Approch to glp1 analogue management in obesity
Reading File
Finding Sources
Finding Sources
Searching PubMed
"GLP-1 receptor agonist" AND obesity AND management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
I now have rich, comprehensive data from Harrison's (2025), Sabiston, and the comparative trial data. Let me compile the full, structured answer.
Approach to GLP-1 Analogue Management in Obesity
1. Background and Mechanism
GLP-1 receptor agonists (GLP-1 RAs) are incretin-mimetic agents that have become central to obesity pharmacotherapy. Their mechanism is multifactorial:
- Pancreatic effects: Stimulate glucose-dependent insulin secretion; inhibit glucagon secretion
- Gastrointestinal: Slow gastric emptying, prolonging satiety
- Central (hypothalamic): Activate GLP-1 receptors in the arcuate nucleus and nucleus tractus solitarius, suppressing appetite and reducing food intake
- Combined GIP/GLP-1 (tirzepatide): GIP receptor agonism in the brain acts synergistically with GLP-1 receptor activation to enhance weight loss
- Harrison's Principles of Internal Medicine 22E, p. 3236
2. Approved Agents for Obesity (Indications)
| Drug | Dose/Route | Approval for Obesity | Key Trial |
|---|---|---|---|
| Liraglutide (Saxenda) | 3.0 mg SC once daily | Adults (2014); Adolescents ≥12 yrs (2020) | SCALE program |
| Semaglutide (Wegovy) | 2.4 mg SC once weekly | Adults (2021); Adolescents (2022) | STEP program |
| Tirzepatide (Zepbound) | 5/10/15 mg SC once weekly | Adults (2023) | SURMOUNT program |
As of May 2024, 13 GLP-1 RAs are FDA approved; only liraglutide, semaglutide, and tirzepatide are specifically approved for obesity.
- Sabiston Textbook of Surgery, p. 3543; Harrison's, p. 3236-3237
3. Patient Selection - Who to Start
Standard indications (pharmacotherapy for obesity):
- BMI ≥ 30 kg/m² (obesity), OR
- BMI ≥ 27 kg/m² with at least one weight-related comorbidity (T2DM, hypertension, dyslipidemia, OSA, CVD)
- Failed lifestyle intervention (diet + exercise counseling)
Preferred when comorbidities present:
- T2DM - any GLP-1 RA (dual benefit)
- Established CVD - semaglutide 2.4 mg preferred (SELECT trial: 20% reduction in MACE)
- Heart failure with preserved EF - semaglutide (STEP-HFpEF trial benefit)
- Pre-bariatric surgery bridging - use to reduce operative risk in very high BMI
- Post-bariatric weight regain - semaglutide especially effective (~10% additional loss)
- Harrison's, p. 3236-3237; Sabiston, p. 3547
4. Dose Titration Protocol
Slow dose escalation is essential to minimize GI side effects:
Liraglutide
- Start: 0.6 mg SC once daily x 1 week
- Increase by 0.6 mg weekly
- Target: 3.0 mg SC daily
- Titration period: ~5 weeks
Semaglutide (Wegovy)
- Start: 0.25 mg SC once weekly x 4 weeks
- Escalate in 4-week increments: 0.5 mg → 1.0 mg → 1.7 mg → 2.4 mg
- Target: 2.4 mg SC weekly
- Full titration: ~17 weeks
Tirzepatide
- Start: 2.5 mg SC once weekly x 4 weeks
- Increase by 2.5 mg every 4 weeks
- Target: 5 mg, 10 mg, or 15 mg SC weekly (max 15 mg)
- Adjust upward based on tolerability
- Yamada's Textbook of Gastroenterology, p. 2149; Harrison's, p. 3237
5. Efficacy - Trial Data
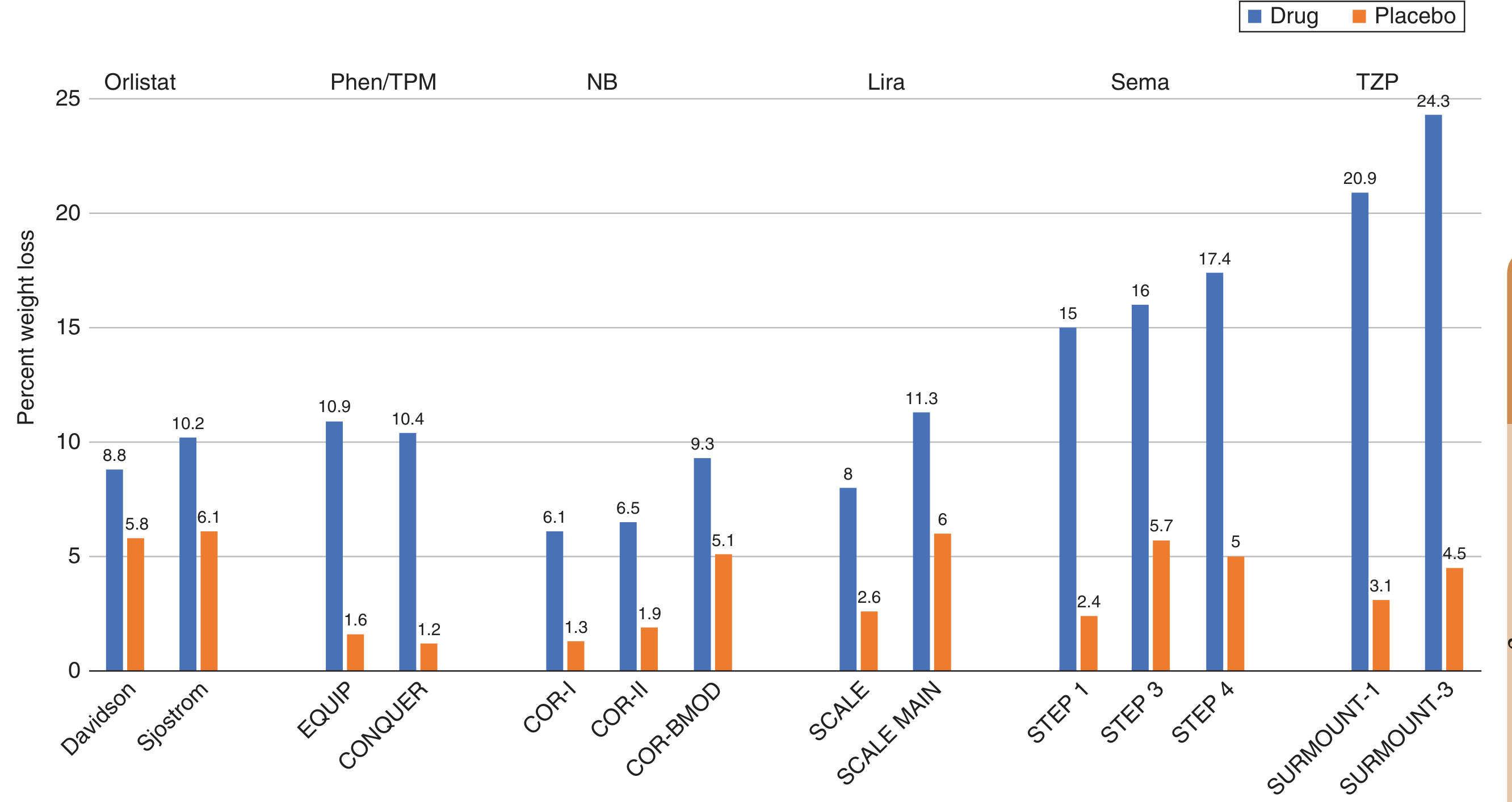
| Drug | Placebo-subtracted weight loss |
|---|---|
| Liraglutide | 3.4-6.1% (SCALE trials, 1 year) |
| Semaglutide | 6.2-14.8% (STEP 1-4, 68 wks); 12.6% at 104 wks (STEP 5) |
| Tirzepatide | 11.6-21.4% (SURMOUNT, 15 mg dose) |
Key meta-analysis (Sabiston): Pooled STEP + SURMOUNT data: placebo-subtracted body weight reduction of -12.9% with semaglutide, -19.2% with tirzepatide.
Important caveat: After stopping medication, approximately two-thirds of prior weight loss is regained within 1 year - these are likely chronic, long-term therapies.
- Harrison's, p. 3236-3237; Sabiston, p. 3545
6. Contraindications
Absolute:
- Personal or family history of medullary thyroid carcinoma (MTC)
- Multiple Endocrine Neoplasia type 2 (MEN2)
- Pregnancy (teratogenic risk; discontinue before conception attempt)
- Known hypersensitivity to the agent
Relative/precautions:
- History of pancreatitis (use with caution)
- Severe gastroparesis (GI slowing may worsen)
- Renal impairment (monitor for dehydration from GI side effects)
- Pre-operative context: increased aspiration risk - typically held for 1 week (liraglutide daily) or 2-4 weeks (semaglutide/tirzepatide weekly) before elective surgery per perioperative guidelines
- Harrison's, p. 3236-3237; Miller's Anesthesia, p. 1179-1184
7. Adverse Effects and Monitoring
Most common (class effect):
- Nausea, vomiting, diarrhea, constipation (generally mild and transient; peak during dose escalation)
- Injection site reactions
Serious but rare:
- Acute pancreatitis (monitor for abdominal pain; discontinue if suspected)
- Gallbladder disease / cholelithiasis (rapid weight loss increases risk)
- Tachycardia (mild, usually transient)
- Eustachian tube dysfunction (emerging adverse event signal from recent systematic review, PMID 39666743)
Monitoring parameters:
- Weight / BMI at each visit
- Blood glucose (hypoglycemia risk when combined with insulin/sulfonylurea)
- HbA1c if diabetic
- Renal function if GI side effects significant (dehydration)
- Thyroid (clinical vigilance; routine calcitonin not universally recommended)
8. Assessing Response and Adjusting Therapy
A standard benchmark:
- If < 5% weight loss after 12-16 weeks at the target dose → consider switching agent or augmenting with lifestyle/behavioural therapy
- If ≥ 5% weight loss → continue; reassess comorbidity improvement
- Reassess at 16 weeks; if inadequate response, consider:
- Escalating to higher dose tier (e.g., tirzepatide 10 → 15 mg)
- Adding complementary medication (e.g., phentermine/topiramate or naltrexone/bupropion if not already on)
- Referral for bariatric surgery evaluation (if BMI criteria met)
9. Special Populations
| Population | Consideration |
|---|---|
| Adolescents (≥12 yrs) | Liraglutide and semaglutide approved; tirzepatide not yet |
| T2DM | All three agents confer dual metabolic benefit |
| Established CVD | Semaglutide preferred (SELECT trial: 20% MACE reduction) |
| HFpEF | Semaglutide (STEP-HFpEF trial) |
| Post-bariatric surgery | GLP-1 RAs useful for inadequate loss/regain; semaglutide superior to liraglutide |
| Pre-surgical (bariatric) | Use as bridge to lower BMI and reduce operative risk |
| Pre-general surgery | Hold 1-2 weeks (daily agents) or 2-4 weeks (weekly agents) before procedure |
10. Treatment Algorithm Summary
Obesity (BMI ≥30 or ≥27 + comorbidity)
↓
Lifestyle intervention (diet + exercise + behavioural therapy)
↓ Insufficient response
Pharmacotherapy: GLP-1 RA (first choice in most patients)
↓
Choose agent based on comorbidities:
- CVD/HFpEF → Semaglutide 2.4 mg weekly
- T2DM → Any GLP-1 RA; tirzepatide dual benefit
- General obesity → Tirzepatide (greatest efficacy) or semaglutide
↓
Titrate slowly to target dose (4-17 weeks per agent)
↓
Assess response at 12-16 weeks at target dose
≥5% loss → Continue, monitor
<5% loss → Reassess adherence, switch/add agent, or refer for bariatric surgery
↓
Long-term continuation (weight regains if stopped)
Recent Evidence Update
A 2025 Cochrane meta-analysis on tirzepatide for obesity (PMID: 41161687) and a 2024 systematic review/meta-analysis on tirzepatide efficacy including SURMOUNT-2 (PMID: 38850440) confirm its superiority in body weight reduction versus placebo, with the largest effects seen at the 15 mg dose. GLP-1 RAs as adjunct to bariatric surgery also show promise (PMID: 41071360 - Langenbecks Arch Surg, 2025).
Sources: Harrison's Principles of Internal Medicine 22E (2025), pp. 3236-3238 | Sabiston Textbook of Surgery, pp. 3541-3549 | Yamada's Textbook of Gastroenterology 7e | Miller's Anesthesia 10e | PubMed: PMID 38850440, 41161687, 41071360
This is a shared conversation. Sign in to Orris to start your own chat.