Increase in wbc in a diabwtic patient reason for it diagnosis ,investigation of choice and treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Searching PubMed
leukocytosis diabetes mellitus infection
Here is a comprehensive, structured answer based on authoritative textbook sources.
Leukocytosis (Raised WBC) in a Diabetic Patient
Why WBC Rises in a Diabetic Patient - Causes
Diabetes creates a unique environment that predisposes to both infectious and non-infectious causes of leukocytosis. The key categories are:
A. NON-INFECTIOUS (Metabolic/Stress)
| Cause | Mechanism |
|---|---|
| Diabetic Ketoacidosis (DKA) | A non-infectious inflammatory state - DKA itself causes leukocytosis via cortisol/catecholamine-driven demargination and cytokine release, even without infection |
| Hyperosmolar Hyperglycaemic State (HHS) | Same demargination mechanism |
| Physiological stress/dehydration | Stress hormones (corticosteroids, inotropes) demarginate neutrophils from vessel walls, raising circulating WBC |
Goldman-Cecil Medicine notes: "Many cases are due to noninfectious causes, including inflammatory conditions (renal insufficiency, diabetic ketoacidosis, lupus erythematosus), and demargination stress reactions (dehydration, systemic corticosteroids)." Check for toxic granulations, Dohle bodies, and a band-cell shift on the peripheral smear to differentiate.
Important: In DKA, a WBC of up to ~25,000/mm³ can occur purely due to stress/ketosis. A WBC >25,000 or the presence of toxic granulations should raise suspicion for a co-existing infection.
B. INFECTIOUS CAUSES (Most Common & Clinically Important)
Diabetes impairs neutrophil chemotaxis, phagocytosis, and intracellular killing - making diabetics uniquely vulnerable to a range of infections.
1. Diabetic Foot Infection / Osteomyelitis
- Most common cause in a diabetic with leukocytosis
- Microangiopathy + neuropathy (motor, sensory, autonomic) leads to ulcers, soft-tissue infection, and bone invasion
- Organisms: polymicrobial - S. aureus most common, followed by S. epidermidis; moderate/severe infections also involve gram-negatives, anaerobes, MRSA
- WBC >12,000/mm³ with >10% bands = part of the SIRS/IWGDF severity classification (Grade 4/Severe)
2. Urinary Tract Infections (UTI) - Including Emphysematous Pyelonephritis
- Diabetes is a risk factor for complicated UTIs
- Emphysematous pyelonephritis (gas-forming, necrotizing renal infection) - almost exclusively in diabetics - is a urologic emergency presenting with sepsis and leukocytosis
- Other diabetes-specific UTI syndromes: renal/perinephric abscess, papillary necrosis, xanthogranulomatous pyelonephritis
3. Cellulitis / Skin & Soft Tissue Infections
- Manifests as erythema, warmth, edema, tenderness + fever + leukocytosis
- Diabetics have impaired skin barrier and immune response
4. Necrotizing Soft Tissue Infections (NSTI) / Necrotizing Fasciitis
- Rapidly spreading infection along fascial planes
- Diabetes is a major risk factor
- Presents with disproportionate pain, crepitus, systemic sepsis, and marked leukocytosis
- This is a surgical emergency
5. Rhinocerebral Mucormycosis
- Seen in ~70% of cases in diabetic patients (especially poorly controlled/DKA)
- Presents with facial pain, nasal discharge (black eschar), proptosis, headache - cranial nerve palsies
- Leukocytosis reflects the invasive fungal infection
6. Other Infections
- Liver abscess (diabetes + biliary disease)
- Deep neck space infections
- Pneumonia
Approach to Diagnosis
Step 1 - Clinical Assessment
- History: fever, localizing symptoms (foot ulcer, dysuria, facial pain, skin changes)
- Examination: vital signs for SIRS (temp >38 or <36°C, HR >90, RR >20, WBC >12,000)
- Peripheral blood smear: look for toxic granulations, Dohle bodies, band cells (left shift confirms infection, not just stress demargination)
Step 2 - Investigations by Suspected Site
| Investigation | What it Detects |
|---|---|
| CBC with differential | Degree of leukocytosis, left shift, eosinophilia |
| Peripheral blood smear | Toxic granulations, Dohle bodies, band cells |
| Blood cultures (x2) | Bacteraemia/sepsis |
| Urine R/M/E + culture | UTI, emphysematous pyelonephritis |
| HbA1c + blood glucose | Glycaemic control |
| Serum ketones / ABG | DKA/HHS |
| CRP / ESR / Procalcitonin | Differentiates infectious from non-infectious causes |
| X-ray of foot | Osteolysis, periosteal reaction, bone destruction (sensitivity 60%, specificity 80%) - changes appear 10-20 days after onset |
| MRI foot (investigation of choice for diabetic osteomyelitis) | Bone marrow edema, abscess, soft tissue tracking - >95% sensitive/specific |
| CT abdomen/pelvis | Emphysematous pyelonephritis, perinephric abscess, liver abscess |
| MRI brain + paranasal sinuses | Rhinocerebral mucormycosis (orbital/sinus invasion) |
| Bone biopsy | Gold standard for osteomyelitis (identifies organism and confirms diagnosis) |
| Probe-to-bone test | If a blunt sterile probe reaches bone through an ulcer = near-100% diagnostic of underlying osteomyelitis |
Investigation of Choice
- Diabetic foot osteomyelitis: MRI foot - recommended by the American College of Radiology (appropriateness criteria score 9/9); detects changes earlier than X-ray
- Emphysematous pyelonephritis: CT abdomen (gas within renal parenchyma)
- Rhinocerebral mucormycosis: MRI brain + sinuses
- Sepsis source unknown: Blood cultures + procalcitonin

Treatment
1. Glycaemic Control (Always First)
- Optimise blood glucose - hyperglycaemia impairs neutrophil function and wound healing
- Insulin is the agent of choice in inpatient/acute settings
2. Diabetic Foot Infection - Antibiotic Therapy (IWGDF/IDSA 2023 Guidelines)
| Severity | Route | Coverage | Agents | Duration |
|---|---|---|---|---|
| Mild (Grade 2) | Oral | GPC (S. aureus, Streptococcus) | Cephalexin, oxacillin; clindamycin, TMP-SMX, doxycycline; amox-clav | 1-2 weeks |
| Moderate/Severe (Grade 3-4) | IV then oral | GPC + GNR + Pseudomonas + anaerobes + MRSA | Pip-tazo, carbapenem; vancomycin/linezolid/daptomycin for MRSA; fluoroquinolone/aminoglycoside for resistant GNR | 2-4 weeks |
| Osteomyelitis (no surgery) | IV/oral | Broad | As above | 6 weeks |
| Osteomyelitis (bone resected) | IV/oral | Culture-directed | - | 2-5 days post-resection |
3. Surgical Management
- Diabetic foot: Debridement, drainage of abscess; amputation for severe/non-salvageable limb
- Necrotizing fasciitis: Emergency surgical debridement (surgery + antibiotics - no role for antibiotics alone)
- Emphysematous pyelonephritis: Fluid resuscitation + glucose control + antibiotics + percutaneous nephrostomy or nephrectomy
4. Rhinocerebral Mucormycosis
- Reverse predisposing factor (control DKA, stop steroids)
- Liposomal Amphotericin B - antifungal of choice
- Aggressive surgical debridement of necrotic tissue
- Often fatal if treatment is delayed
5. If Non-Infectious (DKA/HHS)
- Treat the underlying DKA/HHS (IV fluids, insulin, electrolyte correction)
- Leukocytosis resolves as metabolic state corrects
- Empirical antibiotics are not routinely indicated unless infection cannot be excluded clinically
Summary Table
| Cause | Key Clue | Investigation of Choice | Treatment |
|---|---|---|---|
| DKA/HHS | Hyperglycaemia, ketones, no focus | ABG, serum ketones | IV fluids, insulin, electrolytes |
| Diabetic foot infection | Foot ulcer, erythema, probe-to-bone | MRI foot | Antibiotics ± debridement |
| Osteomyelitis | Bone exposure, X-ray changes | MRI foot / bone biopsy | 6 weeks antibiotics ± surgery |
| Emphysematous pyelonephritis | Sepsis + diabetes + flank pain | CT abdomen | Emergency drainage + antibiotics |
| Necrotizing fasciitis | Severe pain out of proportion, crepitus | CT soft tissue / clinical | Emergency surgical debridement |
| Rhinocerebral mucormycosis | Black nasal eschar, facial pain, DKA | MRI sinuses/brain | Amphotericin B + surgery |
| Cellulitis | Erythema, warmth, edema | Clinical | Antibiotics (cover GPC) |
Sources: Goldman-Cecil Medicine (26e), Sabiston Textbook of Surgery (Diabetic Foot Infections - IWGDF/IDSA 2023), Grainger & Allison's Diagnostic Radiology, Tintinalli's Emergency Medicine, Campbell-Walsh-Wein Urology, Robbins Pathologic Basis of Disease.
What does wbc do in the body
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete, textbook-grounded answer on what WBCs do in the body.
Functions of White Blood Cells (Leukocytes)
White blood cells are the mobile units of the body's protective system. Normal count is 4,000-11,000 cells/µL of blood. They are formed in the bone marrow (granulocytes, monocytes) and lymphoid tissue (lymphocytes), then transported wherever they are needed.
"The real value of WBCs is that most of them are specifically transported to areas of serious infection and inflammation, thereby providing a rapid and potent defense against infectious agents." - Guyton & Hall Medical Physiology
The 5 Types and Their Specific Functions
1. Neutrophils (50-70% of all WBCs)
The first responders to infection. They are the most numerous WBC and the primary defence against bacteria and fungi.
What they do:
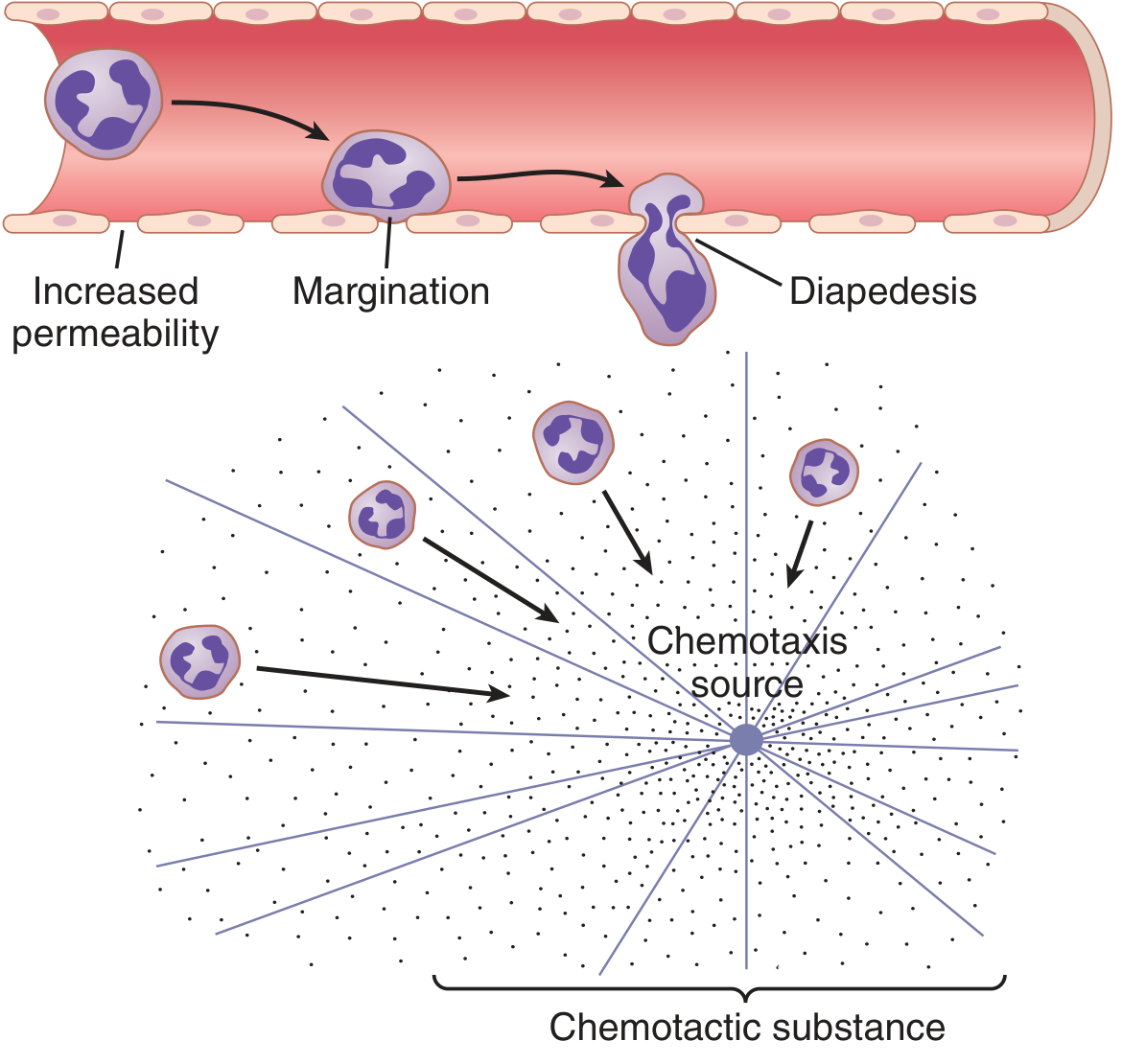
- Chemotaxis - they detect chemical signals (bacterial toxins, complement fragments, clotting products) released at sites of infection and migrate toward them, guided by a concentration gradient, up to 100 µm away from the source
- Diapedesis - they squeeze through gaps between capillary endothelial cells to reach infected tissues
- Phagocytosis - they engulf bacteria by extending pseudopodia around them, forming a phagosome; lysosomes then fuse with the phagosome to form a phagolysosome, releasing digestive enzymes (lysozyme, lactoferrin, myeloperoxidase) that kill the organism
- Each neutrophil can phagocytize 3-20 bacteria before it dies
- Their granules contain antimicrobial peptides and enzymes ready for immediate killing
Life span: 4-8 hours in blood + 4-5 days in tissues (shorter during active infection)
2. Monocytes → Macrophages (2-8% of WBCs)
The heavy-duty phagocytes and antigen presenters.
- In the blood they are immature (monocytes) with limited killing ability
- Once they enter tissues, they swell up to 5x in diameter (60-80 µm) and become macrophages - extremely potent defenders
- Macrophages can phagocytize particles up to 100x larger than neutrophils can handle, including whole red blood cells, parasites, and even dead neutrophils
- They also present antigens to T lymphocytes, linking innate and adaptive immunity
- Tissue macrophages can live for months
- They release cytokines (TNF, IL-1, IL-6) that orchestrate the inflammatory response
3. Lymphocytes (20-40% of WBCs)
The brains of the immune system - responsible for specific, memory-based immunity.
There are three main subtypes:
| Type | Function |
|---|---|
| T cells (CD4+ helper) | Help B cells make antibodies; coordinate the immune response |
| T cells (CD8+ cytotoxic) | Directly kill virus-infected cells and tumour cells |
| B cells / Plasma cells | Produce antibodies (immunoglobulins) that tag pathogens for destruction (opsonisation) |
| NK (Natural Killer) cells | Kill virus-infected cells and cancer cells without prior sensitisation |
- Lymphocytes continuously recirculate - from blood → tissues → lymph → back to blood
- They form immunological memory (reason vaccines work)
- Life span: weeks to months (memory cells can last years)
4. Eosinophils (1-4% of WBCs)
Specialists against parasites and allergic reactions.
- Their specific granules contain cytotoxic proteins that are toxic to helminths (worms) and protozoa
- They play a key role in allergic reactions and chronic inflammation
- Elevated in: asthma, hay fever, drug reactions, parasitic infections (mnemonic: NAACP - Neoplasm, Allergy, Asthma, Collagen vascular disease, Parasites)
5. Basophils (<0.5% of WBCs)
Mediators of allergic and inflammatory responses.
- Their large granules contain: histamine, heparin, heparan sulfate, leukotrienes
- Release of these substances causes the classic signs of allergy: vasodilation, increased capillary permeability, bronchospasm
- Functionally similar to mast cells (their tissue counterparts)
- Heparin they release prevents blood from clotting in inflamed areas, allowing better immune cell circulation
How WBCs Work Together - A Summary
INFECTION / FOREIGN SUBSTANCE DETECTED
↓
Neutrophils → arrive first (minutes to hours) → phagocytose bacteria
↓
Monocytes → arrive later → become macrophages → powerful phagocytosis
↓
Macrophages → present antigens to T lymphocytes
↓
T cells (helper) → activate B cells
↓
B cells → produce antibodies → opsonise pathogens
↓
Opsonised pathogens → phagocytosed more efficiently (opsonisation)
↓
Memory cells formed → faster response on next exposure
Opsonisation is particularly important: antibodies coat bacteria, making them stick to phagocyte receptors (via C3 complement), dramatically increasing phagocytic efficiency.
Normal WBC Reference Values
| Cell Type | Normal Count/µL | % of Total |
|---|---|---|
| Total WBC | 4,000 - 11,000 | - |
| Neutrophils | 3,000 - 6,000 | 50-70% |
| Lymphocytes | 1,500 - 4,000 | 20-40% |
| Monocytes | 300 - 600 | 2-8% |
| Eosinophils | 150 - 300 | 1-4% |
| Basophils | 0 - 100 | <0.5% |
In Short
| Cell | Primary Role |
|---|---|
| Neutrophil | First-line: bacteria and fungi (phagocytosis) |
| Macrophage | Powerful phagocytosis + antigen presentation |
| T lymphocyte | Cell-mediated immunity (kill infected/tumour cells) |
| B lymphocyte | Antibody production (humoral immunity) |
| NK cell | Kill virus-infected and cancer cells |
| Eosinophil | Parasites + allergic inflammation |
| Basophil | Allergic reactions (histamine, heparin release) |
Sources: Guyton & Hall Textbook of Medical Physiology (14e); Ganong's Review of Medical Physiology (26e); Histology: A Text and Atlas (Pawlina); Robbins & Kumar Pathologic Basis of Disease.
This is a shared conversation. Sign in to Orris to start your own chat.