Clinical features of hydrocephalus in pediatrics
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
hydrocephalus children clinical features diagnosis
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Clinical Features of Hydrocephalus in Pediatrics
Hydrocephalus is a pressure-dependent enlargement of the cerebral ventricles due to obstruction or impaired absorption of CSF. In children, clinical presentation varies significantly depending on age (whether sutures are open or fused) and acuity of onset.
Key Dividing Line: Open vs. Fused Sutures
The cranial sutures fuse by approximately age 2-3 years (occasionally up to age 5 under extreme ICP). This is the single most important determinant of how hydrocephalus presents:
| Feature | Infants (open sutures) | Older children (fused sutures) |
|---|---|---|
| Head enlargement | Yes - hallmark sign | No |
| Fontanelle bulging | Yes | Not applicable |
| Papilledema | Absent (skull expands instead) | Present |
| Optic atrophy | May develop late | Possible |
A. Infants and Neonates (Open Sutures)
Head and Skull Signs
- Macrocephaly / rapidly increasing head circumference - the cardinal finding; head soon surpasses the 97th percentile on growth charts. Excessively rapid head growth is the hallmark.
- Bulging, tense anterior fontanelle - present even when the infant is upright and relaxed (normally the fontanelle is flat or soft in the upright position)
- Splayed/separated cranial sutures - palpable on examination
- Engorged/prominent scalp veins - due to venous hypertension
- Frontal bossing - unusually prominent frontal skull regions; the face appears relatively small and "pinched" by comparison
- Thinned, tight scalp skin over the cranial vault
- "Cracked-pot" sound (McEwen's sign) - hollow percussion note heard when the skull is tapped; due to suture separation and thinned bone
- "Beaten silver" appearance on skull X-ray - unevenly thinned inner table from raised ICP
- No papilledema (the expanding skull decompresses pressure; optic discs may become atrophic late)
Behavioral/Systemic Signs
- Irritability - very common early symptom
- Poor feeding - infant appears fretful and feeds poorly
- Frequent vomiting - especially with acute enlargement (due to raised ICP)
- Lethargy / torpor - as ventricles continue to enlarge, the infant becomes languid and uninterested in surroundings, unable to sustain activity
Eye Movement Abnormalities
- "Setting-sun sign" - the most classic ocular sign in infants. The upper eyelids retract, eyes deviate downward and inward, and the sclerae are visible above the iris. Caused by pressure on the midbrain tectum (superior colliculus), producing a Parinaud-type downward gaze paresis. It typically reverses after shunting.
- Sixth nerve (abducens) palsy - may be unilateral or bilateral; produces incomplete horizontal abduction. This can be the only eye finding in milder cases.
- Inward deviation of eyes at rest - seen in more severe or rapidly developing cases
Motor and Neurological Signs
- Lower limb spasticity - can develop at any stage
- Corticospinal tract signs - deep tendon reflexes increased
- Feeble, tremulous arm movements
- Posture: in untreated progressive cases, infant adopts flexed arms with flexed or extended legs
- Developmental delay in motor function - if hydrocephalus is arrested; verbal skills are often surprisingly preserved relative to motor function
B. Children After Suture Closure (Age >2-3 years)
Once sutures are fused, the skull cannot expand, so hydrocephalus produces signs of raised ICP rather than macrocephaly.
Headache
- Often the predominant symptom in older children
- Early morning headache is classic - due to rise in ICP during sleep from increased cerebral blood volume in the recumbent position, combined with hypoventilation-related hypercarbia and increased CBF
- May be accompanied by projectile vomiting on waking
Vomiting
- Frequently occurs in the morning
- Vomiting due to raised ICP is characteristically projectile and may not be preceded by nausea
Visual Symptoms
- Papilledema - present (unlike in infants where skull expansion prevents it)
- Blurred vision / visual spots
- Diplopia - due to sixth nerve palsy (false localizing sign of raised ICP); child may complain of double vision
- Optic atrophy if untreated - with permanent visual loss
Gait and Motor
- Wide-based, ataxic gait - due to stretching of white matter tracts from the frontal leg regions around the enlarged ventricles
- Lower limb spasticity with hyperreflexia
- In posterior fossa tumors causing obstructive hydrocephalus: cerebellar ataxia
Neurological Signs
- Sixth cranial nerve palsy - unilateral or bilateral; "false localizing sign"
- Decreased level of consciousness / somnolence with severe or acute hydrocephalus
- Cushing's triad (hypertension + bradycardia + irregular respirations) - a late, ominous sign of impending herniation
Endocrine Dysfunction (Long-standing Cases)
- Short stature - from pressure on the hypothalamus/pituitary axis
- Menstrual irregularities
- Diabetes insipidus
- These reflect chronic hypothalamic compression
C. CT Appearance
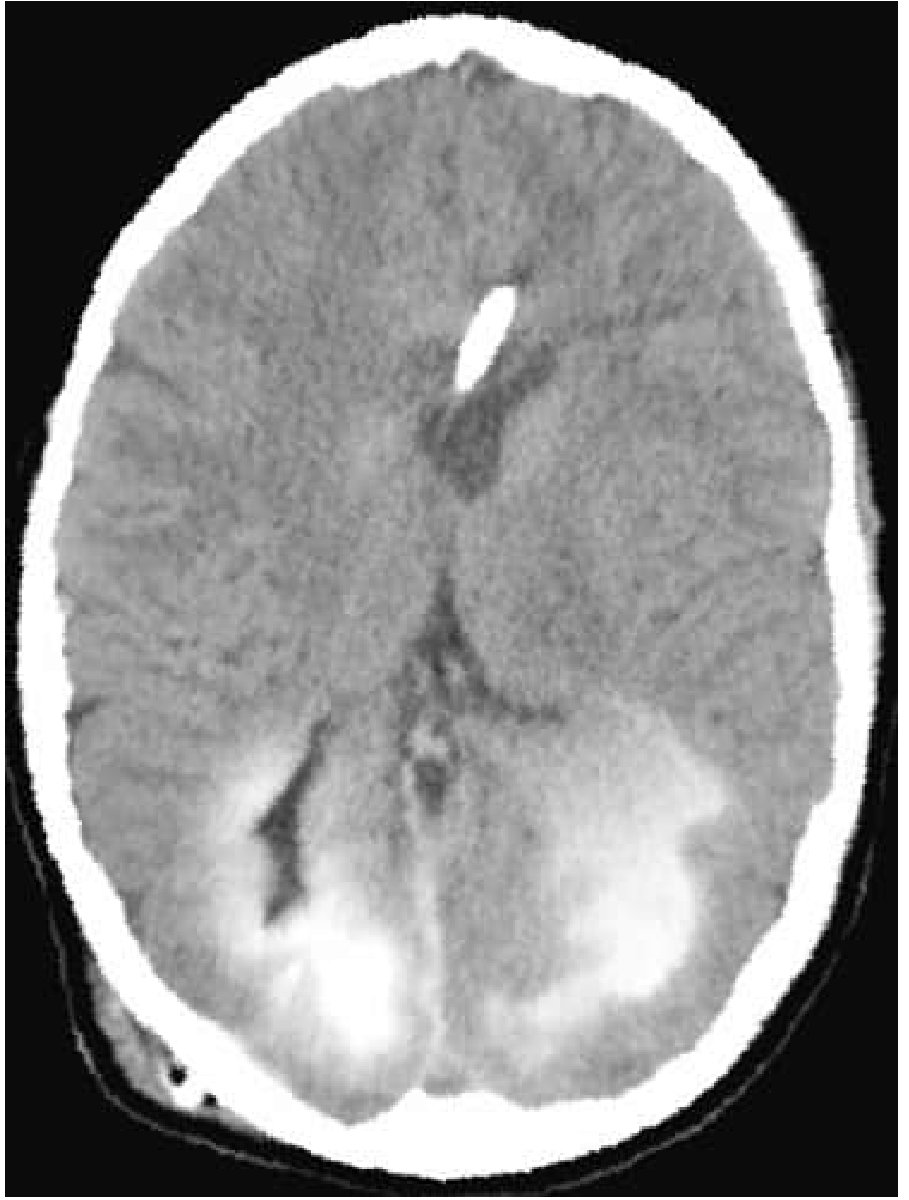
Axial CT with transependymal flow - contrast in the lateral ventricles has diffused through the ependymal lining into surrounding periventricular brain tissue, a hallmark of active, pressure-dependent hydrocephalus.
D. Summary of Clinical Features by Age
| Clinical Feature | Neonate/Infant | Young Child (sutures open, <3y) | Older Child (sutures fused, >3y) |
|---|---|---|---|
| Macrocephaly | +++ | + | - |
| Bulging fontanelle | +++ | + | - |
| Engorged scalp veins | ++ | + | - |
| McEwen's sign | ++ | + | - |
| Setting-sun sign | +++ | + | - |
| Papilledema | - | - | +++ |
| Morning headache | - | +/- | +++ |
| Vomiting | ++ | ++ | ++ |
| CN VI palsy | + | + | ++ |
| Irritability/lethargy | ++ | ++ | + |
| Spasticity (lower limbs) | + | + | + |
| Gait ataxia | - | +/- | ++ |
| Endocrine dysfunction | - | - | + (chronic) |
| Cushing's triad | - | +/- | + (late) |
E. Special Notes
- Premature infants (<1500 g): At high risk for intraventricular hemorrhage; ~25% develop progressive ventricular enlargement, and 5% ultimately require shunting.
- "Bobble-head" syndrome: A rare form from suprachiasmatic arachnoid cyst or third ventricular enlargement causing rhythmic head bobbing.
- Arrested hydrocephalus: Ventricles may remain enlarged with normal ICP; child is typically motor-delayed but often surprisingly verbal.
- Acute exacerbations (even in previously compensated hydrocephalus) can cause sudden vomiting, stupor, or coma.
Sources
- Bradley and Daroff's Neurology in Clinical Practice, Chapter 88 (Hydrocephalus in Children), pp. 1853-1855
- Adams and Victor's Principles of Neurology, 12th ed. (Syndromes of Hydrocephalus), pp. 559-561
- The Harriet Lane Handbook, 23rd ed. (Hydrocephalus with Increased ICP), p. 728
- Neuroanatomy through Clinical Cases, 3rd ed. (Section 5.7 Hydrocephalus), p. 182
- Tintinalli's Emergency Medicine (Clinical Features and Diagnosis - Pediatric CNS Tumors / Obstructive Hydrocephalus)
Recent evidence note: A 2025 systematic review on neuro-ophthalmological findings in pediatric shunt failure (PMID 40215619) confirms that ocular signs - particularly sixth nerve palsy and papilledema - are important early markers of shunt malfunction and should prompt urgent imaging.
This is a shared conversation. Sign in to Orris to start your own chat.