Q. Disciss the role of ethmoid sinus in causation of chronic sinusiris. in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances
ethmoid sinus anatomy role chronic sinusitis pathophysiology
osteomeatal complex ethmoid chronic rhinosinusitis Scott Brown Cummings
ethmoid labyrinth anterior ethmoid ostiomeatal unit sinusitis
ethmoid sinus anatomy osteomeatal complex diagram
ethmoid sinus key sinus chronic sinusitis drainage pathways mucociliary clearance
anterior ethmoid cells infundibulum hiatus semilunaris uncinate process middle turbinate sinusitis mechanism
coronal CT scan ethmoid sinusitis chronic rhinosinusitis osteomeatal complex obstruction
ethmoid sinusitis FESS functional endoscopic sinus surgery Messerklinger Stammberger ethmoid
chronic rhinosinusitis pathogenesis biofilm microbiology inflammatory mediators eosinophils cytokines
Role of the Ethmoid Sinus in the Causation of Chronic Sinusitis
A Comprehensive Review — 50 Marks Answer
1. INTRODUCTION
2. SURGICAL ANATOMY OF THE ETHMOID SINUS
2.1 Overview
| Feature | Details |
|---|---|
| Location | Between nasal cavity (medially) and orbit (laterally) |
| Boundaries | Skull base (superior), orbit (lateral), nasal cavity (medial), sphenoid (posterior), frontal (anterior/superior) |
| Cell count | 3–18 cells per side (average 9) |
| Arterial supply | Anterior & posterior ethmoidal arteries (branches of ophthalmic artery) |
| Venous drainage | Ophthalmic veins → cavernous sinus |
| Nerve supply | Anterior & posterior ethmoidal nerves (V1) |
2.2 Division into Anterior and Posterior Groups
ETHMOID LABYRINTH
│
┌────────────────┴────────────────┐
│ │
ANTERIOR ETHMOID POSTERIOR ETHMOID
(3–15 cells) (1–7 cells)
- Drain into middle meatus - Drain into superior meatus
- Via infundibulum/OMC - Related to optic nerve &
- Related to frontal & sphenoid sinus
maxillary sinus drainage
- KEY AREA FOR CRS
3. THE OSTIOMEATAL COMPLEX (OMC) — THE KEY UNIT
3.1 Definition
┌─────────────────────────────────────────────────────────────┐
│ OSTIOMEATAL COMPLEX (OMC) │
│ │
│ 1. Uncinate Process │
│ 2. Ethmoidal Infundibulum │
│ 3. Hiatus Semilunaris (inferior) │
│ 4. Anterior Ethmoid Air Cells (Agger nasi, Bulla ethmoidalis)│
│ 5. Middle Meatus │
│ 6. Middle Turbinate │
│ 7. Frontal Recess │
│ 8. Ostia of: Maxillary sinus + Frontal sinus │
└─────────────────────────────────────────────────────────────┘
- Anterior ethmoid cells
- Maxillary sinus (via maxillary ostium → infundibulum)
- Frontal sinus (via frontal recess)
4. THE ETHMOID AS THE "KEY SINUS" — ANATOMICAL BASIS
4.1 Central Position
-
Frontal sinus drains via the frontal recess, which is bounded anteriorly and posteriorly by anterior ethmoid cells (agger nasi cell, frontal bulla cell). Any anterior ethmoid disease → frontal outflow obstruction.
-
Maxillary sinus drains via its natural ostium into the ethmoidal infundibulum (a cleft within anterior ethmoid). The infundibulum is bounded:
- Laterally: lamina papyracea
- Medially: uncinate process
- Posteriorly: ethmoidal bulla
-
Sphenoid sinus — while it drains into the sphenoethmoidal recess, posterior ethmoid disease directly abuts the sphenoid and can propagate disease.
-
Posterior ethmoid cells lie adjacent to the optic nerve and carotid artery in the lateral wall — of surgical and complication importance.
FLOWCHART: ETHMOID AS DRAINAGE CONFLUENCE
FRONTAL SINUS
│
▼
FRONTAL RECESS ──────── (Bounded by anterior ethmoid cells)
│
▼
ANTERIOR ETHMOID COMPLEX ────────────────────┐
(Infundibulum / OMC) │
│ │
▼ ▼
MIDDLE MEATUS MAXILLARY SINUS
(Hiatus semilunaris) (Drains via ostium
│ into infundibulum)
▼
NASOPHARYNX / POSTERIOR CHOANA
5. PATHOPHYSIOLOGY: HOW ETHMOID DISEASE CAUSES CHRONIC SINUSITIS
5.1 The Vicious Cycle (Stammberger's Concept)
┌─────────────────────────────────────────────────────────────────────┐
│ STAMMBERGER'S VICIOUS CYCLE OF CHRONIC SINUSITIS │
│ │
│ Viral URTI / Allergy / Anatomic Variant │
│ │ │
│ ▼ │
│ Mucosal Edema in Anterior Ethmoid / OMC │
│ │ │
│ ▼ │
│ Obstruction of Ethmoidal Infundibulum / Frontal Recess │
│ │ │
│ ┌─────────┴──────────┐ │
│ ▼ ▼ │
│ Maxillary sinus Frontal sinus │
│ ostium obstructed recess obstructed │
│ │ │ │
│ ▼ ▼ │
│ Reduced O₂ tension → Anaerobic bacterial growth │
│ Impaired mucociliary clearance │
│ Accumulation of secretions │
│ │ │
│ ▼ │
│ Bacterial infection → Toxins → Further mucosal damage │
│ │ │
│ ▼ │
│ Perpetuation of obstruction → CHRONIC SINUSITIS │
└─────────────────────────────────────────────────────────────────────┘
5.2 Step-by-Step Mechanism
Step 1 — Initiating Event
- Viral upper respiratory infection (commonest)
- Allergic rhinitis
- Environmental irritants (smoke, pollution)
- Anatomical variants (see Section 7)
- Dental infection (for maxillary sinus secondarily)
Step 2 — Ethmoid Mucosal Swelling
Step 3 — Disruption of Mucociliary Clearance (MCC)
- The sinuses depend entirely on ciliary beating for drainage (not gravity).
- Maxillary sinus cilia beat toward the natural ostium → infundibulum → middle meatus.
- Obstruction prevents secretions from exiting → stasis of mucus.
- Stagnant mucus becomes a culture medium.
Step 4 — Hypoxia and Acidosis
- Trapped secretions and increased O₂ consumption create a hypoxic microenvironment.
- pH drops → impairs ciliary function further.
- Creates ideal conditions for anaerobic and facultative anaerobes (Staphylococcus aureus, Pseudomonas aeruginosa, anaerobes).
Step 5 — Bacterial Colonization and Biofilm Formation
- Bacteria form biofilms on sinus mucosa — organized communities resistant to antibiotics and immune defenses.
- S. aureus biofilms detected in up to 33% of CRS patients (Cummings Otolaryngology).
- Biofilm bacteria release superantigens (esp. S. aureus TSST-1) → polyclonal T-cell activation → eosinophilic inflammation.
Step 6 — Chronic Mucosal Inflammation
- Perpetuated by:
- Eosinophils (in CRSwNP — type 2 inflammation: IL-4, IL-5, IL-13, eotaxin)
- Neutrophils (in CRSsNP — type 1/type 17 inflammation: IL-8, TNF-α)
- Mast cells and IgE-mediated responses (in allergic subtypes)
Step 7 — Secondary Sinus Involvement
- Maxillary sinus → retained secretions, mucosal thickening, polyp formation
- Frontal sinus → chronic frontal headache, mucocele risk
- Sphenoid → posterior ethmoid disease spreads posteriorly
- Orbital complications → via lamina papyracea dehiscence
6. ANATOMICAL VARIANTS OF ETHMOID THAT PREDISPOSE TO CRS
6.1 Concha Bullosa
- Pneumatization of the middle turbinate (anterior ethmoid cells extending into turbinate)
- Prevalence: 34–53% of general population
- Mechanism: Enlarges middle turbinate → narrows middle meatus → OMC obstruction
- Quallotine et al. showed worsened QoL and greater surgical improvement in CRS with concha bullosa
- Associated with ipsilateral sinusitis and contralateral septal deviation
6.2 Agger Nasi Cell
- Most anterior ethmoid cell — lies anterior to the lacrimal bone
- Largest/most prominent agger nasi cell → narrows frontal recess → frontal sinusitis
- Langille et al. showed enlarged agger nasi cells correlate with frontal sinus mucosal thickening
6.3 Paradoxical Middle Turbinate
- Turbinate curves laterally instead of medially
- Directly impinges on OMC → recurrent/chronic sinusitis
6.4 Uncinate Process Variations
- Lateralized uncinate process: Narrows infundibulum → impaired maxillary drainage
- Superior attachment variations: Determines whether frontal sinus drains medial or lateral to uncinate (surgical significance)
- Pruna et al. (Surgical Management of CRS, p. 45) studied morphofunctional evaluation of OMC in chronic sinusitis by coronal CT
6.5 Haller Cells (Infraorbital Ethmoid Cells)
- Ethmoid cells that extend into the floor of the orbit / roof of maxillary sinus
- Mechanism: Narrow the infundibulum from its lateral wall → maxillary sinus drainage obstructed
- Prevalence: 10–45%
6.6 Onodi Cells (Sphenoethmoidal Cells)
- Most posterior ethmoid cell that pneumatizes posterosuperiorly, closely related to optic nerve
- Can cause sphenoiditis (Senturk et al., 2017)
- Surgical hazard: optic nerve injury during posterior ethmoidectomy
6.7 Bulla Ethmoidalis Variations
- Prominent bulla → compresses infundibulum → OMC obstruction
- Absent ground lamella → communication between anterior and posterior ethmoid → widespread disease
6.8 Deviated Nasal Septum
- Contralateral to deviation → narrowed middle meatus / OMC
- Fu et al. showed septal deviation associated with recurrent CRS after primary surgery
- Balikci et al. (retrospective 296 cases) confirmed correlation between septal deviation and sinusitis
ANATOMICAL VARIANTS AND THEIR EFFECT ON OMC
VARIANT | MECHANISM | SINUS AFFECTED
---------------------|-------------------------|-------------------
Concha bullosa | Narrows middle meatus | Maxillary, frontal
Agger nasi cell | Narrows frontal recess | Frontal
Haller cell | Narrows infundibulum | Maxillary
Paradoxical MT | Impinges OMC | Multiple
Uncinate lateral. | Narrows infundibulum | Maxillary, frontal
Large ethmoidal bulla| Compresses infundibulum | Maxillary
Onodi cell | Near optic nerve | Sphenoid
DNS (contralateral) | Narrows middle meatus | Ipsilateral
7. CORONAL CT FINDINGS — ETHMOID AND OMC IN CRS
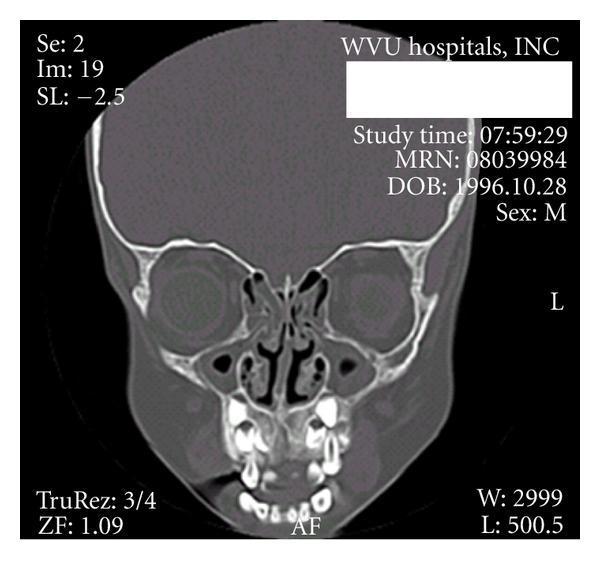

Lund-Mackay CT Scoring (Relevant to Ethmoid Assessment)
| Sinus | Score 0 | Score 1 | Score 2 |
|---|---|---|---|
| Maxillary | No abnormality | Partial opacification | Complete opacification |
| Anterior ethmoid | No abnormality | Partial opacification | Complete opacification |
| Posterior ethmoid | No abnormality | Partial opacification | Complete opacification |
| Frontal | — | — | — |
| Sphenoid | — | — | — |
| OMC | No obstruction (0) | — | Obstructed (2) |
8. ROLE OF ETHMOID IN SPECIFIC TYPES OF CRS
8.1 CRS without Nasal Polyps (CRSsNP)
- Predominantly type 1 / type 17 (Th1/Th17) inflammation
- Driven by bacterial colonization, anatomical obstruction
- Neutrophilic infiltrate
- Anterior ethmoid disease + OMC obstruction predominates
- IL-8, IFN-γ, IL-17 are key cytokines
8.2 CRS with Nasal Polyps (CRSwNP)
- Predominantly type 2 (Th2) eosinophilic inflammation
- IL-4, IL-5, IL-13, eotaxin
- Polyps originate in the ethmoid labyrinth (particularly from the middle meatus and anterior ethmoid clefts)
- Edematous stroma, abundant eosinophils, goblet cell hyperplasia
- Associated with aspirin sensitivity (Samter's triad) and asthma
- Jain et al. showed that CRSwNP is more of a global mucosal disease vs. CRSsNP (more anatomic/ethmoid-limited) — ICAR:RS 2021, p. 141
8.3 Allergic Fungal Rhinosinusitis (AFRS)
- Eosinophilic mucin with non-invasive fungal hyphae
- Characteristically involves ethmoid + unilateral sinus expansion
- High IgE, eosinophilia
- CT: heterogeneous opacification of ethmoid cells with central hyperdense mucin
8.4 Chronic Invasive Fungal Sinusitis
- Per Harrison's (21st Ed., p. 6270): "Chronic invasive sinusitis most commonly affects the ethmoid and sphenoid sinuses" — in immunocompromised patients (diabetes, HIV)
- Bone destruction, orbital apex syndrome, cavernous sinus thrombosis
9. ROLE OF ETHMOID IN COMPLICATIONS OF SINUSITIS
FLOWCHART: ORBITAL COMPLICATIONS FROM ETHMOID SINUSITIS
(Chandler's Classification)
Ethmoid Sinusitis
│
▼
Stage I: Inflammatory Edema (Preseptal/Periorbital cellulitis)
│
▼
Stage II: Orbital Cellulitis (Edema of orbital fat, no abscess)
│
▼
Stage III: Subperiosteal Abscess (Between periorbita & lamina papyracea)
│
▼
Stage IV: Orbital Abscess (Pus within orbital fat)
│
▼
Stage V: Cavernous Sinus Thrombosis
│
▼
DEATH (if untreated)
- Cavernous sinus thrombosis: Ethmoidal veins → ophthalmic vein → cavernous sinus (valveless venous system)
- Meningitis / cerebral abscess: Via anterior ethmoid roof → cribriform plate → anterior cranial fossa
- Mucocele: Chronic frontal-ethmoid mucocele from OMC obstruction — commonest type
10. MUCOCILIARY CLEARANCE AND THE ETHMOID
Normal Mucociliary Transport in Sinuses
MAXILLARY SINUS:
Cilia beat from floor → walls → natural ostium
→ ETHMOIDAL INFUNDIBULUM → MIDDLE MEATUS → NASOPHARYNX
FRONTAL SINUS:
Medial wall (descending) → FRONTAL RECESS
→ ANTERIOR ETHMOID → MIDDLE MEATUS → NASOPHARYNX
ANTERIOR ETHMOID:
→ HIATUS SEMILUNARIS → MIDDLE MEATUS
POSTERIOR ETHMOID:
→ SUPERIOR MEATUS → NASOPHARYNX
Ciliary Beat Frequency (CBF) in CRS
- Normal: 11–15 Hz
- Reduced to 6–9 Hz in CRS (due to inflammation, bacterial toxins, hypoxia)
- Further reduced by: cigarette smoke, low temperature, viral infections
- Restoration after FESS has been demonstrated within 3–6 months
11. MICROBIOLOGY AND THE ETHMOID
Acute-on-Chronic Exacerbations
- Streptococcus pneumoniae (most common in acute exacerbations)
- Haemophilus influenzae
- Moraxella catarrhalis
Chronic Disease (Ethmoid mucosa)
- Staphylococcus aureus (including MRSA)
- Pseudomonas aeruginosa
- Anaerobes: Prevotella, Fusobacterium, Peptostreptococcus
- Fungi: Aspergillus fumigatus, Bipolaris, Alternaria
Biofilm (Critical for Chronicity)
- Ethmoid surfaces harbor biofilm communities
- Biofilm detected in >50% of CRS patients undergoing revision surgery
- Protected from antibiotics by exopolysaccharide matrix (100–1000× more antibiotic concentration needed)
- Triggers sustained innate immune activation → perpetuates inflammation
12. THE CONCEPT OF "ETHMOID SINUSITIS AS PRIMARY" — HISTORICAL PERSPECTIVE
Pre-FESS Era (Intranasal Antrostomy Period)
- Focus was on maxillary sinus (antrum)
- Intranasal antrostomy, Caldwell-Luc operation
- Results were poor — recurrence common
- Reason: Ethmoid disease was not addressed
Messerklinger-Stammberger Revolution (1970s–1980s)
- Karl Messerklinger (Graz, Austria) demonstrated via endoscopy that mucociliary flow from maxillary sinus converges at the ethmoid infundibulum
- Heinz Stammberger popularized the OMC concept and FESS
- Demonstrated that targeted anterior ethmoidectomy + OMC clearance cures downstream maxillary and frontal sinusitis without touching those sinuses directly
- This is the basis of FESS in Scott-Brown, Cummings, and all modern ENT texts
Kennedy's Contribution (Johns Hopkins, 1985)
- Coined the term "FESS" in English literature
- Established CT coronal sinus protocols
- Confirmed ethmoid as the primary target
13. SURGICAL IMPLICATIONS — FESS AND THE ETHMOID
Principles of FESS (Based on Ethmoid Pathophysiology)
- Remove diseased ethmoid cells → restore OMC patency
- Anterior ethmoidectomy — open anterior ethmoid cells, remove uncinate process, open infundibulum
- Posterior ethmoidectomy — when posterior disease present
- Frontal sinusotomy — address frontal recess disease (Draf I/II/III)
- Maxillary antrostomy — middle meatal antrostomy (not inferior — to preserve MCC toward natural ostium)
Extent of Surgery
- Ramkumar et al. (Surgical Management of CRS, p. 45) — systematic review: no significant difference in outcomes between limited vs. extensive ESS when OMC is adequately addressed
- Masterson et al. showed extensive ESS reduces revision rates in nasal polyposis
Revision Surgery
- Most common cause of failure: residual ethmoid disease
- Incomplete anterior ethmoidectomy → persistent OMC obstruction → recurrence
- Simmonds et al. (5-year data, Surgical Management CRS, p. 45): ESS provides sustained improvement in SNOT-22 scores
14. RECENT ADVANCES (2015–2024)
14.1 Endotype-Based Classification of CRS
- Traditional phenotype (polyp/no polyp) replaced by endotypes based on underlying immunopathology:
- Type 2 CRS (eosinophilic, atopic): Responds to biologics
- Type 1/Type 17 CRS (neutrophilic): More antibiotic/surgical approach
- Ethmoid tissue biopsy now guides biological therapy selection
14.2 Biologics for CRS — Ethmoid Disease as Target
- Dupilumab (IL-4Rα blocker): FDA approved 2019 for CRSwNP; shown to reduce ethmoid opacification on CT
- Omalizumab (anti-IgE): Phase III data (POLYP 1&2 trials); reduces nasal polyp (ethmoid origin) burden
- Mepolizumab (anti-IL-5): Reduces eosinophilic ethmoid polyposis
- ICAR:RS 2021 strongly endorses these for refractory CRSwNP
14.3 Microbiome and Dysbiosis
- Healthy ethmoid/sinus microbiome dominated by Lactobacillus, Staphylococcus epidermidis
- CRS shows dysbiosis → S. aureus, Pseudomonas dominance
- Loss of Lactobacillaceae → reduced bacteriocin production → pathogen overgrowth
- Potential for probiotic therapy for CRS
14.4 Epithelial Barrier Dysfunction
- CRS patients show defective tight junctions (claudin, occludin) in ethmoid epithelium
- Increases mucosal permeability → antigen penetration → amplified immune response
- IL-33, TSLP (thymic stromal lymphopoietin) released from damaged epithelium → type 2 skew
14.5 Staphylococcal Superantigens and IgE
- S. aureus colonizing ethmoid mucosa releases superantigens (SEA, SEB, TSST-1)
- Polyclonal IgE production in ethmoid tissue
- Total IgE levels correlate with ethmoid disease severity and polyp recurrence
14.6 Image-Guided Surgery (Navigation)
- CT-based intraoperative navigation now standard for complex ethmoid dissection
- Reduces orbital and skull base complications
- Essential when ground lamella is absent or anatomy is distorted
14.7 Drug-Eluting Implants
- PROPEL (mometasone furoate-eluting stent) placed in ethmoid cavity post-FESS
- Reduces postoperative inflammation, adhesions, and polyp recurrence
- FDA approved; shown to reduce need for revision ethmoidectomy
14.8 Balloon Sinuplasty vs. FESS for Ethmoid Disease
- Balloon sinuplasty: Limited role for ethmoid — cannot address diseased ethmoid cells
- FESS remains gold standard for ethmoid CRS
- Hybrid approaches: balloon for maxillary/frontal + FESS for ethmoid
15. COMPREHENSIVE FLOW CHART — ETHMOID IN CRS CAUSATION
╔══════════════════════════════════════════════════════════════════════════════╗
║ ROLE OF ETHMOID SINUS IN CAUSATION OF CHRONIC SINUSITIS ║
╚══════════════════════════════════════════════════════════════════════════════╝
PREDISPOSING FACTORS
│
├── Viral URTI
├── Allergic Rhinitis (Atopy)
├── Environmental Pollutants
├── Anatomical Variants (concha bullosa, agger nasi, Haller cell, etc.)
├── Immunodeficiency (IgA def., CVID)
├── Mucociliary Dyskinesia (Kartagener's, CF)
└── Dental sepsis (→ maxillary)
│
▼
MUCOSAL EDEMA IN NARROW ETHMOID CLEFTS
(Infundibulum width 1–2 mm → minimal swelling → complete block)
│
▼
OMC OBSTRUCTION
(Anterior ethmoid / Infundibulum / Frontal Recess)
│
┌─────┴──────────────────────────────────────────┐
│ │
▼ ▼
MAXILLARY OSTIUM BLOCKED FRONTAL RECESS BLOCKED
(Maxillary sinus drainage impaired) (Frontal sinus drainage impaired)
│ │
└──────────────────┬──────────────────────────────┘
│
▼
STASIS OF SECRETIONS IN ETHMOID + DEPENDENT SINUSES
│
▼
HYPOXIA + ACIDOSIS IN SINUS CAVITIES
│
▼
REDUCED CILIARY BEAT FREQUENCY (11→6 Hz)
│
▼
BACTERIAL COLONIZATION
(S. aureus, Pseudomonas, anaerobes)
│
▼
BIOFILM FORMATION (on ethmoid mucosa)
↓ Antibiotic penetration (100–1000× resistance)
↓ Immune evasion
↓ Superantigen release (TSST-1)
│
▼
CHRONIC MUCOSAL INFLAMMATION
┌──────────────┴────────────────┐
│ │
CRSsNP CRSwNP
(Th1/Th17) (Th2)
Neutrophilic Eosinophilic
IL-8, IL-17, IFN-γ IL-4, IL-5, IL-13
│ │
▼ ▼
Mucosal thickening Nasal polyps
(ethmoid, maxillary) (originate in ethmoid)
│
▼
STRUCTURAL CHANGES
Mucosal fibrosis, goblet cell hyperplasia,
bony erosion, mucocele formation
│
▼
CHRONIC SINUSITIS ESTABLISHED
(Duration > 12 weeks, ± exacerbations)
16. SUMMARY TABLE — TEXTBOOK PERSPECTIVES
| Textbook | Key Contribution on Ethmoid in CRS |
|---|---|
| Scott-Brown's Otorhinolaryngology (8th Ed.) | Detailed anatomy of OMC, Messerklinger-Stammberger doctrine, FESS rationale |
| Cummings Otolaryngology (7th Ed.) | Inflammatory endotypes, biofilm, biologic therapy, FESS outcomes |
| Stell & Maran's Head and Neck Surgery | Surgical anatomy of ethmoid, orbital complications, anatomical variations |
| Zakir Hussain's ENT | OMC concept in South Asian context, mucociliary recirculation, exam-oriented summary |
| Dhingra's Diseases of ENT (7th Ed.) | Ethmoid as key sinus, Chandler's classification, MCC physiology |
| Hazarika's Textbook of ENT | Endoscopic anatomy, FESS technique, ethmoid and complications |
| Harrison's Internal Medicine (21st Ed., p. 6270) | Chronic invasive ethmoid/sphenoid sinusitis in immunocompromised |
| ICAR:RS 2021 | Comprehensive evidence-based review: OMC variants, endotypes, biologics, surgery outcomes |
17. CONCLUSION
-
Anatomically central: All other paranasal sinuses (frontal, maxillary, and to a lesser extent, sphenoid) drain through or adjacent to the ethmoid complex.
-
The OMC is the rate-limiting step: The narrow anterior ethmoid clefts — the infundibulum, frontal recess, and hiatus semilunaris — are the first to become obstructed with even mild mucosal swelling.
-
Primary disease propagator: Ethmoid disease initiates and perpetuates maxillary and frontal sinusitis via the vicious cycle of obstruction → stasis → infection → further mucosal damage.
-
Anatomical variants amplify risk: Concha bullosa, agger nasi cells, Haller cells, and uncinate variations predominantly affect ethmoid drainage and are strongly associated with limited CRS.
-
Surgical target: FESS targeting the ethmoid (anterior ethmoidectomy, OMC clearance) resolves downstream sinus disease without directly instrumenting the maxillary or frontal sinus in many cases — the ultimate proof of the ethmoid's primacy.
-
Modern biological targets originate in ethmoid tissue: Nasal polyps begin in the ethmoid; eosinophilic inflammation peaks in ethmoid mucosa; S. aureus biofilms colonize ethmoid surfaces.
References
- Stammberger H. Functional Endoscopic Sinus Surgery. Philadelphia: B.C. Decker, 1991.
- Kennedy DW et al. Functional Endoscopic Sinus Surgery. Arch Otolaryngol. 1985;111:576–582.
- Fokkens WJ et al. EPOS 2020: European Position Paper on Rhinosinusitis and Nasal Polyps. Rhinology. 2020;58(Suppl 29):1–464.
- Orlandi RR et al. ICAR:RS 2021. Int Forum Allergy Rhinol. 2021;11(3):213–739. [pp. 52, 141, 471 cited above]
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th Ed., Watkinson & Clarke, 2018.
- Cummings Otolaryngology Head and Neck Surgery, 7th Ed., Flint et al., Elsevier, 2021.
- Stell & Maran's Head and Neck Surgery, 5th Ed., Mackay & Rhys Evans, 2012.
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat, 7th Ed., Elsevier India, 2018.
- Hazarika P et al. Textbook of ENT and Head & Neck Surgery, 3rd Ed., CBS Publishers, 2009.
- Zakir Hussain. ENT for Undergraduates. Jaypee Brothers, 2020.
- Harrison's Principles of Internal Medicine, 21st Ed., p. 6270. McGraw-Hill, 2022.
- Bhattacharyya N. Eosinophilia in chronic rhinosinusitis. Laryngoscope. 2002.
- Gwaltney JM et al. CT scanning in rhinosinusitis. Arch Otolaryngol. 1994.
- Van Crombruggen K et al. Inflammatory markers in CRS. Allergy. 2011.
- Jain R et al. Anatomical variants in limited vs. diffuse CRS. Auris Nasus Larynx. 2017.
- Ramkumar SP et al. Limited vs. extensive ESS outcomes. Int Forum Allergy Rhinol. 2023;13:2096–2100.
- Bachert C et al. Dupilumab in CRS with nasal polyps. NEJM. 2019;380:1638–1650.
- Simmonds JC et al. ESS 5-year outcomes. Int Forum Allergy Rhinol. 2022;12(3):257–265.