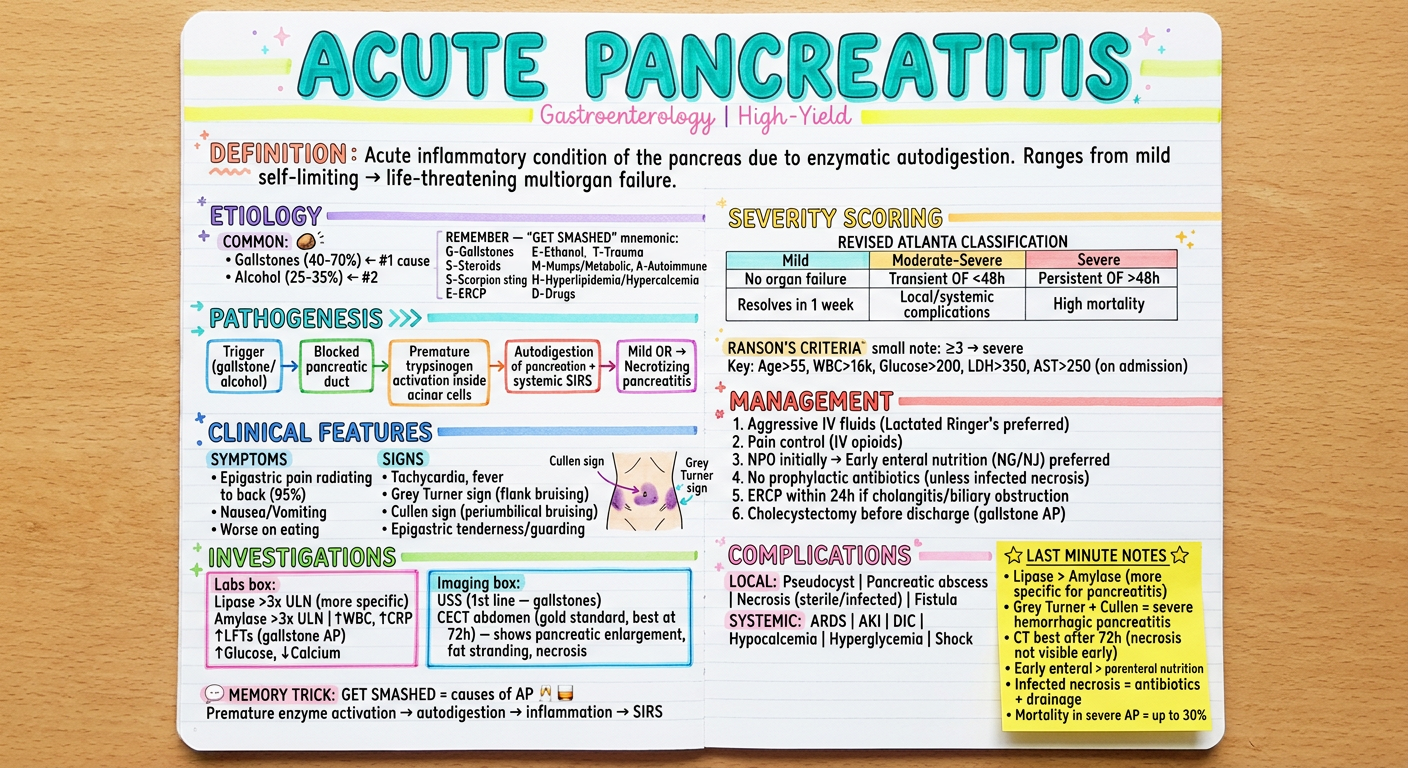
- Gallstones (#1, 40-70%) | Ethanol (#2, 25-35%) | Trauma | Steroids | Mumps/Metabolic | Autoimmune | Scorpion sting | Hypertriglyceridemia/Hypercalcemia | ERCP | Drugs
Pph management,treatment details,dosage,contraindication
postpartum hemorrhage PPH management drugs dosage oxytocin misoprostol tranexamic acid carboprost 2024 guidelines
PPH drugs dosage contraindications management steps
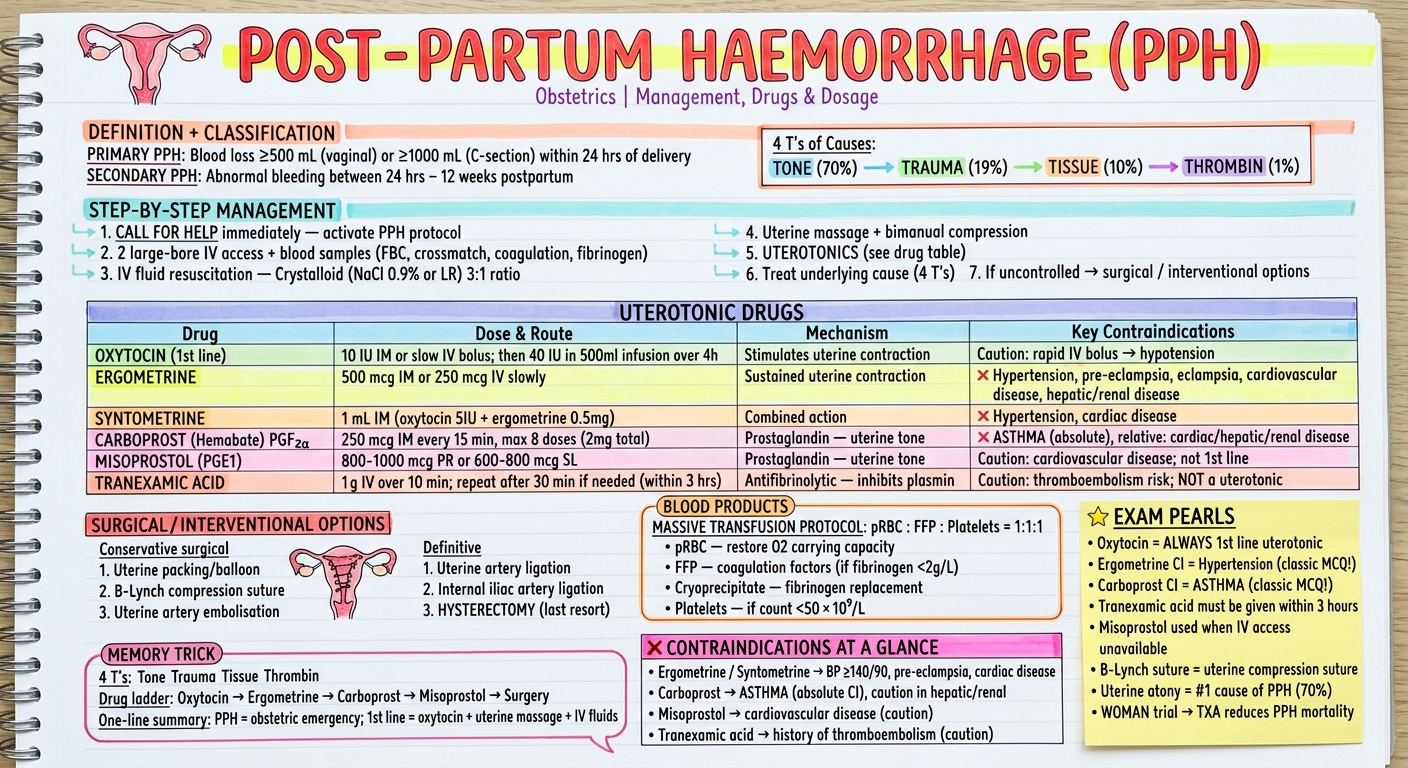
PPH - Key High-Yield Points
- Primary PPH: ≥500 mL blood loss (vaginal) / ≥1000 mL (C-section) within 24 hours
- Secondary PPH: Abnormal bleeding 24 hrs - 12 weeks postpartum
| Cause | % |
|---|---|
| Tone (uterine atony) | 70% |
| Trauma (lacerations) | 19% |
| Tissue (retained placenta) | 10% |
| Thrombin (coagulopathy) | 1% |
| Drug | Dose | Contraindications |
|---|---|---|
| Oxytocin (1st line) | 10 IU IM/slow IV; 40 IU in 500 mL infusion | Rapid IV → hypotension |
| Ergometrine | 500 mcg IM or 250 mcg IV slowly | Hypertension, pre-eclampsia, cardiac disease |
| Syntometrine | 1 mL IM | Hypertension, cardiac disease |
| Carboprost (PGF2α) | 250 mcg IM q15 min, max 8 doses (2 mg) | ASTHMA (absolute CI), hepatic/renal disease |
| Misoprostol (PGE1) | 800-1000 mcg PR or 600-800 mcg SL | Cardiovascular disease (caution) |
| Tranexamic Acid | 1g IV over 10 min; repeat after 30 min if needed (within 3 hrs) | Thromboembolism risk (caution) |
- Ergometrine ❌ = Hypertension / Pre-eclampsia
- Carboprost ❌ = Asthma (absolute contraindication)
- Tranexamic acid - give within 3 hours (WOMAN trial evidence)
Eclampsia management
eclampsia management magnesium sulfate antihypertensives dosage protocol 2024 guidelines
eclampsia magnesium sulfate dose contraindications toxicity antidote antihypertensives
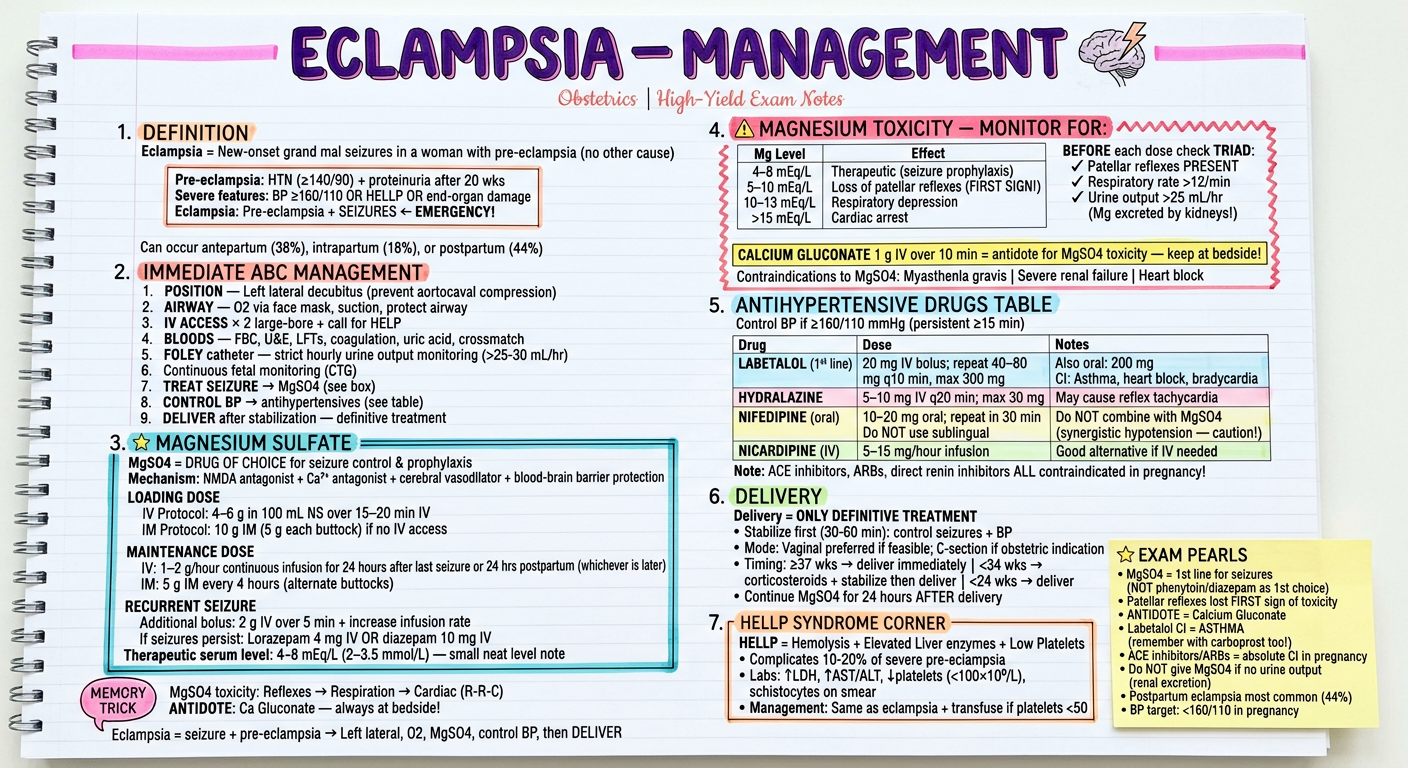
Eclampsia - Complete Management Summary
Immediate Steps (ABC + obstetric)
- Left lateral position (aortocaval decompression)
- O2 via face mask + protect airway
- 2× large-bore IV + bloods (FBC, U&E, LFTs, coag, crossmatch)
- Foley catheter - strict hourly urine output (target >25-30 mL/hr)
- Continuous CTG monitoring
- MgSO4 → seizure control
- Antihypertensives → if BP ≥160/110
- Deliver after stabilization
MgSO4 - Drug of Choice
| Protocol | Loading Dose | Maintenance |
|---|---|---|
| IV | 4–6 g in 100 mL NS over 15–20 min | 1–2 g/hr for 24 hrs after last seizure/delivery |
| IM (no IV access) | 10 g IM (5 g each buttock) | 5 g IM every 4 hrs |
| Recurrent seizure | Extra 2 g IV bolus | Increase infusion rate |
MgSO4 Toxicity - "R-R-C" Mnemonic
| Mg Level | Effect |
|---|---|
| 5–10 mEq/L | Loss of patellar reflexes (FIRST sign!) |
| 10–13 mEq/L | Respiratory depression |
| >15 mEq/L | Cardiac arrest |
- ✅ Patellar reflex present
- ✅ RR >12/min
- ✅ Urine output >25 mL/hr
Antihypertensives (target BP <160/110)
| Drug | Dose | Contraindication |
|---|---|---|
| Labetalol (1st line) | 20 mg IV → repeat 40–80 mg q10 min; max 300 mg | Asthma, heart block, bradycardia |
| Hydralazine | 5–10 mg IV q20 min; max 30 mg | Lupus, aortic dissection |
| Nifedipine (oral) | 10–20 mg oral; repeat in 30 min | Caution with MgSO4 (additive hypotension) |
| Nicardipine | 5–15 mg/hr IV infusion | - |
Key Exam MCQs
- MgSO4 = 1st line (NOT phenytoin, NOT diazepam as primary)
- Patellar reflex = first thing to disappear in toxicity
- Calcium gluconate = antidote
- Labetalol CI = Asthma
- Delivery = only definitive treatment; continue MgSO4 for 24 hrs postpartum
1p0ml NS or 13 ml NS for 4g Mgso4
4 g ÷ 0.5 g/mL = 8 mL of 50% MgSO4
How much diluent (NS)?
- 100 mL NS is correct for IV administration
- Neither "10 mL NS" nor "13 mL NS" is a standard dilution for the loading dose
Where does the confusion come from?
| Preparation | MgSO4 vol | Diluent | Total vol | Infuse over |
|---|---|---|---|---|
| Standard (WHO/RCOG) | 8 mL (50%) | 92 mL NS → total 100 mL | 100 mL | 15–20 min |
| Concentrated (some protocols) | 8 mL (50%) | 12 mL NS → total 20 mL | 20 mL | 10–15 min slow push |
| Pritchard IM protocol | 10 g IM (5 g each buttock) | No diluent | — | — |
Bottom line
| Question | Answer |
|---|---|
| Volume of 50% MgSO4 for 4 g | 8 mL |
| Standard diluent | 92 mL NS (total 100 mL) |
| "10 mL NS" correct? | ❌ No standard protocol |
| "13 mL NS" correct? | ❌ No standard protocol |
| Correct standard dilution | 8 mL MgSO4 + 92 mL NS = 100 mL total |