30 year old male patient Pain in right lilac region and right loin and also pain in left iliac region since 1 day
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Here is a structured clinical analysis for this presentation:
Clinical Analysis: 30-Year-Old Male
Presenting complaint: Right iliac fossa (RIF) + right loin pain + left iliac fossa (LIF) pain - 1 day duration
Most Likely Diagnosis: Bilateral Ureteric Calculi (Top Priority)
The combination of right loin + right iliac fossa pain is the classical distribution of ureteric colic. The involvement of the left iliac fossa simultaneously strongly points to bilateral ureteric stones, which is a urological emergency.
From S Das - A Manual on Clinical Surgery:
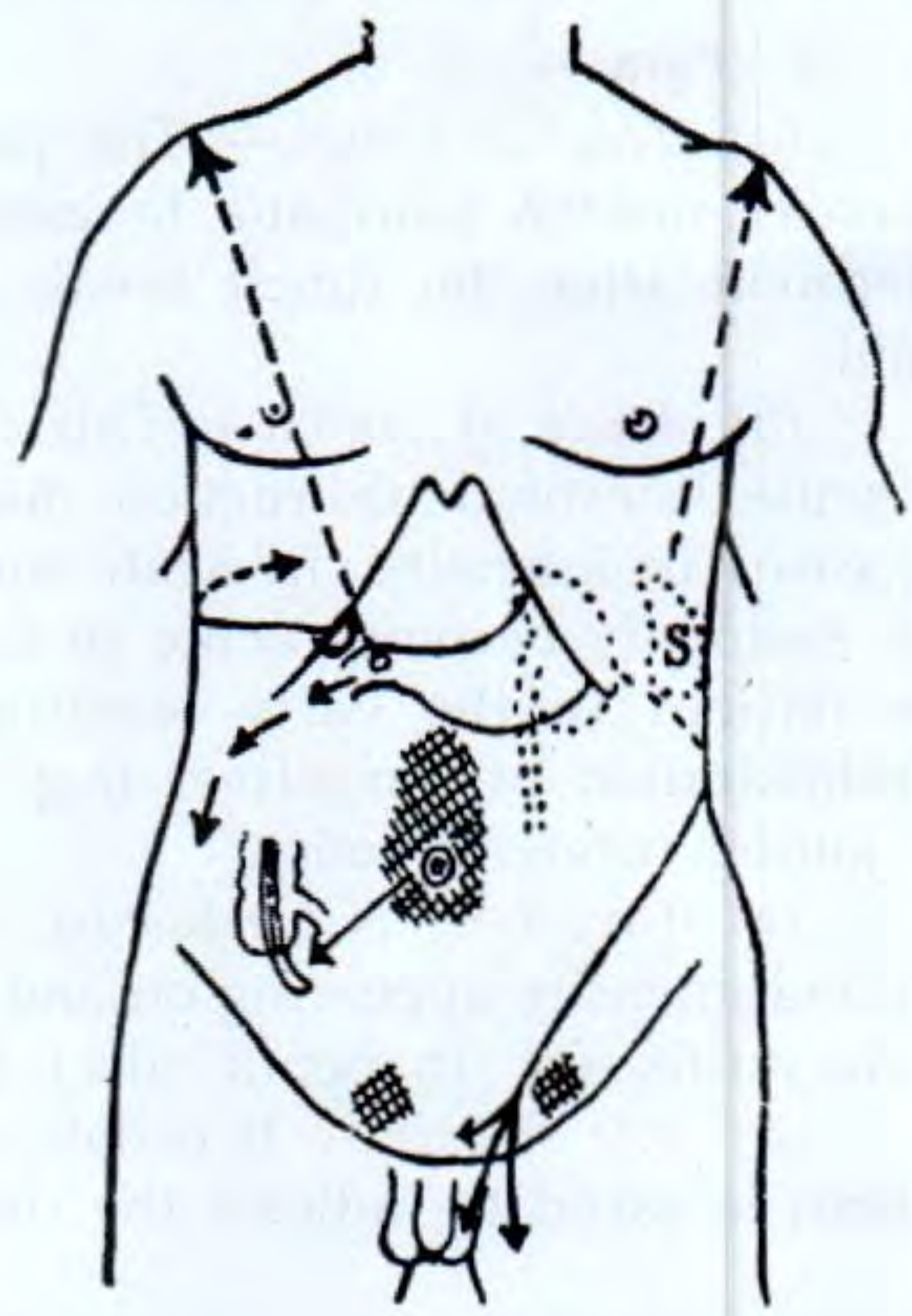
"When the stone is in the upper 1/3rd of the ureter, pain starts in the loin or near the renal angle and gradually radiates to the groin... At a lower level, pain commences rather anteriorly just above the iliac crest and is referred along the branches of the genitofemoral nerve to the testis in the male." - S Das, Manual on Clinical Surgery
The right loin-to-RIF radiation = right ureteric stone. The left iliac fossa pain = left ureteric stone (lower third, no loin component yet, or loin pain was not volunteered).
Key features to ask about:
- Colicky, episodic, severe griping pain (comes and goes suddenly)
- Radiation to the right testis or inner thigh
- Haematuria (frank or microscopic)
- Nausea/vomiting
- Dysuria or strangury (if stone near vesicoureteric junction)
- Previous stone history
Differential Diagnoses
Right-Sided (RIF + Loin)
| Diagnosis | Supporting Features | Against |
|---|---|---|
| Ureteric colic (right) | Colicky loin-to-groin pain, haematuria, young male | - |
| Acute appendicitis | RIF pain, male age group, fever, anorexia, nausea | No classical periumbilical-to-RIF migration described; bilateral involvement unusual |
| Testicular torsion | RIF pain can be referred from torsion in young males - "easily missed" (Bailey & Love) | Check the scrotum in every case |
| Renal pathology | Hydronephrosis, PUJ obstruction - constant gnawing loin pain | Usually unilateral |
| Rectus sheath haematoma | RIF pain after strenuous exercise, no GI upset | Rare |
| Psoas abscess / IlIocaecal TB | RIF mass, vague ill health, weight loss | Duration only 1 day |
| Crohn's disease (terminal ileitis) | RIF pain, chronic, diarrhoea | Acute onset 1 day |
| Perforated duodenal ulcer | Rigidity, pain migrating to RIF via right paracolic gutter | Would be peritonitic and unwell |
Left-Sided (LIF)
| Diagnosis | Supporting Features |
|---|---|
| Ureteric colic (left) | Part of bilateral stone disease |
| Sigmoid diverticulitis | LIF pain, but unusual at age 30 |
| Constipation / sigmoid distension | Common, may co-exist |
Immediate Workup
Bedside
- Urine dipstick - haematuria strongly supports ureteric colic
- Urine microscopy and culture (rule out infection/pyonephrosis)
- Temperature, pulse, BP - fever + loin pain = infected obstructed kidney (emergency)
- Examine the scrotum (rule out torsion)
Bloods
- FBC (leucocytosis suggests inflammation/infection)
- Serum creatinine and electrolytes (renal function - bilateral obstruction risk)
- Serum amylase/lipase (exclude acute pancreatitis in RIF/loin pain differential)
- Serum uric acid, calcium (stone workup)
Imaging
- CT KUB (non-contrast CT abdomen/pelvis) - gold standard for urolithiasis, shows stones, hydronephrosis, and excludes other pathology
- Ultrasound abdomen - quick, no radiation, detects hydronephrosis, appendix if visualised, can assess for appendicitis
- X-ray KUB - only shows radio-opaque stones (calcium oxalate/phosphate); misses uric acid stones
Red Flags Requiring Urgent Action
If this patient has bilateral ureteric obstruction + fever or rising creatinine, this is a urological emergency requiring same-day urology review and possible nephrostomy or JJ stenting.
- Fever + rigidity = infected obstructed kidney -> sepsis risk
- Bilateral obstruction = acute obstructive uropathy -> renal failure
- Inability to pass urine = complete bilateral obstruction
Initial Management (While Awaiting Workup)
- Analgesia: NSAIDs (diclofenac 75 mg IM or rectal) are first-line for ureteric colic - superior to opioids for ureteric smooth muscle; ketorolac IV is an alternative
- IV fluids if vomiting
- Alpha-blocker (tamsulosin 0.4 mg OD) - facilitates stone passage (medical expulsive therapy) for stones <10 mm
- NPO if surgical intervention looks likely
- Urgent urology referral given bilateral involvement
Bottom line: This 30-year-old male almost certainly has bilateral ureteric calculi until proven otherwise. The combination of right loin + right and left iliac fossa pain is the anatomical hallmark. Bilateral obstruction needs urgent imaging and urology input today. - Bailey and Love's Short Practice of Surgery 28th Ed; S Das Manual on Clinical Surgery 13th Ed
This is a shared conversation. Sign in to Orris to start your own chat.