Hyperprolactinemia
Reading File
Finding Sources
Searching PubMed
"hyperprolactinemia"[MeSH Terms] AND ("diagnosis" OR "treatment")
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have everything needed for a thorough, well-structured answer. Here it is:
Hyperprolactinemia
Definition and Normal Values
Hyperprolactinemia is defined as a serum prolactin (PRL) level above the upper limit of normal. Normal PRL is generally <20 ng/mL in women and <15 ng/mL in men (though reference ranges vary slightly by assay). It is the most common hypothalamic-pituitary disorder encountered in clinical endocrinology and can affect fertility, gonadal function, and bone health.
- Prevalence: <1% of the general population, but up to 14% of women with abnormal menses
- PRL >200 ng/mL strongly suggests a prolactinoma (macroadenoma)
Physiology of Prolactin
- Secreted by lactotropes of the anterior pituitary
- Primarily under tonic inhibitory control by hypothalamic dopamine (DA) - dopamine keeps PRL suppressed under normal conditions
- Stimulatory factors: TRH, VIP, estrogen, serotonin, opioids
- Main physiologic roles: mammary gland development and lactation; suppresses GnRH pulsatility
Any process that reduces dopamine delivery to lactotropes (hypothalamic or stalk lesions, DA-blocking drugs) OR any autonomous PRL-secreting tumor leads to hyperprolactinemia.
Etiology / Causes
I. Physiologic
| Cause | Mechanism |
|---|---|
| Pregnancy | Estrogen stimulates lactotrope hyperplasia |
| Lactation / nipple stimulation | Suckling reflex arc |
| Sleep | Nocturnal PRL surge (reverts within 1h of waking) |
| Stress, exercise | Transient |
| Sexual orgasm | Transient |
II. Pharmacologic (Drug-Induced) - Very Common
Dopamine antagonists or agents disrupting dopaminergic tone:
- Antipsychotics (risperidone, haloperidol, phenothiazines) - risperidone can push PRL >200 ng/mL
- Antidepressants (TCAs, SSRIs less so)
- Antiemetics (metoclopramide, domperidone, prochlorperazine)
- Antihypertensives - methyldopa (inhibits DA synthesis), verapamil (blocks DA release)
- Opioids / H2 blockers (cimetidine)
- Estrogens (directly stimulate lactotropes)
- Drug-induced PRL is typically <100 ng/mL
III. Pathological - Pituitary / Hypothalamic
| Cause | PRL Level | Notes |
|---|---|---|
| Microprolactinoma (<1 cm) | Variable, often 100-250 ng/mL | Most common pituitary tumor in women |
| Macroprolactinoma (≥1 cm) | Often >250, can be in thousands | More common in men; mass effects |
| Stalk compression (any non-lactotrope mass) | Typically 30-100 ng/mL | Blocks dopamine delivery |
| Hypothalamic tumors/cysts | 30-100 ng/mL | Craniopharyngioma, germinoma |
| Infiltrative disease | 30-100 ng/mL | Sarcoidosis, histiocytosis X, TB |
| Radiation-induced damage | Varies | Loss of dopaminergic neurons |
| GH- or ACTH-secreting adenomas | Varies | Plurihormonal co-secretion |
IV. Systemic Disease
- Primary hypothyroidism - elevated TRH compensatorily stimulates both TSH and PRL (always check TSH)
- Chronic renal failure - reduced peripheral PRL clearance
- Cirrhosis - impaired PRL metabolism
- Polycystic ovarian syndrome (PCOS) - up to 30% have mildly elevated PRL
V. Macroprolactinemia (Artifact)
PRL can dimerize ("big prolactin") or complex with IgG ("big-big prolactin / macroprolactin") - these complexes are biologically inactive but measured as elevated by some immunoassays. This is a benign condition. Polyethylene glycol (PEG) precipitation differentiates macroprolactin from true monomeric PRL.
Pathophysiology of Symptoms
Elevated PRL suppresses hypothalamic GnRH pulsatility → decreased LH and FSH → hypogonadotropic hypogonadism.
- Women: low estrogen → menstrual irregularity → oligomenorrhea → amenorrhea; infertility; osteopenia (direct PRL effect + indirect estrogen deficiency)
- Men: low testosterone → decreased libido, impotence, oligospermia, reduced muscle mass, osteopenia; late presentation since male hypogonadism symptoms are subtle
- Both sexes: galactorrhea (PRL drives milk production when breast tissue is primed by estrogen)
Clinical Features
Women (Premenopausal)
- Amenorrhea or oligomenorrhea (most common presenting symptom)
- Galactorrhea - present in up to 80%; may be bilateral/spontaneous or unilateral/manual
- Infertility (anovulation)
- Decreased libido, vaginal dryness
- Mild hirsutism and weight gain
- Osteopenia/osteoporosis (with sustained hypoestrogenemia)
- Primary amenorrhea if onset before menarche
Note: Postmenopausal women do not develop galactorrhea despite elevated PRL because estrogen priming is absent.
Men
- Decreased libido, impotence (usually the presenting complaint)
- Oligospermia, infertility
- Osteopenia, reduced muscle mass, decreased beard growth
- Galactorrhea - rare (requires elevated estrogen, e.g., in cirrhosis)
- Visual field defects (bitemporal hemianopsia from optic chiasm compression by large tumor) - men often present late with macroadenomas
- Headaches
Diagnosis
Step 1: Serum PRL
- Measure under resting conditions (minimal stress, no breast stimulation, morning sample)
- Borderline elevation: repeat on at least 2 separate occasions
- PRL >200 ng/mL: very likely prolactinoma (macroadenoma)
- PRL 100-200 ng/mL: adenoma possible; MRI mandatory
- PRL <100 ng/mL: microadenoma, drug-induced, stalk effect, or systemic cause
Hook Effect (Prozone Effect): Very high PRL levels (macroprolactinoma with PRL >1000 ng/mL) can saturate the immunoassay antibodies and give a falsely low reading. Suspect this when a large pituitary mass has a "low" PRL - request serial dilutions.
Step 2: Exclude Secondary Causes
- TSH - rule out hypothyroidism
- Serum creatinine/BUN - rule out renal failure
- Pregnancy test (urine/serum hCG) in all women of reproductive age
- Drug history (careful medication review)
- Consider macroprolactin if PRL is mildly elevated with no symptoms (PEG precipitation assay)
Step 3: MRI of the Pituitary
- Indicated in all patients with:
- PRL >100 ng/mL
- Symptomatic hyperprolactinemia (galactorrhea, amenorrhea, visual symptoms)
- No obvious drug/systemic cause
- Classifies tumor as microadenoma (<1 cm) or macroadenoma (≥1 cm)
- For macroadenomas: also perform formal visual field testing (Goldman or Humphrey perimetry)
Treatment
Treatment goal: normalize PRL, alleviate hypogonadism, stop galactorrhea, preserve/restore bone density, and - for prolactinomas - reduce tumor size.
Treat the Underlying Cause First
- Drug-induced: withdraw offending drug if possible; for psychiatric patients, supervised dose reduction, drug switch (e.g., quetiapine has lower PRL-elevating potential), or cautious DA agonist co-administration (note: DA agonists may worsen psychosis)
- Hypothyroidism: thyroid hormone replacement normalizes PRL
- Renal failure: PRL often normalizes after successful renal transplantation
- Stalk compression by non-functioning tumor: surgical resection can reverse hyperprolactinemia
- Idiopathic hyperprolactinemia: spontaneous resolution occurs in up to 30% of cases; only treat if symptomatic
Dopamine Agonists - First-Line for Prolactinomas
Both are ergoline derivatives acting on D2 receptors on lactotropes to suppress PRL synthesis and secretion, and to shrink tumor mass.
Cabergoline (preferred)
- Dose: 0.5-1.0 mg orally twice weekly, titrated to lowest effective dose
- Achieves normoprolactinemia in ~80% of microadenomas and ~70% of macroadenomas
- Reduces tumor size in 80-90% of macroprolactinomas
- Long half-life (>14 days after single dose); better tolerability than bromocriptine
- Galactorrhea resolves in 90% of patients
- Visual field defects can begin improving within days
- Caution: doses >2 mg/week long-term - concern for cardiac valve fibrosis (particularly tricuspid); echocardiogram recommended yearly for patients on >5 mg/week or with known valvular disease
Bromocriptine
- Dose: start 0.625-1.25 mg at bedtime with a snack, gradually increased to 2.5-15 mg/day
- Preferred when pregnancy is desired (more safety data in pregnancy; short-acting so can be stopped quickly once pregnant)
- More GI side effects (nausea, vomiting, dizziness) than cabergoline
- Can be administered vaginally in women to improve tolerability
Monitoring Response
- PRL measured at regular intervals after dose adjustments
- For macroadenomas: repeat MRI within 16 weeks of starting therapy; then annually
- Target PRL: <10 ng/mL (Goldman-Cecil recommendation)
- ~20% of patients (especially males) are resistant to dopaminergic treatment due to decreased D2 receptor numbers
Stopping Therapy
- Microadenomas: after 2+ years of normoprolactinemia and significant tumor shrinkage, may cautiously withdraw DA agonist with close monitoring; ~5% achieve permanent remission
- PRL and MRI repeated at 3 months, 6 months, then annually after stopping
- Macroadenomas: higher recurrence risk; generally require longer treatment
Surgery (Transsphenoidal Adenomectomy)
- Indicated when:
- DA agonist intolerance or resistance
- Tumor growth despite medical therapy
- Apoplexy with acute visual loss
- Patient preference (desire for drug-free state)
- Cure rates: ~70-80% for microadenomas, ~30% for macroadenomas
- Risk of CSF leak, hypopituitarism, diabetes insipidus
Radiotherapy
- Reserved for aggressive or malignant prolactinomas unresponsive to drugs and surgery
- Stereotactic radiosurgery (Gamma Knife) for well-defined residual tumors
- Risk of delayed hypopituitarism
Prolactinoma in Pregnancy
- Women with microprolactinomas: very low risk of clinically significant tumor growth during pregnancy (~2-5%); bromocriptine/cabergoline can be stopped once pregnancy is confirmed
- Macroadenomas: ~25% grow significantly during pregnancy; continue dopamine agonist or consider surgery if vision threatened; monitor visual fields each trimester
- Prolactin levels rise physiologically during pregnancy, so PRL measurements are not useful for monitoring tumor growth - rely on symptoms and visual fields
Treatment Algorithm
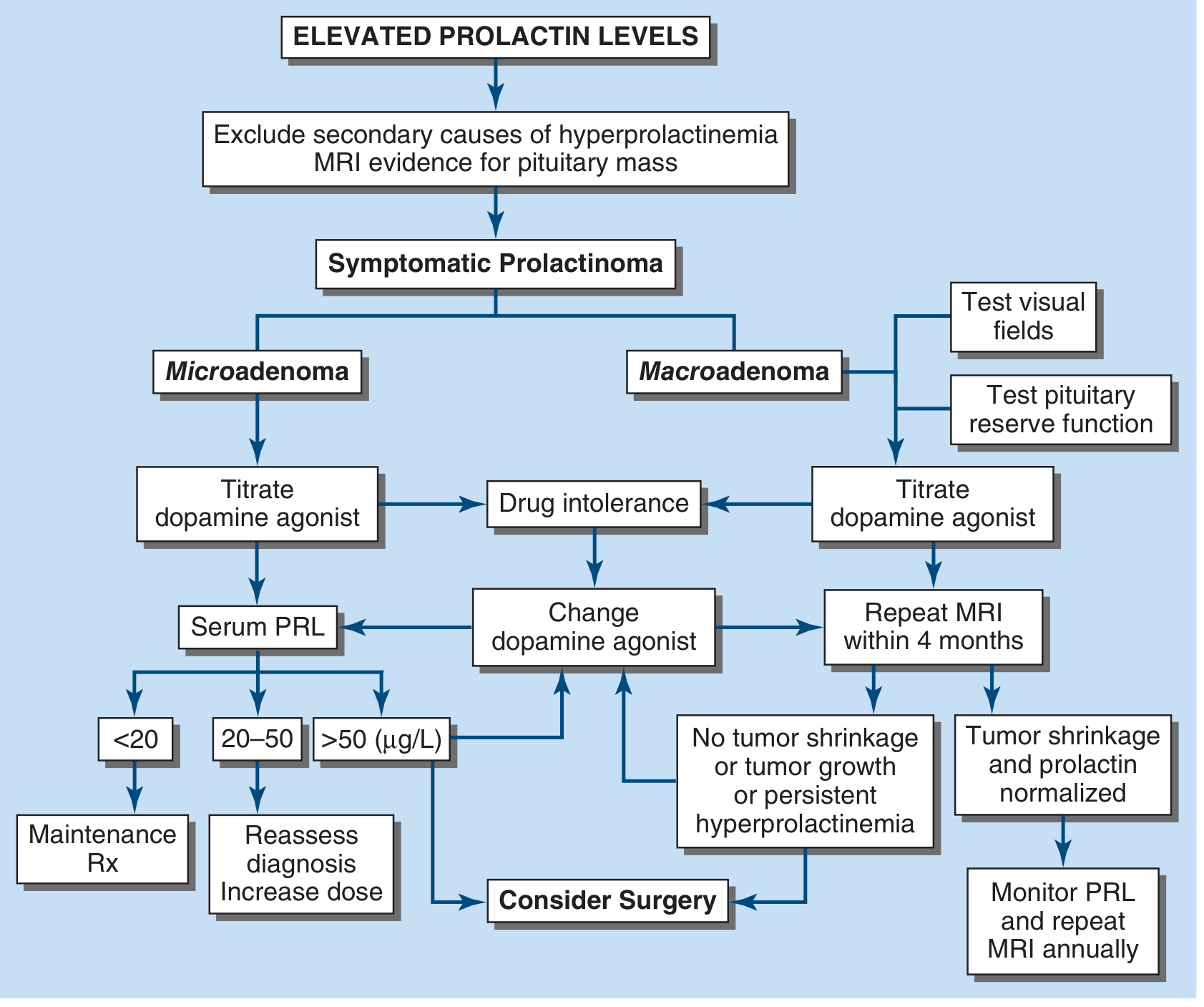
Treatment algorithm for elevated prolactin levels / prolactinoma - Harrison's Principles of Internal Medicine 22e
MRI Response to Cabergoline
Before treatment (A) and after 6 months of cabergoline (B) in a macroprolactinoma:
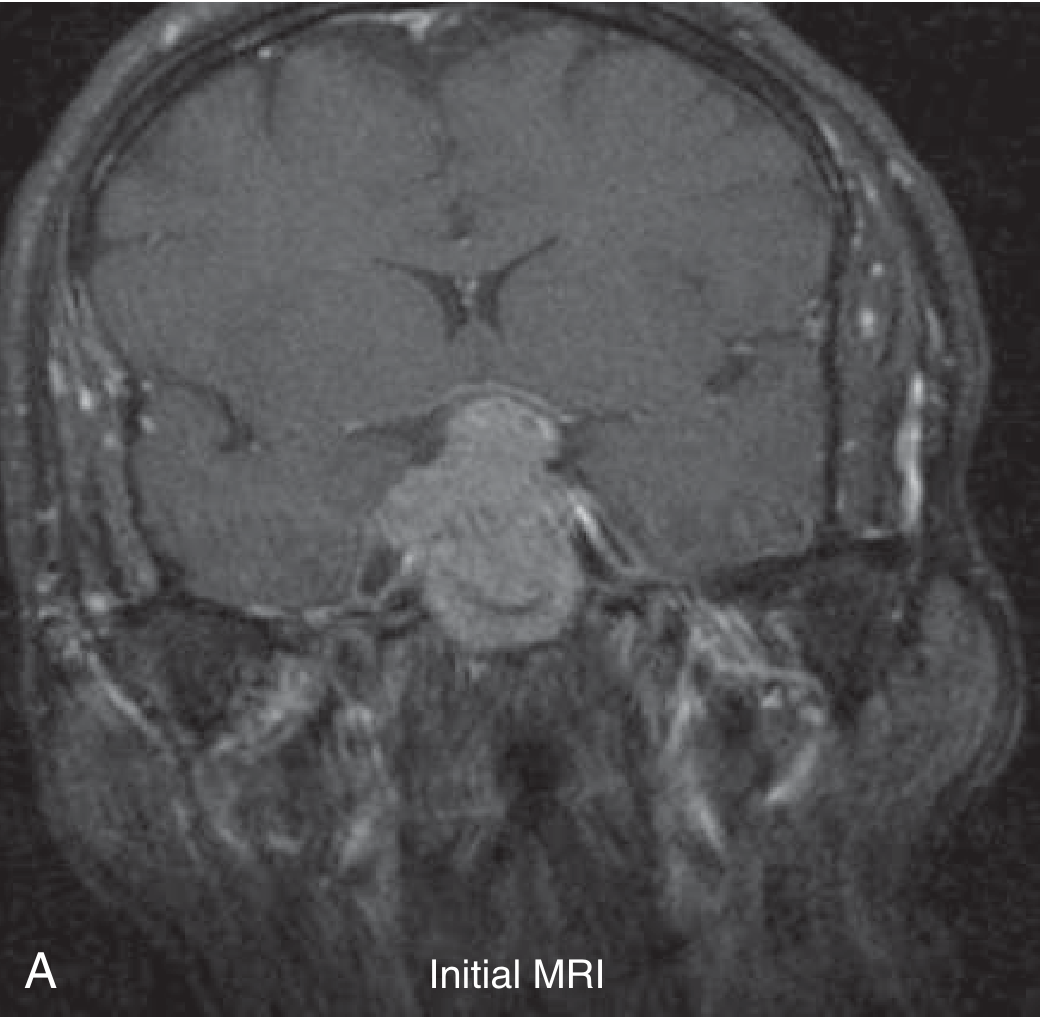
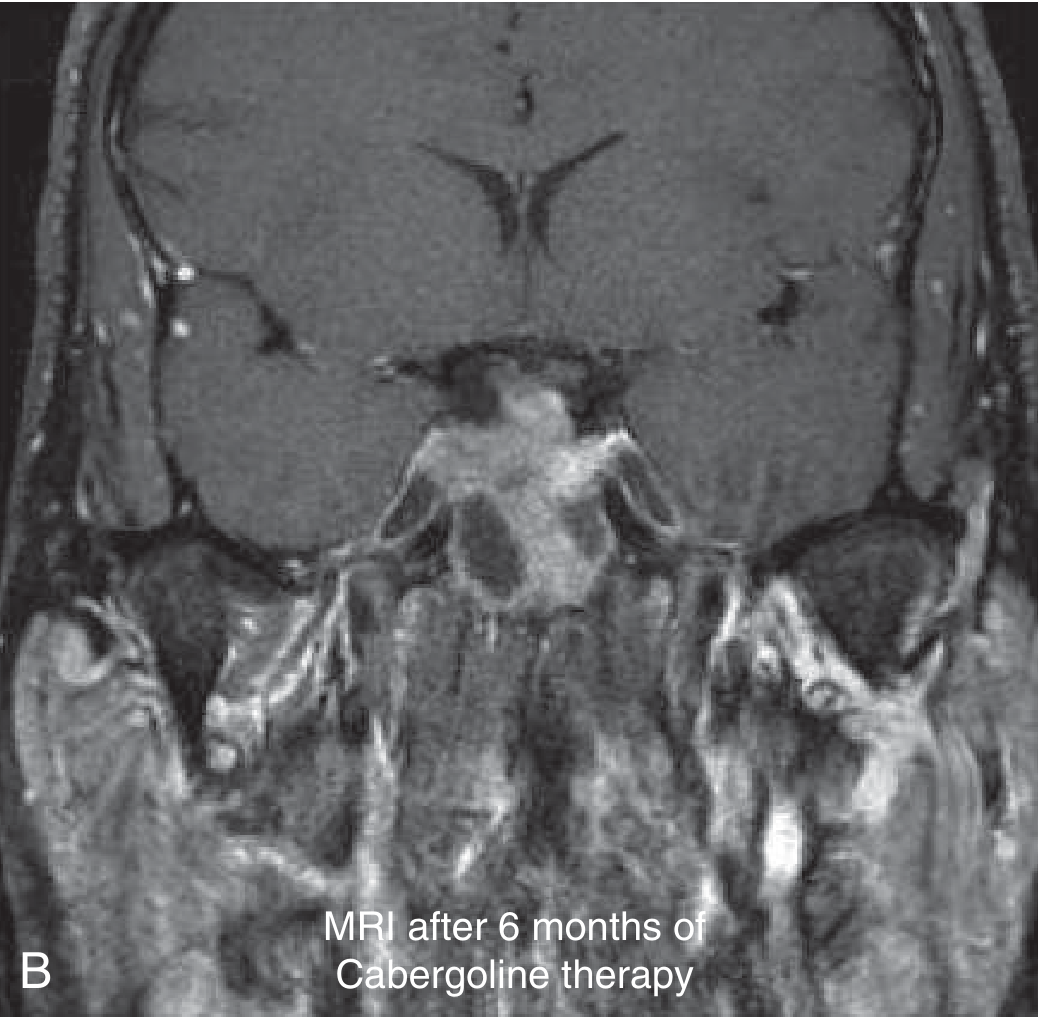
A 43-year-old man with prolactin 8,000 ng/dL and a large sellar mass. After 2 doses of cabergoline, PRL fell to 2,086; after 6 months, PRL was 15 ng/dL with dramatic tumor shrinkage on MRI. - Goldman-Cecil Medicine
Key Differentiating Points
| Feature | Microprolactinoma | Macroprolactinoma | Drug/Stalk Effect |
|---|---|---|---|
| PRL level | Variable, can be any | Usually >250 | Usually <100 |
| MRI | <1 cm lesion | ≥1 cm lesion | Normal or stalk compression |
| Visual fields | Normal | May be impaired | Normal (unless mass) |
| Female:Male ratio | 20:1 | ~1:1 | N/A |
| Risk of progression | ~5% progress to macro | Invasive potential | Resolves with drug change |
| Treatment | DA agonist ± watch | DA agonist first-line | Withdraw drug |
Recent Evidence (PubMed 2024-2026)
- A network meta-analysis (2025) [PMID: 39411853] comparing aripiprazole, bromocriptine, and cabergoline found cabergoline had superior efficacy and favorable safety for hyperprolactinemia treatment.
- A meta-analysis (2024) [PMID: 38945085] in women with PCOS and hyperprolactinemia showed metformin + cabergoline was more effective than metformin alone for reducing prolactin and improving ovulation.
- A systematic review (2024) [PMID: 39627209] in systemic lupus erythematosus found elevated prolactin correlates with disease activity and dopaminergic agonists modestly reduce both prolactin and disease activity.
Sources: Harrison's Principles of Internal Medicine 22e (2025), Goldman-Cecil Medicine (International Ed.), Tietz Textbook of Laboratory Medicine 7e
This is a shared conversation. Sign in to Orris to start your own chat.