Recent advances in snoring surgery in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
snoring surgery treatment advances
Searching the Web
recent advances snoring surgery RGUHS ENT 2024 2025 UPPP palatal implants drug-induced sleep endoscopy
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
hypoglossal nerve stimulation OSA surgery
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
RECENT ADVANCES IN SNORING SURGERY
RGUHS Standard Answer - 20 Marks
Sources: Scott-Brown's Otolaryngology, Cummings Otolaryngology, Murray & Nadel, Dhingra, Hazarika, Zakir Hussain | Recent PubMed Evidence 2023-2026
INTRODUCTION
Snoring occurs due to vibration of the soft palate, uvula, pharyngeal walls, tongue base, and epiglottis during sleep. It may represent simple primary snoring or may be part of Obstructive Sleep Apnea Syndrome (OSAS). Surgical treatment aims to correct upper airway obstruction, which may require intervention at multiple levels - from nasal to hypopharyngeal.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, pp. 1118-1121
PREOPERATIVE EVALUATION FLOWCHART
PATIENT WITH SNORING
|
v
HISTORY + CLINICAL EXAMINATION
(BMI, Mallampati, tonsil size, nasal patency)
|
v
SLEEP STUDY (Polysomnography / Home Sleep Test)
|
_____|_____
| |
AHI < 5 AHI 5-30 AHI > 30
(Primary (Mild-Moderate (Severe OSAS)
Snoring) OSAS)
| | |
v v v
Site- CPAP trial CPAP first-line +
specific +/- surgery Surgery if CPAP
surgery fails/refused
|
v
DRUG-INDUCED SLEEP ENDOSCOPY (DISE)
(Identify level of collapse: VOTE Classification)
|
_____|________________________
| | | |
Velum Oropharynx Tongue Epiglottis
(Palate) (Tonsils) Base
| | | |
Palatal Tonsillect/ Tongue base Partial
surgery UPPP/ESP surgery epiglottidectomy
DRUG-INDUCED SLEEP ENDOSCOPY (DISE)
DISE (Drug-Induced Sleep Endoscopy) is a cornerstone preoperative procedure that identifies the site and pattern of upper airway collapse using propofol or dexmedetomidine sedation to simulate sleep. The VOTE classification grades collapse at four sites:
- V - Velum (palate/uvula)
- O - Oropharynx (lateral walls/tonsils)
- T - Tongue base
- E - Epiglottis
Collapse pattern guides procedure selection. Concentric retropalatal collapse is a contraindication to hypoglossal nerve stimulation (HNS) but can be converted to AP collapse by palatopharyngoplasty, then making the patient eligible for HNS. - Murray & Nadel, p. 2707
CLASSIFICATION OF SURGICAL APPROACHES
SURGERY FOR SNORING / OSAS
|
_______|_______________________
| | |
LEVEL 1 LEVEL 2 LEVEL 3
(Nasal) (Palatal/ (Tongue base/
Oropharyngeal) Hypopharyngeal/
Skeletal)
| | |
Septoplasty UPPP Tongue base RF
Turbinate LAUP TORS
reduction CAPSO Genioglossus adv.
Nasal valve RF/Coblation Hyoid suspension
repair ESP MMA
Palatal HNS (Inspire)
implants
A. NASAL SURGERY
Nasal obstruction (deviated septum, polyps, nasal valve collapse) increases upper airway resistance and worsens snoring. Procedures include:
- Septoplasty
- Inferior turbinate reduction
- Nasal valve repair (spreader grafts, alar batten grafts)
Key point: Nasal surgery alone does NOT significantly improve AHI or snoring intensity, but reduces CPAP pressure requirements and improves compliance. A study of 40 patients showed objective improvement in nasal airway (rhinomanometry) without change in snoring time or intensity. - Scott-Brown's, p. 1118
B. PALATAL / OROPHARYNGEAL SURGERY
1. Uvulopalatopharyngoplasty (UPPP)
Original Fujita Technique (1981): Excision of the uvula, removal of 1-2 cm of oral palatal mucosa in curvilinear fashion along anterior pillars, excision of excess soft palate, and anterolateral advancement of nasopharyngeal mucosa to widen the nasopharyngeal airway.
Simmons Modification (UK): Excision of tonsils, uvula, half of anterior and posterior pillars, and full-thickness lower soft palate, with closure pulling the cut edges together.
Outcomes:
- Short-term success rate: ~50-60% (AHI reduction >50%)
- Complications: velopharyngeal insufficiency, nasopharyngeal stenosis, voice change, dry throat, post-op hemorrhage
- UPPP may compromise nasal CPAP therapy if VPI occurs
- Scott-Brown's Otorhinolaryngology, pp. 8992-9010; Cummings Otolaryngology
2. Expansion Sphincter Pharyngoplasty (ESP)
A modification of UPPP that specifically addresses lateral pharyngeal wall collapse by rotating the palatopharyngeus muscle superolaterally and suturing it to the pterygomandibular raphe, creating a stent-like effect. Preferred for lateral wall collapse on DISE. Better outcomes than traditional UPPP for selected patients.
3. Laser-Assisted Uvulopalatoplasty (LAUP)
Described by Kamami (1990) using CO2 laser:
- Creates vertical trenches up to 2 cm on either side of the uvula
- Partial vaporization of the uvula
- Multiple modifications described using CO2 or Nd-YAG laser
- Aim: scarring and stiffening of soft palate to reduce palatal flutter
Outcomes:
- Short-term success: 79%; drops to 55% long-term
- Post-op pain worse than UPPP (peaks day 3, resolves ~day 15)
- Complications: hemorrhage (2.12%), temporary palatal incompetence (0.53%), loss of taste (0.27%), globus symptoms
- Risk: Some simple snorers developed mild OSA following LAUP due to palatal fibrosis contracting the velopharyngeal space
- Scott-Brown's, p. 1119
4. Radiofrequency Tissue Reduction / Coblation (CAUP)
Mechanism: Low-frequency radio waves delivered submucosal via a wand create charged ions heating tissue to 60-90°C, causing protein denaturation and cell lysis with minimal collateral damage. This induces scarring, reduces tissue volume, and stiffens the palate.
Devices available: Somnus unit, Celon device (bipolar), Coblator unit
Coblation Assisted Upper Airway Procedure (CAUP) - Tvinnereim:
- Lateral palatal incision on each side
- Ablation of 3 upward fan-shaped channels on each side of midline
- Partial uvulectomy with 2 upward channels
- Channelling of anterior/posterior pillars
- Can be applied at tongue base simultaneously
- Multilevel therapy: 33% improvement in OSA patients
- Long-term success rate: 37%
Advantages: Can be performed under local anesthesia at multiple levels
Complications: Hemorrhage, infection, velopharyngeal fistula (rare); tongue base - abscesses 0-8%, tongue neuralgias
- Scott-Brown's, pp. 9088-9127
5. Cautery-Assisted Palatal Stiffening Operation (CAPSO)
Uses electrocautery needle to remove a 2 cm inverted 'U' area of mucosa from soft palate plus mucosa and part of uvula. Heals by secondary intention to stiffen the soft palate. Performed under local anesthesia.
6. Palatal Implants (Pillar Procedure)
Three braided polyester implants are inserted into the submucosal layer of the soft palate under local anesthesia in an office setting. They induce a fibrotic reaction that stiffens the soft palate. Minimal morbidity; most suitable for primary snoring and mild OSA.
7. Tonsillectomy and Adenoidectomy
- Children: Most effective surgery; adenotonsillectomy is first-line for pediatric OSAS
- Adults: When tonsils are enlarged (Friedman grade 3-4), tonsillectomy combined with UPPP significantly improves outcomes
C. TONGUE BASE AND HYPOPHARYNGEAL SURGERY
1. Radiofrequency Tongue Base Reduction
Radiofrequency probe inserted at multiple sites into the tongue base submucosal tissue under GA or LA. Multiple treatment sessions may be needed. Success rate: moderate; complications include tongue abscess (0-8%), neuralgias.
2. Genioglossus Advancement
A rectangular window osteotomy is made in the mandibular symphysis around the genial tubercle. The segment is advanced anteriorly and rotated 90 degrees to prevent retraction, effectively pulling the tongue base anteriorly. Combined with hyoid suspension in Phase I surgery.
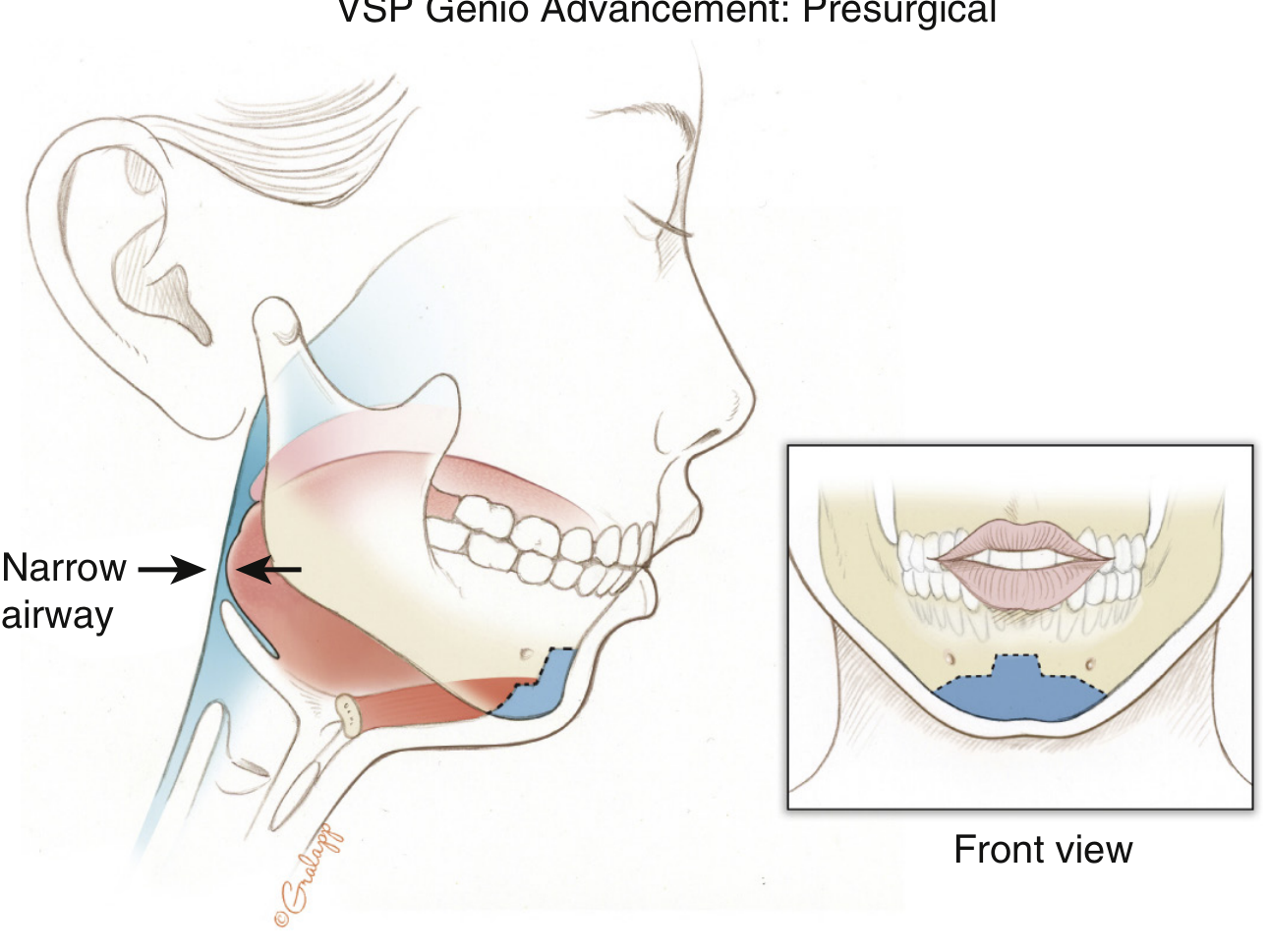
Figure: Genioglossus advancement (Virtual Surgical Planning). The genial segment is advanced to widen the hypopharyngeal airway. (Murray & Nadel, Fig. 122.7)
3. Hyoid Suspension
The hyoid bone is advanced anteriorly and attached to the mandible or thyroid cartilage by permanent sutures. This suspends the tongue base and epiglottis anteriorly, enlarging the retrolingual and retroepiglottic space.
4. Tongue Base Suspension (Repose System)
A permanent suture is passed from a bone screw in the mandibular symphysis to the base of the tongue, suspending it anteriorly to prevent retrolingual collapse.
5. Transoral Robotic Surgery (TORS) - Recent Advance
Minimally invasive telerobotic system providing:
- Excellent 3D visualization
- Immaculate precision and absence of tremor
- Access to tongue base for reduction and treatment of floppy epiglottis
Outcomes: Vicini et al. - PSG success rate (post-op AHI <15) ~80% at 3 years. TORS is typically combined with multilevel surgery (septoplasty, UPPP, supraglottoplasty).
- Scott-Brown's, pp. 9152-9175
6. Lingual Tonsillectomy
Removal of hypertrophied lingual tonsil tissue at tongue base via direct or robotic approach. Particularly effective when DISE reveals tongue base collapse due to lingual tonsillar hypertrophy.
7. Epiglottoplasty / Partial Epiglottidectomy
Performed for epiglottic collapse identified on DISE. Reduces the omega-shaped epiglottis. Can be performed transorally or via TORS.
D. SKELETAL / FRAMEWORK SURGERY
1. Maxillomandibular Advancement (MMA)
The upper and lower jaws (maxilla + mandible) are surgically advanced 10-12 mm via Le Fort I osteotomy (maxilla) and bilateral sagittal split osteotomy (BSSO) of mandible. This pulls all attached soft tissue anteriorly, greatly enlarging the entire upper airway from nose to hypopharynx.
Outcomes:
- Most effective surgical treatment for severe OSA
- Success rate 85-95% (AHI reduction >50%)
- Indicated when multilevel soft tissue surgery has failed
Key point from Murray & Nadel: Treatment selection depends on patient preference and candidacy - patients may proceed to soft tissue surgery (nose, soft palate, tongue) or directly to skeletal MMA depending on OSA severity. - Murray & Nadel, p. 2755
2. Maxillary Expansion / Rapid Palatal Expansion
Used in patients with narrow maxilla and transverse deficiency causing nasal obstruction. Expands the nasal floor and reduces nasal resistance.
E. RECENT ADVANCES (2022-2026)
1. Hypoglossal Nerve Stimulation (HNS) - Inspire Therapy
The most significant recent advance in OSA surgery.
FDA approved in 2014; rapidly expanding indications.
Mechanism: The hypoglossal nerve (CN XII) innervates tongue protrusor (genioglossus) and retrusor muscles through medial and lateral divisions. Selective stimulation of the medial branches (protrusors) causes anterior tongue movement, increasing airflow during sleep.
System components:
- Implantable pulse generator (IPG) - placed in infraclavicular region
- Stimulation lead - cuff electrode around medial branches of hypoglossal nerve
- Sensing lead - placed between intercostal muscles to detect respiratory effort
- Handheld remote for patient activation/deactivation
The IPG detects end of expiration via the sensing lead and then activates tongue protrusion synchronized with inspiration.
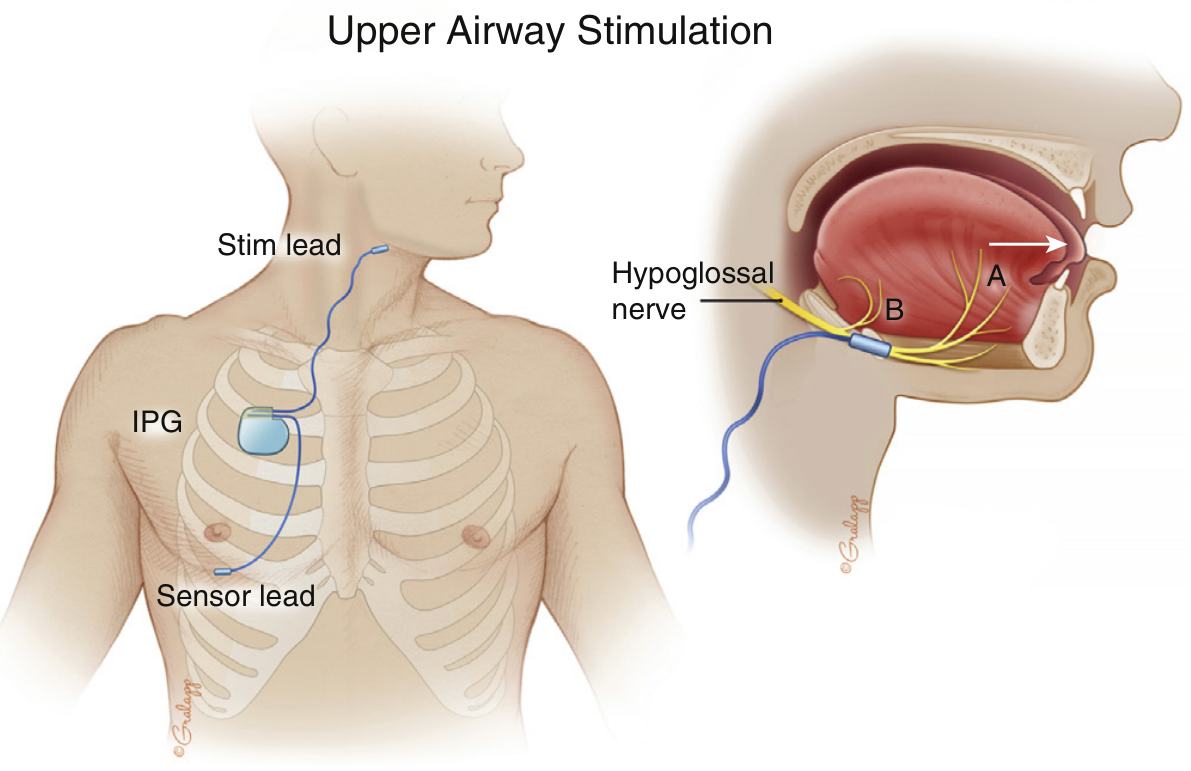
Figure: Hypoglossal nerve stimulation (Inspire device). The IPG is implanted subcutaneously in the chest; a sensing lead detects respiratory effort; a stimulation lead activates tongue protrusor muscles via selective hypoglossal nerve stimulation. (Murray & Nadel, Fig. 122.8)
STAR Trial (Pivotal trial): Significant decrease in OSA symptoms and AHI at 6 months post-implantation.
Patient selection criteria:
- CPAP intolerant/failed
- AHI 15-65 events/hour
- BMI ≤ 40 kg/m² (now expanded to ≤ 40 per 2024 guidelines)
- No concentric retropalatal collapse on DISE (A/P collapse acceptable)
- Absence of complete concentric palatal collapse
Recent meta-analysis (PMID: 37354340): Patient-reported outcomes with HNS show significant improvement in ESS, snoring, and quality of life. Kim et al. meta-analysis (PMID: 37661785) confirmed comparative superiority over alternative surgical treatments for moderate-severe OSA.
New devices: Genio (unilateral hypoglossal stimulation without sensing lead), LivaNova (bilateral stimulation), Ansa cervicalis stimulation.
- Murray & Nadel, pp. 2723-2727; Scott-Brown's, pp. 9270-9272
2. Palatal Hybrid Surgery
Combines UPPP with mini-invasive techniques including push-pull maneuver of palatopharyngeus and palatoglossus muscles, creating a 3D stereoscopic structure in the tonsillar fossa to prevent posterior tongue displacement. Shows 70% reduction in VAS snoring scores. - Biomedical Journal, 2023
3. Modified Barbed Soft Palate Posterior Pillar Flap Palatopharyngoplasty
Single-stage procedure combining DISE with nasal surgery and barbed suture palatopharyngoplasty to address multiple levels simultaneously, reducing surgical morbidity and number of procedures.
4. Drug-Induced Sleep Endoscopy Guided Personalized Surgery
Rather than a standardized approach, DISE-guided tailored multilevel surgery is now the paradigm. Single-stage DISE + nasal surgery + palatopharyngoplasty has been described with excellent AHI improvement (from 8.9 ± 1.3 to 1.11 ± 0.2).
5. ExciteOSA (Neuromuscular Electrical Stimulation)
A daytime neuromuscular electrical stimulation device worn in the mouth for 20 minutes/day to strengthen tongue musculature, reducing nocturnal pharyngeal collapse. Non-invasive; emerging evidence (2024).
6. GLP-1 Agonists as Adjunct
Recent evidence (2024-2025) shows that GLP-1 receptor agonists (semaglutide, tirzepatide) cause significant weight loss and independently reduce OSA severity, potentially reducing the need for surgery in obese patients. AHA/ASA 2024 incorporated GLP-1 therapy alongside surgical options.
7. Role of Nasal Surgery (Recent Systematic Review 2024)
Correa et al. (PMID: 39268344) - systematic review confirming nasal surgery alone does not consistently reduce AHI but remains important as adjunct surgery to improve CPAP compliance and as part of multilevel treatment.
RUSH SLEEP SURGERY ALGORITHM (2024) - Flowchart
Sleep Study Review + H&P + Supine Nasolaryngoscopy
|
Positional OSA? → Yes → Positional Therapy Trial
| No
v
Non-focal Examination
|
BMI > 40? → Yes → Bariatrics Referral
| No
v
Drug-Induced Sleep Endoscopy (DISE)
|
________________|_______________________________
| | | |
Soft Palate Lateral Wall Tongue Base Epiglottic
Collapse Collapse Collapse Obstruction
| | | |
Palatopharyn- Oral Appliance HNS Oral Appliance
goplasty /HNS MMA Lingual Cervical Pillow
Palatopharyn- Tonsillectomy Partial
goplasty Genioglossus Epiglottidectomy
Advancement Hyoid Suspension
Maxillary Exp.
(Source: Rush University Sleep Surgery Algorithm, 2024)
RILEY-POWELL-STANFORD PROTOCOL (Phase I / Phase II Surgery)
PHASE I SURGERY (Soft Tissue - First Line)
Nasal surgery + UPPP + Genioglossus Adv. + Hyoid Suspension
|
Response?
/ \
Yes No
| |
Continue PHASE II SURGERY
(Skeletal - Second Line)
Maxillomandibular
Advancement (MMA)
FRIEDMAN STAGING SYSTEM (Patient Selection for UPPP)
Friedman Tongue Position (FTP) + Tonsil Size (1-4) + BMI
| |
v v
STAGE I: FTP 1-2, Tonsils 3-4 → UPPP success ~80%
STAGE II: FTP 1-2, Tonsils 1-2 OR FTP 3-4, Tonsils 3-4 → ~40%
STAGE III: FTP 3-4, Tonsils 1-2 → <8% success with UPPP alone
PEDIATRIC CONSIDERATIONS (Cummings)
In children, the primary surgical options are:
- Adenotonsillectomy - first line (most effective)
- Lingual tonsillectomy, supraglottoplasty, UPPP, genioglossus advancement, mandibular distraction, HNS (in Down syndrome) for persistent SDB after adenotonsillectomy
Recent advance: HNS (Inspire) now approved for adolescents with Down syndrome and persistent OSA refractory to adenotonsillectomy. - Cummings, block41, p. 3230; PMID: 38062678
COMPLICATIONS OF SNORING SURGERY
| Procedure | Major Complications |
|---|---|
| UPPP | VPI, nasopharyngeal stenosis, voice change, dry throat |
| LAUP | Mild OSA induction, palatal fibrosis, globus |
| RF/Coblation | Hemorrhage, infection, VPF (rare) |
| Genioglossus adv. | Tooth root injury, chin numbness, dehiscence |
| MMA | Malocclusion, nerve injury, relapse |
| HNS | Device infection, lead migration, tongue abrasion |
| TORS | Airway edema, hemorrhage, aspiration |
KEY POINTS (RGUHS Exam Summary)
- DISE is the standard preoperative investigation to guide site-specific surgery
- UPPP (Fujita 1981) remains the most commonly performed palatal surgery; success ~50-60%
- Radiofrequency/Coblation - minimally invasive, outpatient, multilevel application
- LAUP - can paradoxically worsen OSA; falling out of favor
- CAPSO - office procedure under LA; palatal stiffening
- Palatal implants - best for primary snoring, mild OSA
- HNS (Inspire) - most significant recent advance; FDA approved 2014; BMI ≤ 40; contraindicated in concentric palatal collapse
- MMA - gold standard surgical cure rate (85-95%); reserved for severe/failed cases
- TORS - tongue base reduction via robot; multilevel surgery; ~80% PSG success
- Multilevel surgery is required in most cases; single-level surgery often insufficient
- GLP-1 agonists + HNS represent the current frontier in 2024-2026
- Treatment is always multidisciplinary - lifestyle modification, CPAP, dental appliances, then surgery
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Ed., pp. 1117-1121
- Cummings Otolaryngology Head & Neck Surgery, 7th Ed., pp. 3230-3233
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Vol., pp. 2604-2763
- Dhingra P.L. - Diseases of Ear, Nose & Throat
- Hazarika P. - Textbook of ENT & Head-Neck Surgery
- Zakir Hussain - Clinical ENT
- Braun M et al. HNS patient-reported outcomes meta-analysis. Eur Arch Otorhinolaryngol 2023
- Kim DH et al. HNS vs. alternatives systematic review. J Sleep Res 2024
- Rodriguez Lara F et al. HNS in Down Syndrome. Ann Otol Rhinol Laryngol 2024
- Correa EJ et al. Nasal surgery in OSA systematic review. Sleep Sci 2024
RGUHS Exam Tip: This is a 20-mark question typically requiring: Introduction (2M) + Classification of surgical procedures (3M) + Individual procedures with details (8M) + Recent advances esp. HNS, TORS, DISE, ESP (5M) + Complications + Conclusion (2M). Draw at least one diagram of UPPP technique and one flowchart of surgical decision-making.
This is a shared conversation. Sign in to Orris to start your own chat.