Neoplasia
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed. Here is a comprehensive, exam-focused overview of Neoplasia.
Neoplasia - Complete Overview for Exam Preparation
Source: Robbins & Kumar Basic Pathology
1. Definition & Basic Concepts
Neoplasia means "new growth." A neoplasm is an abnormal mass of tissue in which growth is excessive and uncoordinated with that of normal tissues, and persists after the stimuli that evoked it have been removed.
All cancers share these fundamental features:
- Cancer is a genetic disorder caused by DNA mutations (acquired somatic, or inherited germline)
- Genetic alterations are heritable (passed to daughter cells) - subject to Darwinian selection
- Individual tumors are clonal (progeny of a single cell)
- Tumor progression = continued clonal evolution with accumulating mutations that favor more aggressive subclones
2. Nomenclature
Benign Tumors
Named by adding -oma to the cell/tissue of origin:
| Origin | Benign Tumor |
|---|---|
| Fibrous tissue | Fibroma |
| Cartilage | Chondroma |
| Glandular epithelium | Adenoma |
| Blood vessels | Hemangioma |
| Smooth muscle | Leiomyoma |
| Fat | Lipoma |
| Bone | Osteoma |
Malignant Tumors
- Carcinoma = malignancy of epithelial origin
- Adenocarcinoma = glandular pattern
- Squamous cell carcinoma = squamous differentiation
- Sarcoma = malignancy of mesenchymal origin
- Osteosarcoma, liposarcoma, leiomyosarcoma, etc.
Special Exceptions (exam favorites)
| Name | Origin/Notes |
|---|---|
| Melanoma | Malignant (despite -oma suffix) |
| Lymphoma | Malignant lymphoid tumor |
| Hepatoma | Actually malignant (hepatocellular carcinoma) |
| Seminoma | Malignant germ cell tumor of testis |
| Teratoma | Contains tissues from >1 germ layer; can be benign or malignant |
| Hamartoma | Disorganized but mature tissue components (not truly neoplastic) |
| Choristoma | Normal tissue in abnormal location (ectopic tissue) |
3. Characteristics: Benign vs. Malignant
| Feature | Benign | Malignant |
|---|---|---|
| Differentiation | Well differentiated | Variable; may be anaplastic |
| Rate of growth | Slow | Rapid |
| Mitoses | Rare; normal | Frequent; abnormal mitoses |
| Local invasion | Non-invasive; capsule often present | Invasive; no capsule |
| Metastasis | Never | Hallmark of malignancy |
| Recurrence | Rare | Common |
| Necrosis | Rare | Common |
| Nuclear features | Normal | Pleomorphism, hyperchromasia |
Differentiation & Anaplasia
Anaplasia = lack of differentiation; hallmark of malignancy. Features include:
- Pleomorphism - variation in cell and nuclear size/shape
- Hyperchromatic nuclei - dark-staining nuclei
- Abnormal mitoses - tripolar/quadripolar spindles
- Tumor giant cells - single large cells or cells with multiple nuclei
- Loss of polarity - disordered growth pattern
Dysplasia = disordered proliferation (NOT synonymous with cancer):
- Loss of uniformity, architectural disorganization
- May regress if stimulus removed
- Carcinoma in situ = dysplasia involving full thickness of epithelium (preinvasive)
4. Metastasis
The single most important feature distinguishing malignant from benign tumors. Metastasis = spread to distant, non-contiguous sites.
Routes of Spread
| Route | Details | Common Cancers |
|---|---|---|
| Lymphatic | Most common for carcinomas | Breast, lung, colon |
| Hematogenous | Most common for sarcomas; via veins | Osteosarcoma, renal cell carcinoma |
| Seeding of body cavities | Transcoelomic spread | Ovarian, GI carcinomas |
Steps of Metastatic Cascade
- Local invasion of ECM (requires detachment, MMP activity, EMT)
- Intravasation into blood/lymph
- Survival in circulation
- Arrest at distant site
- Extravasation
- Formation of micrometastases
- Growth into macrometastases (requires angiogenesis)
Common Metastatic Destinations
- Liver, lung, bone, brain, adrenal glands are the most common sites
- Bone metastases: osteolytic (kidney, thyroid, lung) vs. osteoblastic (prostate, breast)
5. Carcinogenesis: A Multistep Process
Cancer results from accumulation of multiple genetic "hits" over time. Typically divided into:
- Initiation - irreversible DNA mutation from a carcinogen
- Promotion - clonal expansion of initiated cells (reversible)
- Progression - additional mutations → invasive/metastatic cancer
Types of Carcinogens
- Chemical carcinogens: direct-acting (e.g., alkylating agents) vs. indirect-acting/procarcinogens requiring metabolic activation (e.g., PAHs in cigarette smoke)
- Radiation: UV (pyrimidine dimers → skin cancer), ionizing radiation (leukemia, thyroid, breast)
- Viral/Microbial: HPV (cervical, oropharyngeal), HBV/HCV (hepatocellular), EBV (Burkitt lymphoma, nasopharyngeal), HTLV-1 (adult T-cell leukemia), H. pylori (gastric carcinoma/MALT lymphoma)
6. Cancer Genes
Oncogenes
- Derived from proto-oncogenes (normal growth-promoting genes)
- Mutation → gain-of-function → dominant (one mutated allele sufficient)
- Mechanisms of activation: point mutation, gene amplification, chromosomal translocation
| Oncogene | Mechanism | Associated Cancer |
|---|---|---|
| RAS | Point mutation (most commonly KRAS) | Pancreatic, colon, lung (~30% of all human cancers) |
| MYC | Amplification; t(8;14) translocation | Burkitt lymphoma, breast, lung |
| HER2/NEU (ERBB2) | Amplification | Breast cancer |
| BCR-ABL | t(9;22) Philadelphia chromosome | CML |
| RET | Point mutation/translocation | MEN2, thyroid cancer |
| EGFR | Mutation/amplification | Lung, GBM |
| PDGFR | Translocation | GIST |
| CDK4 | Amplification | Glioblastoma, sarcomas |
Tumor Suppressor Genes (TSGs)
- Normal function: inhibit proliferation, promote apoptosis
- Loss of function → recessive (both alleles must be inactivated - "two-hit hypothesis" of Knudson)
- Exception: dominant-negative mutations and haploinsufficiency
| Gene | Function | Associated Cancer |
|---|---|---|
| RB | G1/S checkpoint; regulates E2F | Retinoblastoma, osteosarcoma, bladder, breast, lung |
| TP53 | "Guardian of the genome"; G1 arrest, apoptosis, DNA repair | ~50% of all human cancers; Li-Fraumeni syndrome |
| APC | Degrades β-catenin (Wnt pathway) | Colorectal cancer (FAP) |
| CDKN2A (p16) | CDK inhibitor; inhibits cyclin D-CDK4/6 | Melanoma, pancreatic, lung |
| BRCA1/2 | DNA repair (homologous recombination) | Breast, ovarian |
| VHL | Regulates HIF-1α; controls angiogenesis | Renal cell carcinoma |
| WT1 | Transcription factor | Wilms tumor |
| NF1/NF2 | RAS-GAP (NF1); Merlin (NF2) | Neurofibromatosis |
| SMAD2/4 | TGF-β signaling | Pancreatic, colon |
| PTEN | PI3K pathway suppressor | Glioblastoma, endometrial, prostate |
7. The Hallmarks of Cancer
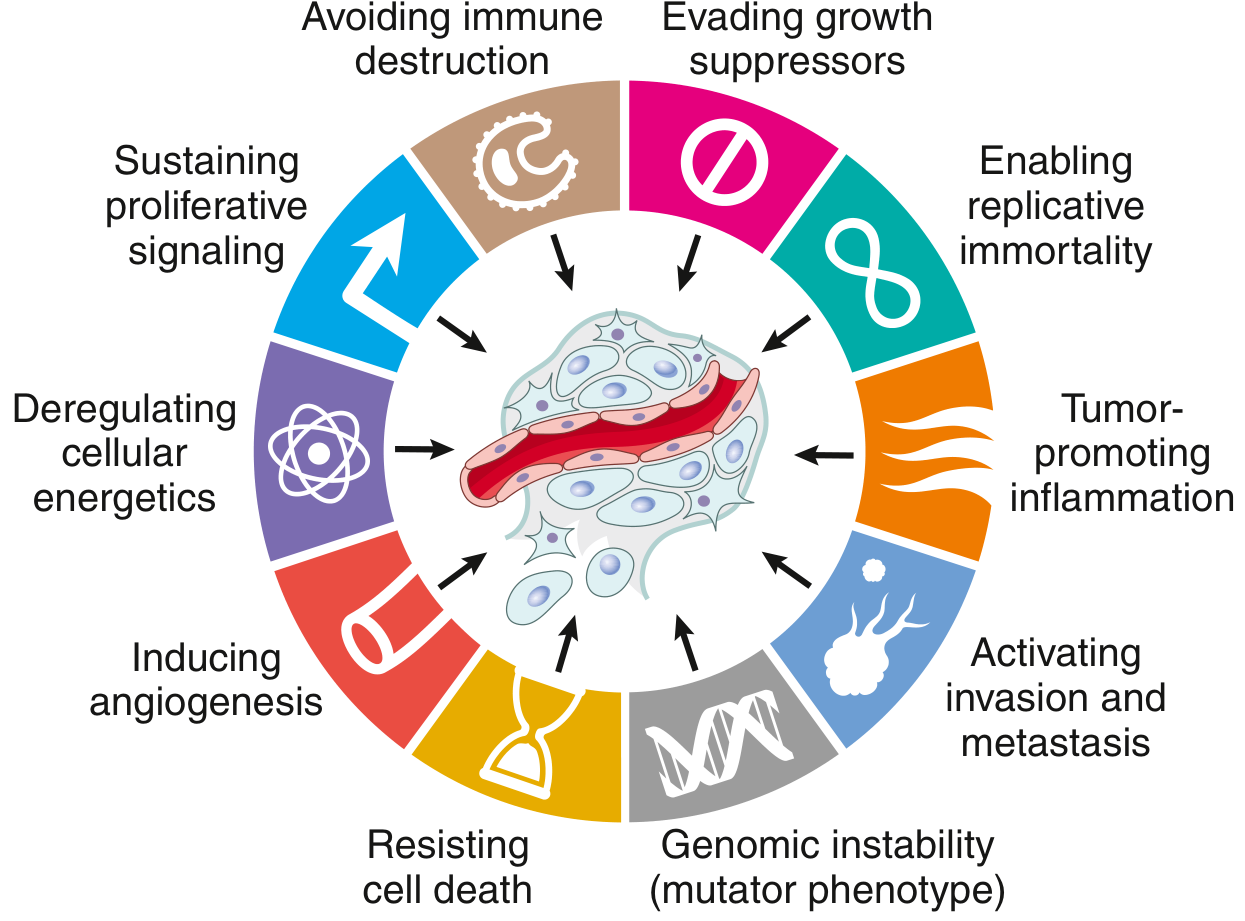
Fig. 6.15 - Eight cancer hallmarks and two enabling factors (Robbins & Kumar Basic Pathology)
The 8 Hallmarks + 2 Enabling Characteristics
| # | Hallmark | Key Molecular Mechanism |
|---|---|---|
| 1 | Self-sufficiency in growth signals | Oncogene activation (RAS, MYC, growth factor receptors) |
| 2 | Insensitivity to growth-inhibitory signals | Loss of TSGs (RB, TP53, APC) |
| 3 | Altered cellular metabolism (Warburg effect) | Aerobic glycolysis even in O2 presence; supports biosynthesis |
| 4 | Evasion of apoptosis | BCL-2 overexpression; TP53 loss; survival pathway activation |
| 5 | Limitless replicative potential (immortality) | Telomerase reactivation (hTERT) |
| 6 | Sustained angiogenesis | VEGF upregulation; HIF-1α activation |
| 7 | Invasion and metastasis | E-cadherin loss, MMP activation, EMT |
| 8 | Evasion of immune surveillance | PD-L1 upregulation, loss of MHC-I, T-reg recruitment |
| E1 | Genomic instability (enabling) | Mismatch repair defects, microsatellite instability |
| E2 | Tumor-promoting inflammation (enabling) | Chronic inflammation → ROS, growth factors, immunosuppression |
8. Key Molecular Pathways - Exam Details
RB Pathway (G1/S Checkpoint)
- Hypophosphorylated RB (active) binds E2F → blocks S-phase genes
- Growth factors → Cyclin D/CDK4/6 → phosphorylate RB → release E2F → cell enters S phase
- Any disruption of this pathway seen in virtually all cancers (CDK4 amplification, cyclin D overexpression, p16 loss, RB mutation)
TP53 Pathway ("Guardian of the Genome")
- DNA damage → ATM/ATR kinases → phosphorylate p53 → released from MDM2
- Activated p53 induces: CDKN1A (p21) → G1 arrest; BAX → apoptosis; GADD45 → DNA repair
- MDM2 provides feedback by binding p53 (p53 induces MDM2 transcription)
- Li-Fraumeni syndrome = germline TP53 mutation → multiple cancers in young age
- Loss of TP53 = most common mutation in human cancer (~50%)
Warburg Effect
- Tumor cells preferentially use aerobic glycolysis (glucose → lactate) even in the presence of oxygen
- Creates acidic microenvironment; provides carbon skeletons for biosynthesis
- Basis of PET scanning (tumors avidly uptake 18F-FDG)
9. Epidemiology
Cancer Incidence (USA)
| Sex | Most Common (Incidence) | Most Common (Mortality) |
|---|---|---|
| Male | Prostate | Lung |
| Female | Breast | Lung |
| Both combined | Lung = leading cause of cancer death |
Age & Cancer
- Cancer incidence increases with age (accumulation of somatic mutations)
- Most cancers in adults >55 years
- Childhood (<15): leukemia, CNS tumors, Wilms tumor, retinoblastoma, neuroblastoma
Hereditary Cancer Syndromes (Autosomal Dominant inheritance)
| Syndrome | Gene | Cancer Risk |
|---|---|---|
| Familial retinoblastoma | RB | Retinoblastoma, osteosarcoma |
| Li-Fraumeni | TP53 | Multiple carcinomas, sarcomas |
| FAP | APC | Colorectal cancer (100% risk) |
| HNPCC (Lynch) | MSH2, MLH1 | Colon, endometrial cancer |
| BRCA1/2 | BRCA1/2 | Breast, ovarian |
| MEN1 | MEN1 | Parathyroid, pituitary, pancreatic |
| MEN2A/B | RET | Medullary thyroid, pheochromocytoma |
| VHL disease | VHL | Renal cell carcinoma, hemangioblastoma |
| NF1 | NF1 | Neurofibromas, gliomas, MPNSTs |
| Xeroderma pigmentosum | Nucleotide excision repair genes | Skin cancers (UV sensitivity) |
10. Grading and Staging
Grading (histologic differentiation)
- Assesses microscopic appearance; Grade I (well-differentiated) → Grade IV (anaplastic)
- Indicates how closely the tumor resembles its tissue of origin
Staging (extent of disease)
- Assesses clinical/pathologic spread; more prognostically significant than grade
- TNM system: T = primary tumor size/invasion, N = regional lymph node involvement, M = distant metastasis
- Roman numeral staging (I-IV): based on TNM groupings
Key exam point: Staging is more important than grading for prognosis.
11. Paraneoplastic Syndromes
Symptoms not due to direct tumor mass or metastasis, but to ectopic hormone production or immune mechanisms.
| Syndrome | Tumor | Mechanism |
|---|---|---|
| Hypercalcemia (most common) | Squamous cell lung, breast, renal, myeloma | PTHrP secretion; osteolytic metastases |
| Cushing syndrome | Small cell lung carcinoma | Ectopic ACTH |
| SIADH | Small cell lung carcinoma | Ectopic ADH |
| Polycythemia | Renal cell carcinoma, hepatoma, cerebellar hemangioblastoma | Ectopic EPO |
| Hypoglycemia | Insulinoma, retroperitoneal sarcoma | IGF-II |
| Carcinoid syndrome | GI carcinoids (especially ileal) | Serotonin/bradykinin |
| Lambert-Eaton syndrome | Small cell lung carcinoma | Anti-VGCC antibodies |
| Acanthosis nigricans | GI, uterine carcinomas | Insulin-like factors |
| Trousseau sign | Pancreatic, other mucin-secreting carcinomas | Migratory thrombophlebitis |
12. Tumor Markers
Used for screening, monitoring response, detecting recurrence - NOT usually diagnostic alone.
| Marker | Associated Tumor | Clinical Use |
|---|---|---|
| PSA | Prostate carcinoma | Screening, monitoring |
| AFP | Hepatocellular carcinoma, yolk sac tumor | Monitoring |
| β-hCG | Choriocarcinoma, gestational trophoblastic disease, testicular germ cell tumors | Monitoring |
| CEA | Colorectal, pancreatic, gastric, lung | Monitoring recurrence |
| CA-125 | Ovarian carcinoma | Monitoring |
| CA 19-9 | Pancreatic carcinoma | Monitoring |
| Calcitonin | Medullary thyroid carcinoma | Screening (MEN2), monitoring |
| Chromogranin A | Neuroendocrine tumors (carcinoid) | Monitoring |
| LDH | Lymphoma, testicular tumors | Prognosis |
| S-100 | Melanoma, neural tumors | Staging |
| BRAF V600E | Melanoma, papillary thyroid carcinoma | Targeted therapy |
13. Apoptosis in Cancer
Cancer cells evade apoptosis through:
- BCL-2 overexpression → t(14;18) in follicular lymphoma (BCL-2 anti-apoptotic protein sequesters pro-apoptotic BAX/BAK)
- TP53 loss → no induction of apoptotic pathway after DNA damage
- Activation of survival signals (PI3K/AKT pathway; PTEN loss)
Quick Memory Aids
| Mnemonic | Content |
|---|---|
| "RB = Retinoblastoma/Brakes" | RB gene = cell cycle brake; loss = accelerated G1→S |
| "p53 = Police/53rd" | p53 = genome police; arrests, repairs, or kills damaged cells |
| "KRAS = cancer's RAS" | Most commonly mutated oncogene in human cancers |
| "BCL-2 = Back-door escape" | Blocks apoptosis via mitochondrial pathway |
| Warburg | Aerobic glycolysis = PET scan basis |
All content sourced from Robbins & Kumar Basic Pathology (Robbins Pathology), 10th edition. This covers the high-yield Neoplasia chapter (Chapter 6, pp. 187-229).
This is a shared conversation. Sign in to Orris to start your own chat.