Bare area of testis and anatomy of testis and all the surgical land marks importance structure during any surgery around testis must know things in depth
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching the Web
bare area of testis anatomy surgical significance epididymis posterior
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive data to write a thorough in-depth answer. Let me compile everything.
Anatomy of the Testis: In-Depth with Bare Area, Coverings, and Surgical Landmarks
1. Overview and Position
The testes are paired oval male gonads seated obliquely in the scrotum with superior poles directed anterolaterally and inferior poles directed posteromedially. Each normal adult testis measures 4-5 cm long, 3 cm wide, 2.5 cm deep, and 15-25 mL volume. The right testis hangs lower than the left in approximately 85% of men.
The testis has:
- Two surfaces: Lateral (smooth, faces laterally) and Medial (faces the opposite testis)
- Two borders: Anterior border (smooth, free) and Posterior border (where vessels, nerves, and lymphatics enter - this is where the epididymis attaches)
- Two poles: Superior and Inferior
General Anatomy and Musculoskeletal System (THIEME Atlas), p. 247
2. Coverings of the Testis (from superficial to deep)
This is clinically the most tested sequence. From outside inward:
| Layer | Derived From |
|---|---|
| Skin of scrotum | Skin |
| Dartos fascia (no fat, smooth muscle) | Superficial fascia of abdominal wall |
| External spermatic fascia | External oblique aponeurosis |
| Cremasteric fascia and muscle | Internal oblique muscle |
| Internal spermatic fascia | Transversalis fascia |
| Tunica vaginalis - parietal layer | Processus vaginalis (peritoneum) |
| Tunica vaginalis - visceral layer | Processus vaginalis (peritoneum) |
| Tunica albuginea | Fibrous capsule of testis |
| Tunica vasculosa | Innermost vascular layer |
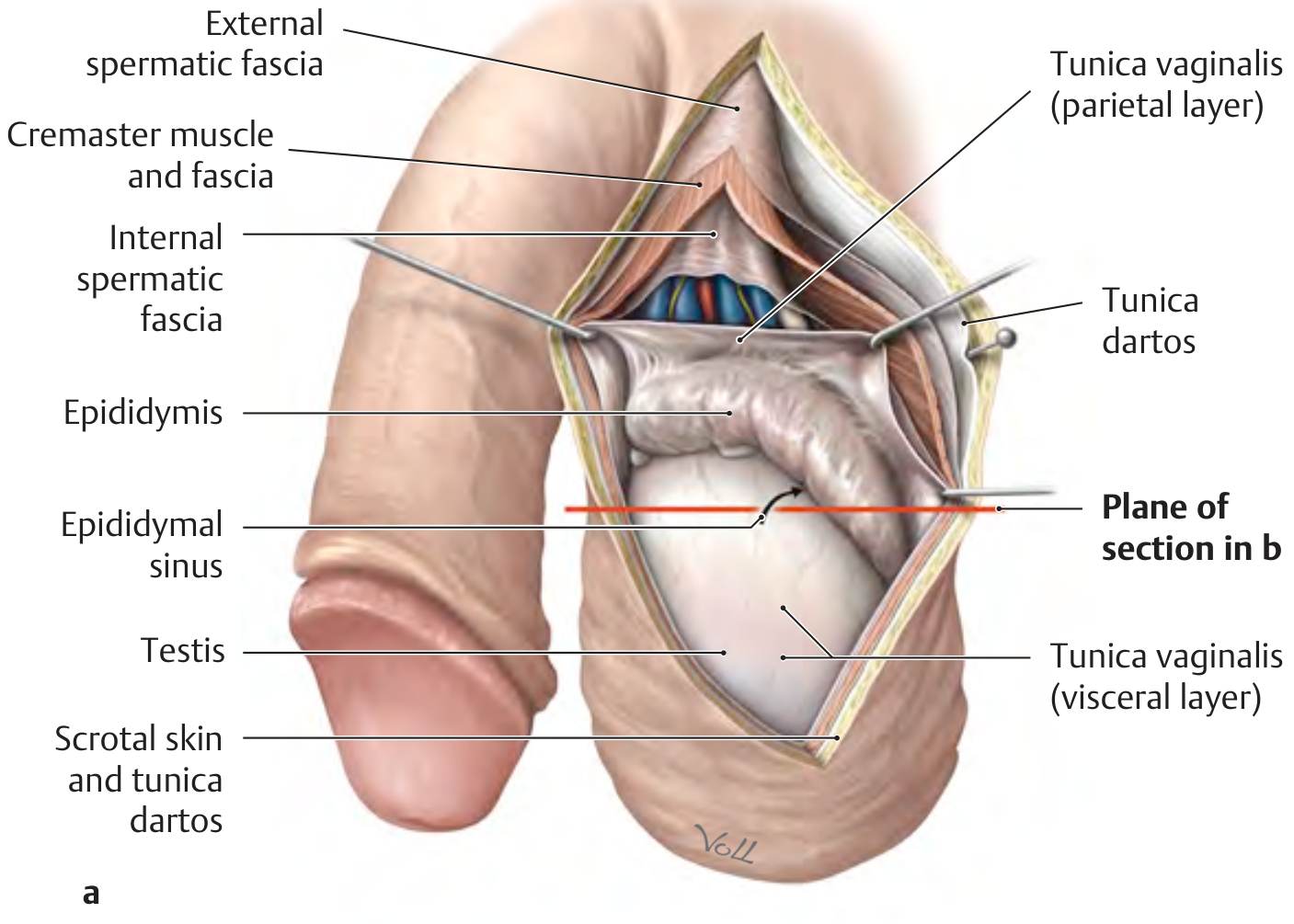
THIEME Atlas of Anatomy: opened tunica vaginalis showing all key layers - external spermatic fascia, cremaster, internal spermatic fascia, tunica vaginalis (parietal and visceral layers), epididymal sinus, testis, and dartos.
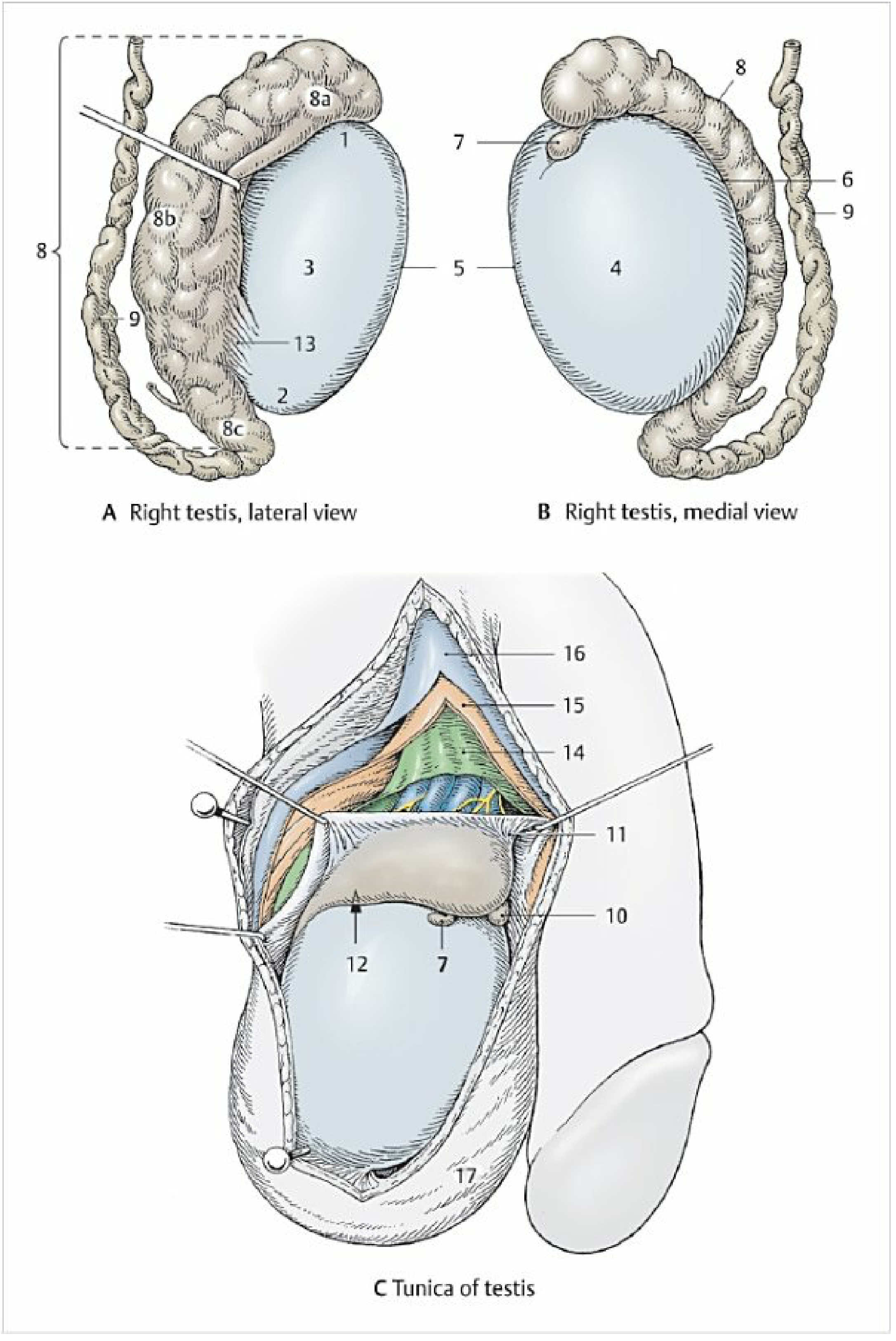
3. The Tunica Vaginalis and the Bare Area
What is the bare area?
The tunica vaginalis is a two-layered peritoneal sac (remnant of the processus vaginalis). Its visceral layer covers all surfaces of the testis and most of the epididymis, EXCEPT for a strip along the posterior border where:
- The epididymis is attached
- Blood vessels, lymphatics, and nerves enter/exit through the mediastinum testis
- The spermatic cord is attached
This posterior strip - where tunica vaginalis does NOT cover - is the bare area of the testis.
Why the bare area matters clinically and surgically
-
Testicular torsion: The bare area is where the testis is anchored. When the tunica vaginalis extends too high on the cord (the "bell-clapper deformity"), the testis loses this posterior fixation and can rotate freely around the cord - this is the anatomical basis for intravaginal testicular torsion. The horizontal lie/"clapper bell" testis on the contralateral side is a hallmark clinical sign.
-
Hydrocele: The tunica vaginalis normally contains only a thin film of fluid between its layers. The bare area is where this serous cavity is absent - fluid collects anteriorly, laterally, and superiorly but NOT posteriorly. This is why hydroceles present as transilluminable anterior swellings and you can always palpate the epididymis and spermatic cord separately at the posterior/superior aspect.
-
Orchidopexy: Sutures for testicular fixation must be placed at the bare area / posterior inferior pole where the scrotal ligament (gubernaculum remnant) exists - NOT through the well-vascularized anterior surface where testicular arteries course.
-
Tumor spread: The tunica albuginea is a strong barrier to tumor spread. Tumors remain confined until they breach the albuginea, but the bare area offers a relative weak point where the tumor can more easily exit the testicular capsule and gain access to peritesticular structures, which changes staging from pT1 to pT2/pT3.
Color Atlas of Human Anatomy Vol. 2, p. 415; Campbell Walsh Wein Urology, p. 1810
4. Internal Architecture
Tunica Albuginea
- Tough fibrous capsule of smooth muscle cells and collagen
- Invaginates posteriorly to form the mediastinum testis - a vertical fibrous septum at the posterior border
- Sends septa inward to divide the testis into 200-300 cone-shaped lobules, each containing 1-4 seminiferous tubules
Mediastinum Testis
- The thickened posterior infolding of the tunica albuginea
- Carries all afferent/efferent structures: testicular artery branches, veins forming the pampiniform plexus, lymphatics, and efferent ductules
- Seen on ultrasound as an echogenic posterior band
- Surgical landmark: This is where the rete testis opens into efferent ductules. Avoid dissecting at the mediastinum during partial orchidectomy or testis-sparing surgery
Internal Tubule System
- Seminiferous tubules (200-300 m total length per testis) → loop within lobules → straighten into tubuli recti → drain into rete testis (within mediastinum) → 12-20 efferent ductules → epididymis caput
Campbell Walsh Wein Urology, p. 1809
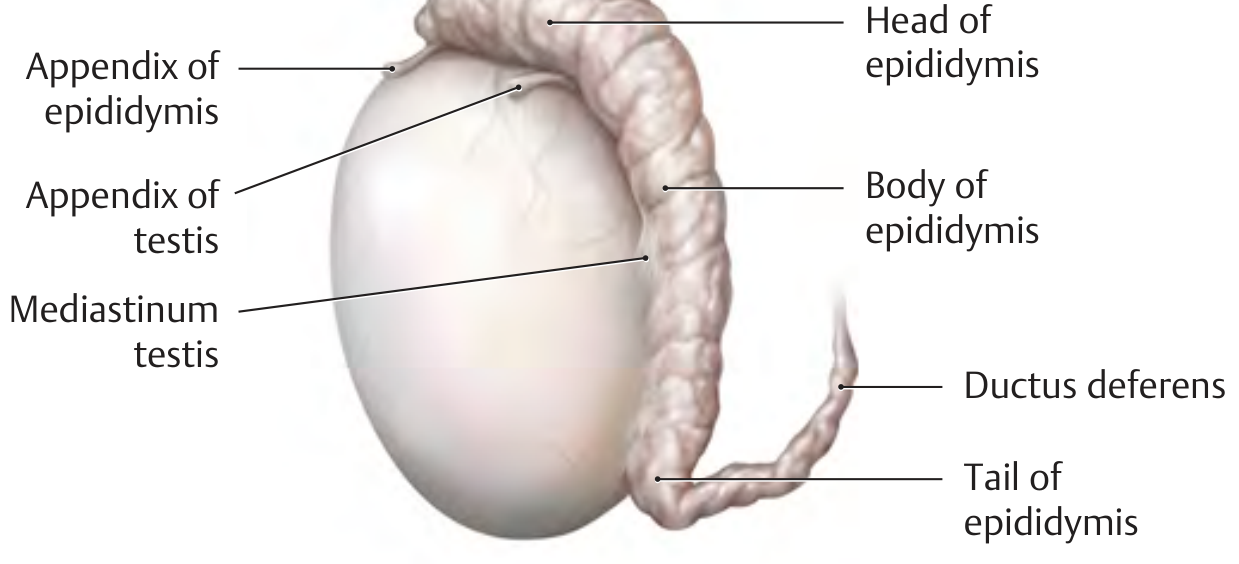
5. The Epididymis
The epididymis is comma-shaped, located on the posterolateral surface of the testis. If uncoiled, it measures ~6 m in length.
Parts:
- Caput (head): Projects above the superior pole; receives efferent ductules from rete testis; isoechoic on USS (10-12 mm diameter)
- Corpus (body): Runs along the posterolateral aspect; hypoechoic on USS (2-5 mm)
- Cauda (tail): At inferior pole; continuous with vas deferens; thicker myometrium
Sinus of the epididymis (digital fossa): A slit-like recess between the body of the epididymis and the lateral surface of the testis, covered by visceral tunica vaginalis on both sides. It is open to the main serous cavity.
Appendix testis: A small pedunculated remnant of the Mullerian (paramesonephric) duct at the superior pole of the testis. Most common structure to undergo torsion in prepubertal boys (the "blue dot sign").
Appendix epididymis: Remnant of the mesonephros (Wolffian duct), found at the head of the epididymis.
6. Blood Supply - The Most Critical Surgical Knowledge
Three arteries supply the testis:
(A) Testicular Artery (= Internal Spermatic Artery)
- Origin: Directly from the abdominal aorta at L2 (just below the renal arteries)
- Crosses the psoas muscle and ureter → enters deep inguinal ring → descends in the spermatic cord
- Main blood supply - its diameter exceeds the deferential + cremasteric arteries combined
- Branches within the spermatic cord (in 31-88% cases, bifurcation occurs within the inguinal canal!)
- Supplies tunica vasculosa of the anterior surface of the upper pole and the anterior, medial, and lateral surfaces of the lower pole
(B) Deferential Artery (= Artery of the vas deferens)
- Origin: Internal iliac artery (or superior vesical artery)
- Travels with the vas deferens
- Supplies vas deferens and epididymis (especially cauda)
- Surgical note: May be compromised at vasectomy. In men with prior vasectomy, the testicular artery becomes the sole major supply - preserve it aggressively during varicocelectomy!
(C) Cremasteric Artery (= External Spermatic Artery)
- Origin: Inferior epigastric artery
- Supplies tunica vaginalis and cremasteric muscle primarily
Anastomoses at the epididymis (surgical safety net): At the head of the epididymis, the testicular and capital arteries anastomose. At the tail, all three arteries form anastomoses. This allows the testis to survive ligation of the testicular artery IF the deferential artery is intact - but this is NOT reliable in adults and should never be relied upon.
Campbell Walsh Wein Urology, p. 1810
7. Venous Drainage
- Small parenchymal veins near the mediastinum and on the surface of the testis → pampiniform plexus
- Pampiniform plexus wraps around the testicular artery in the cord - acts as a countercurrent heat exchanger to cool arterial blood
- Drains: Right testicular vein → IVC at an oblique angle; Left testicular vein → Left renal vein at a right angle (this angle difference explains why left-sided varicoceles are far more common)
- Vena marginalis of Haberer drains corpus/cauda epididymis into the pampiniform plexus or deferential/cremasteric veins
Varicocele point: The increased hydrostatic pressure on the left side (straight-angle drainage into renal vein) is why 80-90% of varicoceles are left-sided or bilateral.
8. Lymphatic Drainage
| Structure | Drains to |
|---|---|
| Testis + caput/corpus epididymis | Para-aortic / interaortocaval nodes (at L1-L2) |
| Cauda epididymis + vas deferens | External iliac nodes |
| Scrotal skin / dartos | Superficial inguinal nodes |
CRITICAL SURGICAL POINT: Testicular tumors metastasize to para-aortic nodes (not inguinal) because the testis originates from the retroperitoneum. Inguinal node involvement only occurs if scrotal skin is involved or prior scrotal surgery has disrupted lymphatic channels. This is why:
- Inguinal orchiectomy (NOT scrotal) is the standard approach for testicular tumors
- Scrotal biopsy for suspected testicular tumor is contraindicated (risks altering lymphatic drainage to inguinal nodes)
9. Nerve Supply
- Visceral afferents and autonomic fibers travel with the testicular artery from the renal and aortic plexuses (T10-T11 sympathetic)
- Additional innervation via the pelvic plexus along the vas deferens
- No somatic innervation - the testis is visceral organ
- Referred pain from the testis maps to the periumbilical/T10 dermatome - hence appendicitis and other T10 pathologies can refer to the testis
Surgical note: Spermatic cord block is placed at the level of the pubic tubercle/external ring, injecting along the anteromedial and anterolateral cord with 1-2% lidocaine WITHOUT epinephrine (to avoid testicular artery spasm). Avoid injecting near the vas.
10. Spermatic Cord Contents
The spermatic cord extends from the deep inguinal ring to the posterior border of the testis. Contents (mnemonic: 3 arteries, 3 nerves, 2 veins, 1 duct, 1 vessel):
Arteries (3):
- Testicular (internal spermatic) artery
- Deferential artery
- Cremasteric artery
Veins (2):
- Pampiniform plexus (→ testicular vein)
- Deferential vein
Nerves (3):
- Genital branch of the genitofemoral nerve (to cremaster)
- Sympathetic fibers (with testicular artery)
- Autonomic fibers (with vas deferens)
Plus: Vas deferens, lymphatics, processus vaginalis remnants
Ilioinguinal nerve travels OUTSIDE the cord in the inguinal canal (within the external oblique aponeurosis), not inside the cord - this is a common anatomy exam trap.
11. Key Surgical Landmarks - Must Know
Scrotal Approach
- Incision: Transverse hemiscrotum or midline raphe
- Layers encountered in sequence: Skin → Dartos → Colles fascia → External spermatic fascia → Cremasteric fascia → Internal spermatic fascia → Parietal tunica vaginalis → Visceral tunica vaginalis → Tunica albuginea
- Gubernaculum/scrotal ligament: Fibrous remnant at the inferior pole attaching the testis to the scrotum - the anchor that prevents retraction. Divide during orchidectomy; preserve during orchidopexy. Its absence or laxity predisposes to torsion
Inguinal Orchiectomy (Standard for Tumor)
- Incision at the inguinal skin crease
- External oblique aponeurosis opened along the axis of its fibers
- Spermatic cord identified at the deep inguinal ring and controlled with a soft clamp BEFORE the testis is delivered (prevents venous spread)
- Ilioinguinal nerve (L1) runs just beneath the external oblique at the medial end - protect it
- Vas deferens and testicular vessels ligated separately at the deep ring
- Never explore testicular tumor through a scrotal incision
Testicular Biopsy
- Incision at medial or lateral surface of the upper pole (NOT the anterior surface and NOT the lower pole)
- Reason: Testicular artery supplies the anterior upper pole and the anterior/medial/lateral lower pole - these are highly vascular
- The upper medial/lateral surface has the most sparse vasculature
- Transverse incision in the tunica albuginea (follows direction of underlying vessels)
- Hinman's Atlas: "Biopsy should be taken from either the medial or lateral aspect of the superior pole where vascularity is sparse, NOT from the well-vascularized anterior surface"
Testicular Torsion
- Surgical approach: Transverse or midline scrotal incision
- Bilateral orchidopexy mandatory - torsion reflects a bilateral anatomic predisposition
- Fixation sutures placed at the bare area (posterior surface) - 3 non-absorbable sutures at posterior, anterolateral, and anteromedial poles securing tunica albuginea to dartos
- Viability assessed after detorsion - if questionable, cover with warm saline swab for 5-10 minutes before deciding on orchidectomy
Orchidopexy for Undescended Testis
- The spermatic cord must be dissected free up to the deep inguinal ring and often retroperitoneally to gain length
- Critical structure: The vas deferens and testicular artery (medial to cord) must be identified separately to avoid injury
- Governaculum divided to mobilize testis
Varicocele Surgery (Microsurgical Inguinal/Subinguinal)
- Preserve the testicular artery (identified with Doppler) and lymphatics (to avoid hydrocele formation post-op)
- All testicular veins ligated while preserving the single testicular artery
- Key landmark: pampiniform plexus wraps tightly around the testicular artery in the cord
12. Tumour Staging and the Bare Area
TNM staging of testicular tumors:
- pT1: Tumor confined to testis/epididymis without vascular invasion; may invade tunica albuginea but NOT tunica vaginalis
- pT2: Tumor extends through tunica albuginea into tunica vaginalis, OR has vascular/lymphatic invasion
- pT3: Invades the spermatic cord
- pT4: Invades the scrotum
The bare area at the posterior border is where tumors breaching the tunica albuginea can directly access the peritesticular tissues and even the spermatic cord (pT3). This directly changes management and prognosis.
Summary: Must-Know List for Surgery Around the Testis
| Point | Why It Matters |
|---|---|
| Bare area = posterior border, no tunica vaginalis | Fixation point; torsion anatomy; tumor spread route |
| Testicular artery from aorta at L2 | Long course - vulnerable during varicocele/hernia repair |
| Three arteries to testis - branching within canal in 31-88% | Don't assume a single artery - identify carefully |
| Biopsy from upper medial/lateral pole only | Avoids the vascular anterior surface |
| Lymphatics drain to para-aortic nodes (not inguinal) | Always use inguinal approach for tumor |
| Ilioinguinal nerve is OUTSIDE the cord | Protect it during inguinal orchidectomy |
| Control cord at deep ring BEFORE delivering testis | Prevents venous tumor spread |
| Bilateral fixation in torsion (even the normal side) | Bilateral anatomic predisposition |
| Deferential artery compromised by vasectomy | Preserve testicular artery rigorously in vasectomized men |
| Mediastinum testis = posterior internal structure | Avoid during testis-sparing surgery |
Sources: Campbell Walsh Wein Urology (10th ed.); THIEME Atlas of General Anatomy; Color Atlas of Human Anatomy Vol. 2 (Sobotta/Schiebler); Hinman's Atlas of Urologic Surgery; Bailey & Love's Short Practice of Surgery (28th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.