
1000128973.jpg
Give me the answer for the essay
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
I now have all the content needed for comprehensive essay answers. Here are the full answers:
GENERAL HUMAN PHYSIOLOGY - SECTION A
SECTION A - I. Elaborate On
1. Hormones Involved in Regulation of Blood Sugar Level - Functions of Insulin - Signs and Symptoms of Diabetes Mellitus (10 marks)
Part A: Hormones Involved in Regulation of Blood Sugar Level
Blood glucose is maintained within a narrow range (70-110 mg/dL fasting) by the coordinated action of several hormones:
1. Insulin (hypoglycemic hormone)
- Secreted by the Beta (B) cells of the islets of Langerhans in the pancreas
- Released in response to rising blood glucose (e.g., after a meal)
- The primary hormone that lowers blood glucose
2. Glucagon (hyperglycemic hormone)
- Secreted by the Alpha (A) cells of the islets of Langerhans
- Released when blood glucose falls
- Stimulates hepatic glycogenolysis (breakdown of glycogen to glucose) and gluconeogenesis (synthesis of glucose from non-carbohydrate precursors like amino acids)
- Acts opposite to insulin - raises blood glucose
3. Epinephrine (Adrenaline)
- Released from the adrenal medulla during stress ("fight-or-flight")
- Stimulates glycogenolysis in both liver and muscle
- Raises blood glucose rapidly
- Also called a "counter-regulatory" or anti-insulin hormone
4. Cortisol (glucocorticoid)
- Released from the adrenal cortex
- Promotes gluconeogenesis in the liver
- Decreases glucose uptake by peripheral tissues
- A counter-regulatory hormone - raises blood glucose
5. Growth Hormone (GH)
- Secreted by the anterior pituitary
- Has anti-insulin effects - decreases glucose uptake and utilization
- Promotes lipolysis, sparing glucose
- Raises blood glucose
6. Thyroid Hormones
- Increase glucose absorption from the gut
- Stimulate glycogenolysis
The interplay: Insulin is the only hormone that lowers blood glucose. All others (glucagon, epinephrine, cortisol, GH) are counter-regulatory and raise blood glucose.
Part B: Functions of Insulin
Insulin is aptly called the "hormone of abundance" because its net effect is the storage of carbohydrate, protein, and fat. Its effects are divided into:
1. On Carbohydrate Metabolism:
- Increases glucose uptake by muscle, adipose tissue, and other peripheral tissues by recruiting GLUT-4 transporters to the cell membrane
- Stimulates glycogenesis (glycogen synthesis) in liver and muscle
- Inhibits glycogenolysis (breakdown of glycogen)
- Inhibits gluconeogenesis in the liver
- Net result: lowers blood glucose (hypoglycemic effect)
2. On Fat (Lipid) Metabolism:
- Promotes lipogenesis (fat synthesis from glucose)
- Inhibits lipolysis (breakdown of stored fat)
- Inhibits ketogenesis (formation of ketone bodies)
3. On Protein Metabolism:
- Increases amino acid uptake by cells
- Stimulates protein synthesis
- Inhibits protein catabolism
4. On Electrolyte Transport:
- Promotes K⁺ entry into cells (lowers plasma K⁺)
- Increases Na⁺ retention by kidneys
5. Growth-promoting effects:
- Stimulates cell growth and DNA synthesis
Note: Insulin acts via tyrosine kinase receptors on cell surfaces. Binding triggers receptor-mediated endocytosis and a cascade of intracellular signals.
Part C: Signs and Symptoms of Diabetes Mellitus
Diabetes mellitus is the constellation of abnormalities caused by insulin deficiency (absolute in Type 1, relative/resistance-based in Type 2). The fundamental defect is: reduced entry of glucose into peripheral tissues + increased glucose liberation from the liver - "starvation in the midst of plenty."
| Classic Triad (3 Ps) | Mechanism |
|---|---|
| Polyuria (increased urine output) | Osmotic diuresis from glucosuria |
| Polydipsia (excessive thirst) | Dehydration from polyuria |
| Polyphagia (increased appetite) | Intracellular glucose deficiency despite high plasma glucose |
Additional Signs and Symptoms:
- Hyperglycemia - fasting blood glucose >126 mg/dL (diagnostic)
- Glycosuria - glucose spills into urine when blood glucose exceeds renal threshold (~180 mg/dL)
- Weight loss - despite increased appetite; due to lipolysis and protein catabolism
- Fatigue and weakness - cellular energy deficiency
- Blurred vision - osmotic changes in the lens
- Recurrent infections - impaired immune function and poor wound healing
- Ketosis and diabetic ketoacidosis (DKA) - in Type 1: fat breakdown produces ketone bodies (acetoacetate, β-hydroxybutyrate, acetone)
- Metabolic acidosis - from accumulation of ketoacids
- Kussmaul breathing - deep, labored breathing to compensate for acidosis
- Sweet (fruity) breath - from exhaled acetone
- Neuropathy - tingling/numbness in extremities (peripheral neuropathy)
- Diabetic coma - in severe untreated cases
Type 1 DM: Autoimmune destruction of B cells; presents acutely in children; requires insulin
Type 2 DM: Insulin resistance + B cell dysfunction; typically in overweight adults; managed with lifestyle changes and oral hypoglycemics
(Ganong's Review of Medical Physiology, 26th Ed.)
SECTION B - II. Write Notes On
1. Draw a Normal Electrocardiogram and Write Briefly About the Different Waves (5 marks)
An electrocardiogram (ECG/EKG) is a recording of the fluctuations in electrical potential that arise from the algebraic sum of the action potentials of all myocardial fibers, recorded from the body surface. Because body fluids are good conductors, the heart acts as a current source in a volume conductor.
Normal ECG Diagram:
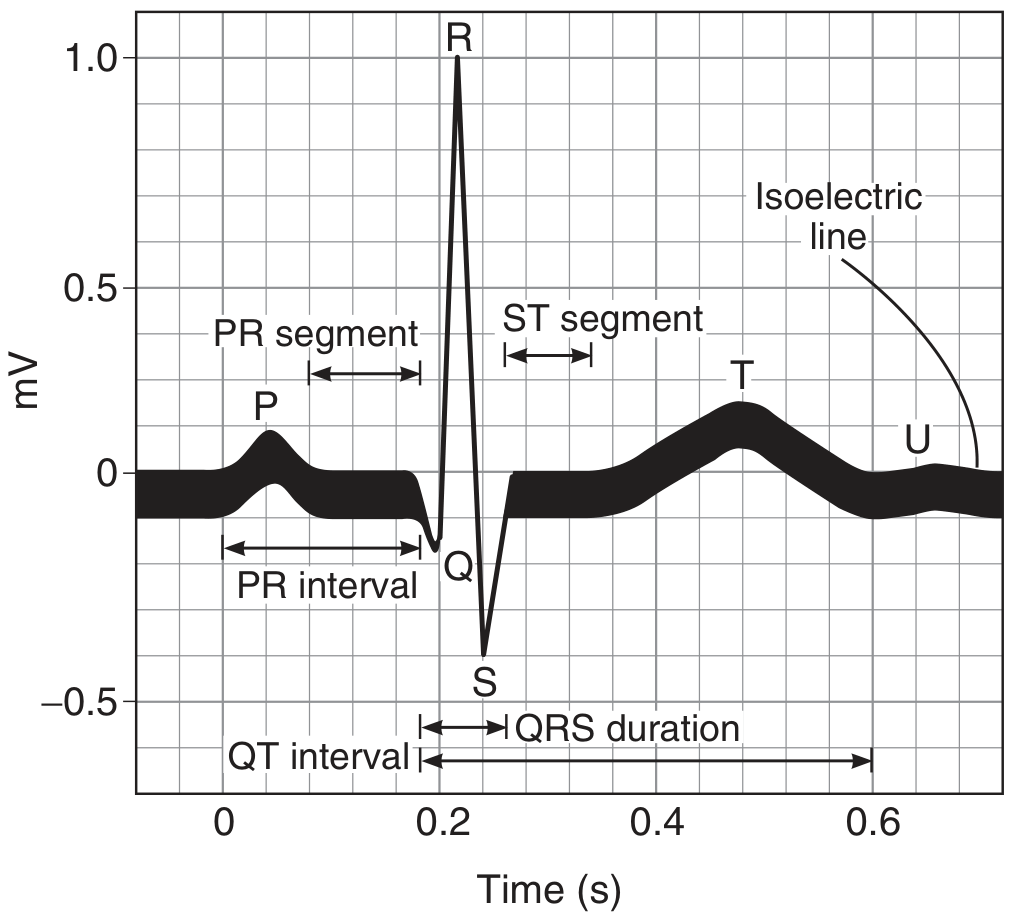
The Waves and Their Significance:
| Wave/Segment | Electrical Event | Normal Duration/Amplitude |
|---|---|---|
| P wave | Atrial depolarization | 0.08-0.10 s; <2.5 mm |
| PR interval | AV conduction time (from atrial to ventricular depolarization) | 0.12-0.20 s (avg 0.18 s) |
| QRS complex | Ventricular depolarization | 0.08-0.10 s |
| - Q wave | Initial septal depolarization (left to right) | Small, narrow |
| - R wave | Main ventricular depolarization (upward) | Tallest deflection |
| - S wave | Terminal ventricular depolarization | Downward deflection |
| ST segment | Plateau of ventricular action potential (no net current flow) | Isoelectric (avg 0.32 s) |
| T wave | Ventricular repolarization | Upright in most leads |
| QT interval | Total ventricular action potential duration | 0.40-0.43 s |
| U wave | Possibly slow repolarization of papillary muscles / ventricular myocytes with long action potentials | Inconstant; follows T wave |
Key Points:
- A positive deflection is written when depolarization moves toward the active electrode
- A negative deflection is written when depolarization moves away from the active electrode
- The ECG is recorded from 12 leads: 3 standard bipolar limb leads (I, II, III), 3 augmented unipolar leads (aVR, aVL, aVF), and 6 chest (precordial) leads (V1-V6)
- The PR interval reflects AV nodal delay (~0.1 s), which is shortened by sympathetic stimulation and lengthened by vagal stimulation
(Ganong's Review of Medical Physiology, 26th Ed.)
2. Micturition Reflex (5 marks)
Micturition (urination) is the process of emptying the urinary bladder. It is primarily an autonomic spinal cord reflex that is modulated by higher brain centers.
Anatomy of Control:
- Detrusor muscle - smooth muscle of the bladder wall; contracts during micturition
- Internal urethral sphincter - smooth muscle; under involuntary (autonomic) control
- External urethral sphincter - skeletal muscle; under voluntary (somatic) control via pudendal nerve
The Micturition Reflex - Step by Step:
-
Bladder filling - As urine accumulates, the bladder wall stretches. Intravesical pressure rises progressively.
-
Stretch receptor activation - Sensory stretch receptors in the bladder wall (especially the posterior urethra) are activated. Signals travel via the pelvic nerves to the sacral segments (S2-S4) of the spinal cord.
-
Reflex arc - Parasympathetic signals return via the pelvic nerves to the detrusor muscle, causing it to contract. This is the core micturition reflex.
-
Self-regenerative cycle - Initial detrusor contraction further stretches receptors, generating more sensory impulses, causing stronger contraction - a positive feedback loop - until the bladder reaches strong contraction.
-
Sphincter inhibition - When the micturition reflex becomes strong enough, a reflex passes via the pudendal nerve to inhibit the external sphincter, allowing urine to flow.
-
Reflex fatigue - After a few seconds to over a minute, the reflex fatigues; the bladder relaxes, and intravesical pressure returns to baseline.
Higher Center Control:
- Brain stem (pons) - Contains both strong facilitative and inhibitory micturition centers
- Cerebral cortex - Mainly inhibitory; allows voluntary postponement of urination
- Higher centers keep the reflex partially inhibited; only when socially convenient do cortical centers facilitate the sacral micturition center and simultaneously relax the external sphincter
- Voluntary urination: Cortical centers facilitate the sacral centers + inhibit the external sphincter simultaneously
Abnormalities:
- Spinal cord injury above sacral level - reflex micturition is preserved but voluntary control is lost ("uninhibited bladder")
- Spinal cord injury at sacral level - abolishes the reflex entirely (atonic bladder/urinary retention)
- Infants - micturition is purely reflex until cortical control develops
(Guyton and Hall Textbook of Medical Physiology)
3. Muscles of Respiration (5 marks)
Breathing involves the coordinated action of several muscle groups that alter thoracic volume to create pressure gradients for airflow.
Diagram:
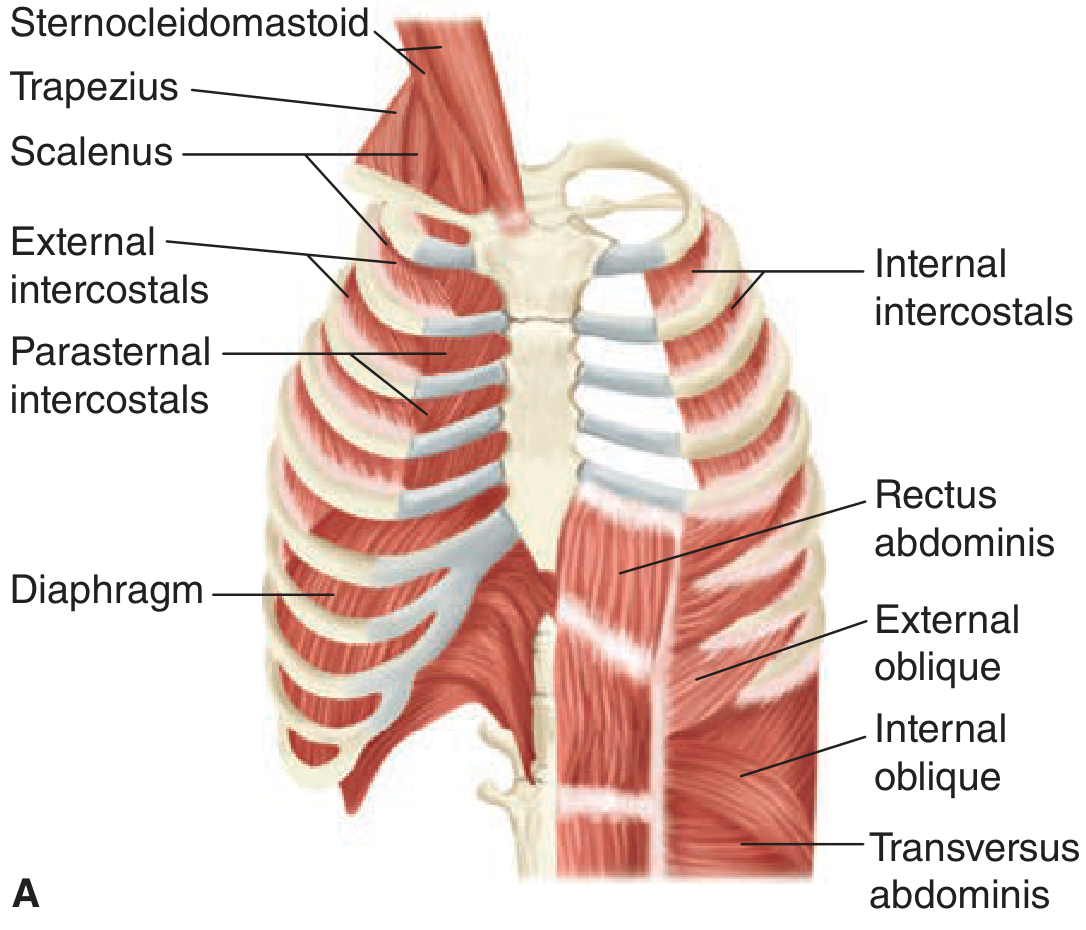
A. Muscles of Inspiration (Active):
1. Diaphragm (Primary muscle of inspiration):
- The most important respiratory muscle; dome-shaped musculotendinous sheet separating thorax from abdomen
- Innervated by the phrenic nerves (C3, C4, C5)
- On contraction: the dome descends, increasing the vertical diameter of the thorax
- Has two parts: costal (attached to lower ribs) and crural (attached to vertebral ligaments)
- Either the diaphragm alone or external intercostals alone can maintain adequate ventilation at rest
- Transection above C3 is fatal without mechanical ventilation; below C5 spares phrenic nerves and preserves breathing
2. External Intercostal Muscles:
- Run obliquely downward and forward from rib to rib
- On contraction: elevate the lower ribs, increasing the anteroposterior and transverse diameter of the thorax (pump-handle and bucket-handle movements)
- Innervated by intercostal nerves
Accessory Muscles of Inspiration (used during deep/labored breathing):
| Muscle | Action |
|---|---|
| Sternocleidomastoid | Elevates the sternum and upper rib cage |
| Scalene muscles | Prevent inward displacement of upper ribs during inspiration; elevate first two ribs |
| Trapezius | Assists in elevation of rib cage |
| Pectoralis major/minor | Expand rib cage when arms are fixed |
B. Muscles of Expiration:
Quiet (normal) expiration is passive - it occurs due to the elastic recoil of the lungs and chest wall; no muscles needed.
Forced/active expiration uses:
| Muscle | Action |
|---|---|
| Internal intercostal muscles | Run obliquely downward and posteriorly; depress the rib cage, decreasing thoracic volume |
| Rectus abdominis | Pulls rib cage downward and inward; increases intra-abdominal pressure |
| External oblique | Compresses abdominal contents; pushes diaphragm upward |
| Internal oblique | Same as above |
| Transversus abdominis | Increases intra-abdominal pressure; most important abdominal expiratory muscle |
Note: Abdominal muscles aid expiration by pushing the diaphragm upward (increased intra-abdominal pressure) and pulling the rib cage downward and inward.
Glottis Control:
- Abductor muscles of the larynx contract early in inspiration, opening the glottis wide to allow free airflow
- Adductor muscles close the glottis reflexively during swallowing to prevent aspiration
(Ganong's Review of Medical Physiology, 26th Ed.)
Sources:
- Ganong's Review of Medical Physiology, 26th Edition
- Guyton and Hall Textbook of Medical Physiology
- Basic Medical Biochemistry: A Clinical Approach, 6th Edition
This is a shared conversation. Sign in to Orris to start your own chat.