Pruritis in third trimester of pregnancy with normal LFT
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pruritus pregnancy" AND "intrahepatic cholestasis"
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have excellent, comprehensive content. Let me compile the full answer.
Pruritus in Third Trimester of Pregnancy with Normal LFTs
Diagnostic Algorithm
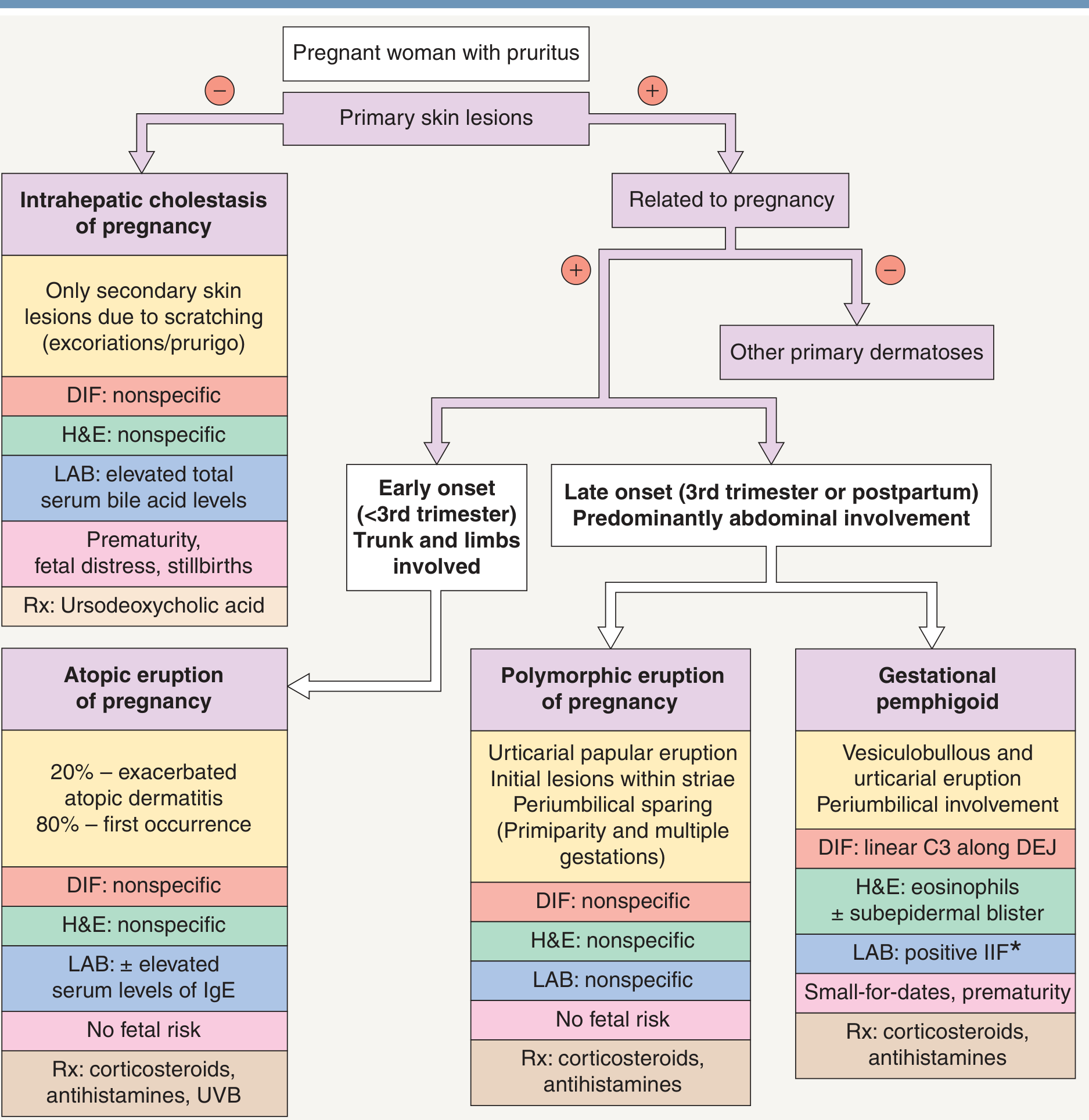
Dermatology 2-Volume Set 5e, Fig. 27.10
Overview
Approximately 20% of pregnant women experience pruritus. The key first step when evaluating pruritus in pregnancy is asking: Are primary skin lesions present?
- No primary lesions (only excoriations from scratching) → Think Intrahepatic Cholestasis of Pregnancy (ICP), but...
- With primary skin lesions in the third trimester → Consider PEP/PUPPP, Gestational Pemphigoid, or AEP
The Critical Point: Normal LFTs Does NOT Rule Out ICP
This is clinically important and frequently tested:
"Pruritus can precede abnormal findings of liver function tests or total serum bile acids, and follow-up testing for obstetric cholestasis may be needed for itchy pregnant patients with initially normal findings."
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1716
"Cholestatic itching correlates better with elevated serum bile acid levels than with the results of other biochemical liver function tests such as alkaline phosphatase, AST, ALT, and bilirubin."
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1716
So in ICP, serum bile acids rise first - standard LFTs (ALT, AST, ALP, bilirubin) may be initially normal. The appropriate test is fasting serum bile acids (>10 µmol/L is diagnostic for ICP).
Differential Diagnosis: Pruritic Conditions in Third Trimester
| Condition | Skin Lesions | LFTs/Labs | Fetal Risk | Trimester |
|---|---|---|---|---|
| ICP (Intrahepatic Cholestasis of Pregnancy) | No primary lesions; only excoriations | Bile acids elevated; LFTs may be normal early | Yes - prematurity, fetal distress, stillbirth | 2nd-3rd |
| PEP / PUPPP | Urticarial papules/plaques in striae, periumbilical sparing | Normal | None | 3rd trimester |
| Gestational Pemphigoid | Vesiculobullous + urticarial; periumbilical involvement | DIF: linear C3 at DEJ | Small-for-dates, prematurity | 2nd-3rd / postpartum |
| Atopic Eruption of Pregnancy (AEP) | Eczematous/papular, trunk and extremities | ± elevated IgE | None | Mostly < 3rd trimester |
| Pruritus Gravidarum (benign) | None | Normal (no cholestasis) | None | 3rd trimester |
1. Intrahepatic Cholestasis of Pregnancy (ICP)
- Occurs in 1.5-2% of pregnant women
- Presents with generalized pruritus without rash, worse on palms and soles, worse at night
- Jaundice in only 0.02% of pregnancies
- Key diagnostic test: fasting serum bile acids (>10 µmol/L = ICP; >40 µmol/L = severe ICP with higher fetal risk)
- LFTs lag behind bile acid elevation - always order bile acids even with normal LFTs
- Resolves within 2 weeks of delivery; recurs in ~50% of subsequent pregnancies
- Treatment: Ursodeoxycholic acid (UDCA) - reduces pruritus and improves fetal outcomes
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1716
2. Polymorphic Eruption of Pregnancy (PEP / PUPPP)
- Most common pregnancy rash
- Onset in 3rd trimester, begins in abdominal striae
- Erythematous urticarial papules and plaques; umbilicus typically spared
- Spreads to thighs, buttocks, proximal arms; face spared
- Associated with: primigravida, multiple gestation, increased weight gain
- All labs normal (DIF, H&E, LFTs all nonspecific)
- No fetal risk
- Does NOT recur in subsequent pregnancies (unlike ICP)
- Treatment: Topical corticosteroids + antihistamines; oral steroids for severe cases
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1717
3. Gestational Pemphigoid (Pemphigoid Gestationis)
- Rare autoimmune blistering disorder
- Periumbilical involvement - vesiculobullous + urticarial eruption
- DIF: linear C3 deposition along the dermal-epidermal junction (diagnostic)
- Associated with small-for-dates babies and prematurity
- Treatment: Corticosteroids + antihistamines
4. Atopic Eruption of Pregnancy (AEP)
- Typically presents before the third trimester (75% < 3rd trimester)
- 80% are first occurrence of atopic disease; 20% are flares of pre-existing atopic dermatitis
- Trunk and extremities involved
- ± elevated IgE; no fetal risk
- Treatment: Corticosteroids + antihistamines + UVB
5. Benign Pruritus Gravidarum
- Generalized itching without cholestasis, without rash
- Associated with: twin pregnancy, fertility treatments, diabetes, nulliparity
- Up to 14% of pregnant women experience itching; most is benign
- No adverse perinatal outcomes when there is no cholestasis
- Treatment: emollients, topical antipruritics, oral antihistamines, UV light
Clinical Approach with Normal LFTs
Normal LFTs + Pruritus in 3rd trimester
↓
Check SERUM BILE ACIDS (fasting)
↓
├── Bile acids >10 µmol/L → ICP → UDCA + fetal monitoring
│ (LFTs may normalize or lag - bile acids are the gold standard)
│
└── Bile acids normal → Does patient have primary skin lesions?
├── Urticarial papules in striae, umbilicus spared → PEP/PUPPP
├── Vesiculobullous, periumbilical → Gestational Pemphigoid (DIF)
├── Eczematous, trunk+limbs, early onset → AEP
└── No lesions, no bile acid elevation → Benign Pruritus Gravidarum
Key Takeaways
- Normal LFTs do not exclude ICP - serum bile acids must always be checked separately
- ICP = pruritus without primary skin lesions - excoriations are secondary
- PEP/PUPPP is the most common rash in 3rd trimester and is benign
- ICP carries real fetal risk (prematurity, fetal distress, stillbirth) - must not be missed
- If initial bile acids are normal but suspicion remains high, repeat testing as levels can fluctuate
- Serum glutathione S-transferase-α is a specific marker distinguishing ICP from benign pruritus gravidarum
Sources: Creasy & Resnik's Maternal-Fetal Medicine, pp. 1716-1717; Dermatology 2-Volume Set 5e, Fig. 27.10
Hypertensive emmergency vs urgency
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Here it is:
Hypertensive Emergency vs. Hypertensive Urgency
Diagnostic Algorithm
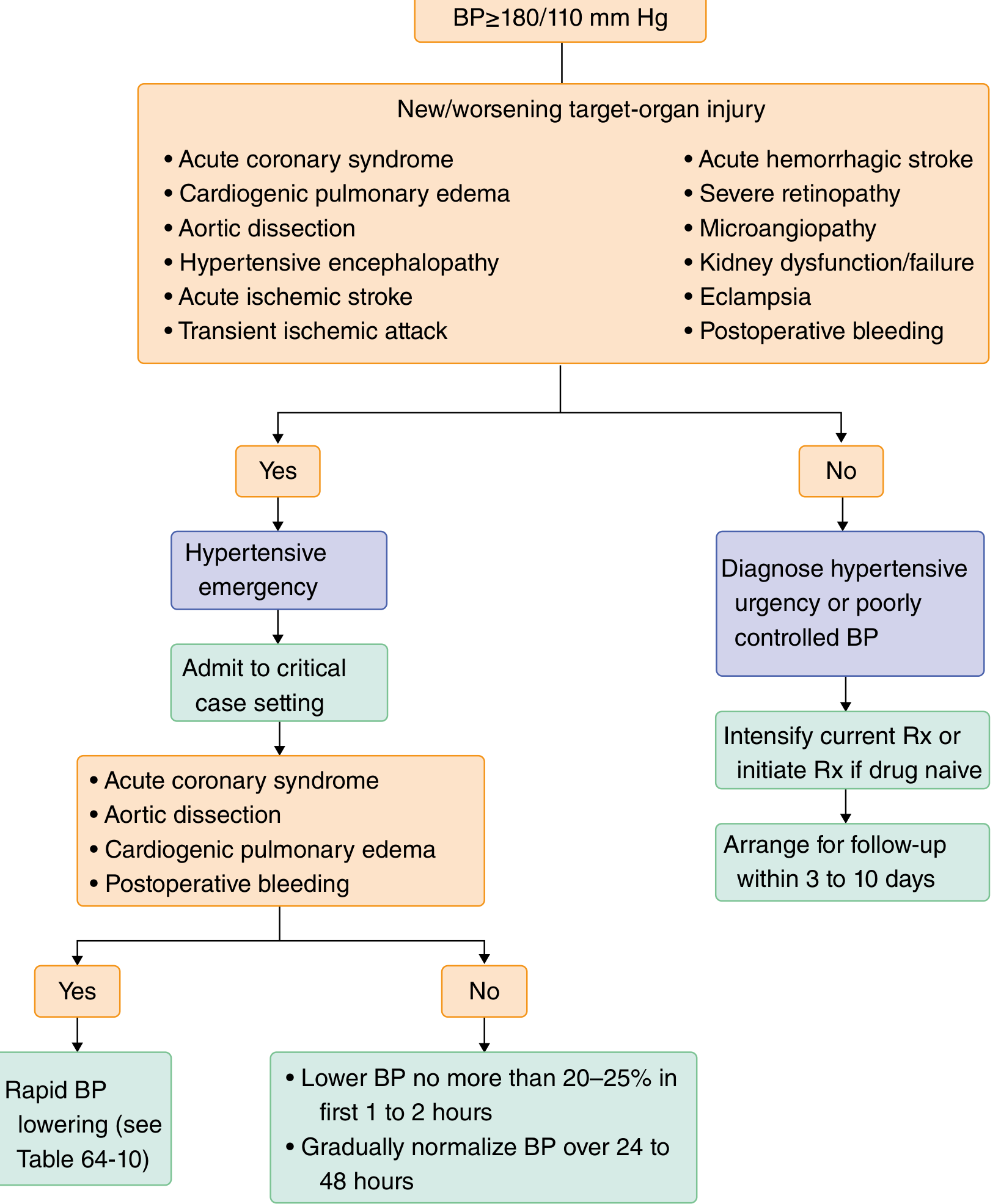
Goldman-Cecil Medicine, Fig. 64-5
Core Definition - The Fundamental Distinction
"A hypertensive emergency is defined by the presence of target-organ damage (TOD), NOT by the degree of BP elevation."
- Symptom to Diagnosis: An Evidence-Based Guide, 4e
Both conditions share similar BP thresholds (typically ≥180/110 mmHg), but the presence or absence of acute end-organ damage is what separates them.
Side-by-Side Comparison
| Feature | Hypertensive Emergency | Hypertensive Urgency |
|---|---|---|
| BP threshold | Usually >180/110 mmHg | Usually >180/110 mmHg |
| End-organ damage | YES - new or worsening | NO |
| Symptoms | Symptomatic (neurologic, cardiac, etc.) | Often asymptomatic or vague |
| Risk | Life-threatening; imminent organ failure | No immediate life threat |
| Setting | ICU / critical care | Outpatient / ED with oral therapy |
| Route of treatment | IV medications | Oral medications |
| Speed of BP reduction | Minutes to hours (goal-directed) | Hours to days |
| Admission | Mandatory | Usually not required |
| Incidence | ~0.3% of ED visits | ~1% of ED visits |
Organs at Risk in Hypertensive Emergency
The target organs most affected are the brain, heart, kidneys, and great vessels:
| System | Manifestations |
|---|---|
| CNS | Hypertensive encephalopathy, acute ischemic stroke, hemorrhagic stroke, subarachnoid hemorrhage, TIA |
| Cardiovascular | Acute coronary syndrome, cardiogenic pulmonary edema, aortic dissection |
| Renal | Acute kidney injury, thrombotic microangiopathy |
| Eyes | Severe retinopathy, papilledema |
| Obstetric | Severe preeclampsia, eclampsia, HELLP syndrome |
| Other | Microangiopathic hemolytic anemia, postoperative bleeding |
Hypertensive Encephalopathy - A Key Emergency to Know
- Severe BP elevation + obtundation, visual disturbances, altered sensorium, seizures
- Marked hypertensive retinopathy ± papilledema
- Absence of focal neurologic findings (if focal findings present, think stroke)
- A subset have posterior reversible leukoencephalopathy syndrome (PRES) - symmetrical vasogenic edema in occipital regions on MRI
- Goldman-Cecil Medicine, p. 759
Important Clinical Pearl: BP Level ≠ Emergency
A normotensive pregnant woman can develop significant TOD at 160/100 mmHg (eclampsia), while a patient with chronic hypertension may be asymptomatic at 220/130 mmHg. Always assess for TOD clinically - don't rely solely on BP numbers.
Common Causes of Both
- Medication nonadherence (most common)
- Abrupt cessation of clonidine or beta-blockers (rebound hypertension)
- CKD / renovascular disease
- Sympathomimetic drugs (cocaine, PCP, methamphetamine)
- Eclampsia
- Postoperative state
- Pheochromocytoma, Cushing syndrome (less common)
Treatment
Hypertensive Urgency
- Restart stopped medications or switch to longer-acting agents
- Start oral antihypertensives in treatment-naive patients
- Schedule prompt follow-up within 3-10 days
- Avoid rapid BP reduction - risk of precipitating ischemia
- Do NOT routinely transfer to ED or hospitalize
Hypertensive Emergency
General BP reduction goals:
- For most emergencies (not requiring rapid correction): reduce MAP by ≤20-25% in the first 1-2 hours, then gradually normalize over 24-48 hours
- For select emergencies requiring immediate reduction (ACS, aortic dissection, cardiogenic pulmonary edema): faster, more aggressive targets
Situation-specific IV drug choices (Goldman-Cecil, Table 64-11):
| Clinical Situation | Target | First-line | Alternative |
|---|---|---|---|
| Malignant HTN / AKI / TMA | MAP -20-25% over several hours | Labetalol or Nicardipine | Nitroprusside |
| Hypertensive encephalopathy | MAP -20-25% immediately | Labetalol or Nicardipine | Nitroprusside |
| Acute ischemic stroke (BP >220/120) | MAP -15% within 1 hour | Labetalol or Nicardipine | Nitroprusside |
| Ischemic stroke + thrombolytics (BP >185/110) | MAP -15% within 1 hour | Labetalol or Nicardipine | Nitroprusside |
| Hemorrhagic stroke (sBP >180) | sBP 130-180 mmHg immediately | Labetalol or Nicardipine | Urapidil |
| Acute coronary event | sBP <140 mmHg immediately | Nitroglycerin or Labetalol | Urapidil |
| Cardiogenic pulmonary edema | sBP <140 mmHg immediately | Nitroprusside or NTG + loop diuretic | Urapidil + loop diuretic |
| Aortic dissection | sBP <120 mmHg + HR <60 immediately | Esmolol + Nitroprusside/NTG | Labetalol or Metoprolol |
| Eclampsia / severe preeclampsia / HELLP | sBP <160, dBP <105 immediately | MgSO4 + Labetalol or Nicardipine | - |
IV Drug Class Summary (Lippincott Pharmacology)
- Calcium channel blockers: Nicardipine, Clevidipine (titratable, predictable)
- Nitric oxide vasodilators: Nitroprusside (rapid, short-acting; cyanide toxicity risk), Nitroglycerin (preferred in ACS/pulmonary edema)
- Adrenergic antagonists: Labetalol (α+β blocker, workhorse agent), Esmolol (β1-selective, very short-acting - ideal for aortic dissection), Phentolamine (for pheochromocytoma)
- Vasodilator: Hydralazine (arteriolar; used in pregnancy)
- Dopamine agonist: Fenoldopam (renal-protective, useful in AKI)
Key Exam Points
- Emergency = TOD present → IV drug, ICU admission
- Urgency = no TOD → oral drug, outpatient follow-up
- Aortic dissection: needs both HR and BP control simultaneously - beta-blocker first, then vasodilator; target HR <60 and sBP <120
- Acute ischemic stroke: avoid over-lowering BP (disrupts autoregulation in ischemic penumbra); only treat if >220/120 or if giving thrombolytics (>185/110)
- Eclampsia: MgSO4 is for seizure prophylaxis/treatment - NOT an antihypertensive; add labetalol or nicardipine for BP control
- DO NOT use nitroprusside in pregnancy (fetal cyanide toxicity)
- The term "malignant hypertension" (older term) = accelerated hypertension with papilledema + retinopathy - now classified under hypertensive emergency
Sources: Goldman-Cecil Medicine, pp. 758-760; Lippincott Illustrated Reviews Pharmacology; Symptom to Diagnosis 4e; Comprehensive Clinical Nephrology 7e
3.6x2.1 cm right breast mass in 45 year female proven infiltrating breast carcinoma RB score grade 3. What will be the management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"breast cancer" AND "grade 3" AND "neoadjuvant chemotherapy"
Finding Sources
Finding Sources
Finding Sources
Finding Sources
3.6x2.1 cm right breast mass in 45 year female proven infiltrating breast carcinoma RB score grade 3. What will be the management. Nodes are negative
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
I send one of my collegue BRCA 1 and BRCA2 mutation test through blood. She is completely normal but had family history. Her mother grand mother had ca breast.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent - I now have comprehensive content from multiple authoritative sources to give a complete, nuanced answer. This is a critically important clinical scenario.
BRCA1/2 Negative with Family History of Breast Cancer - What Does It Mean?
The Most Important Message First
A negative BRCA1/2 test in an unaffected person with family history does NOT mean she is at average population risk.
This is one of the most common and dangerous misinterpretations in genetic counseling.
Understanding the Test Result
Three Possible Outcomes of BRCA Testing
(Current Surgical Therapy 14e)
| Result | Meaning |
|---|---|
| Positive (pathogenic mutation) | Definitive increased risk; actionable |
| Negative | Interpretation depends entirely on family context |
| Variant of Unknown Significance (VUS) | Found but not proven pathogenic; often reclassified over time |
Why Negative ≠ "Normal" in Her Case
The interpretation of a negative BRCA result depends critically on whether an affected family member was tested first. - Schwartz's Principles of Surgery 11e
Scenario A: No Affected Family Member Was Tested First (Her Case - Most Likely)
Your colleague's mother and grandmother had breast cancer but apparently were not tested first. In this situation:
"In a family with a history suggestive of hereditary breast cancer and no previously tested member, the most informative strategy is first to test an affected family member."
- Schwartz's Principles of Surgery 11e
If no affected member was tested, a negative result in an unaffected woman is called a "true negative" or "uninformative negative" - and it means:
- We don't know what mutation the family carries
- Her negative test cannot be compared to a known family mutation
- She may still carry a mutation not yet identified, or the family cancer may be due to a different gene entirely
- Her risk reduction CANNOT be confirmed
Scenario B: If an Affected Relative Was Tested and Found Positive, THEN She Was Tested
- A negative result = "true negative" - she has NOT inherited that specific mutation
- Her risk reverts toward population risk for that specific gene
- BUT she still has elevated risk from other genes and shared environmental/lifestyle factors
Why BRCA Negative Doesn't Equal No Risk
BRCA1/2 explain only a fraction of hereditary breast cancer
"Hereditary breast cancer (HBC) accounts for only 5-10% of all breast cancers. Familial breast cancer (FBC) - affecting several members of a family but NOT attributable to any known mutation - accounts for 20-30%."
- Bailey & Love's Surgery 28e
So there are many other genes and mechanisms at play:
| Gene | Associated Risk |
|---|---|
| BRCA1 (17q21) | 50-85% lifetime breast cancer risk; up to 40% ovarian cancer |
| BRCA2 (13q12.3) | Up to 50-60% lifetime breast cancer risk; 20% ovarian cancer |
| PALB2 | Moderate-high risk; "partner of BRCA2" |
| CHEK2 | Moderate risk; risk increases with more affected family members |
| ATM | Moderate risk |
| TP53 | Li-Fraumeni syndrome |
| PTEN | Cowden syndrome |
| CDH1 | Hereditary diffuse gastric + lobular breast cancer |
| Unknown/polygenic | Familial clustering without identifiable mutation (20-30% of cases) |
Women who tested negative for BRCA before 2014 are being offered repeat testing with contemporary panels because many additional genes have since been identified.
- Current Surgical Therapy 14e
What Should Be Done Now
Step 1: Clarify Who Was Tested in the Family
- Was the mother or grandmother (affected members) tested for BRCA?
- If not, the most informative next step is to test the affected family member first
- If the mother's mutation is identified and your colleague tests negative for that specific mutation = true reassurance
- If no affected member is available to test, your colleague's negative test is uninformative
Step 2: Expand the Genetic Panel
BRCA1/2 alone is insufficient. She should have a multi-gene panel including at minimum:
- BRCA1, BRCA2, CHEK2, PALB2, ATM, CDH1, PTEN, TP53
- Some centers test 77+ genes
- Current Surgical Therapy 14e
Step 3: Risk Assessment with a Validated Model
Regardless of genetic testing results, calculate her lifetime breast cancer risk using:
- BOADICEA (most accurate for family history)
- IBIS (Tyrer-Cuzick) model
- Gail model (less accurate for strong family history)
If her lifetime risk ≥20-25% → she qualifies for high-risk surveillance (annual MRI + mammogram) even with a negative BRCA test.
Step 4: Refer to Genetic Counselor
"Genetic testing should not be offered in isolation, but only in conjunction with patient education and counseling, including referral to a genetic counselor."
- Schwartz's Principles of Surgery 11e
A pre- and post-test genetic counseling consultation is essential - this includes developing a full 3-generation pedigree.
Indications for Genetic Risk Evaluation in Her Family Situation
Per Bailey & Love's Surgery 28e, the following criteria apply to her:
- Breast cancer at any age with two or more affected relatives - her mother AND grandmother qualify
She meets criteria for formal genetic risk evaluation.
Surveillance Recommendations for Her (Regardless of BRCA Result)
Given family history of breast cancer in 1st-degree (mother) and 2nd-degree (grandmother) relatives, she is likely in the intermediate-to-high risk category:
| Risk Category | Recommendation |
|---|---|
| Lifetime risk ≥20-25% | Annual mammogram + annual breast MRI (staggered every 6 months) + clinical breast exam every 6-12 months |
| Lifetime risk 15-20% | Discuss adding MRI to annual mammogram |
| Lifetime risk <15% | Standard population screening (mammogram from age 40-50) |
"Annual MRI screening as an adjunct to annual screening mammography is recommended beginning at age 30 for females at high lifetime risk."
- Sabiston Textbook of Surgery
Risk-Reduction Options if She Is High-Risk
| Intervention | Benefit |
|---|---|
| Chemoprevention - Tamoxifen (premenopausal) or Anastrozole | Reduces breast cancer risk by 40-62% in high-risk women |
| Prophylactic bilateral mastectomy | Reduces risk by ~90% (for confirmed mutation carriers) |
| Bilateral salpingo-oophorectomy | For confirmed BRCA carriers at age 35-40 after family completion |
| Intensive surveillance | Does not reduce risk but enables early detection |
Summary: What to Tell Your Colleague
-
Her BRCA1/2 negative result is NOT reassuring by itself - it is likely uninformative because no affected family member was tested first
-
She needs:
- Expanded multi-gene panel testing (not just BRCA1/2)
- Ideally, testing of her mother (affected) first, then comparison
- Formal genetic counseling with 3-generation pedigree
- Risk model calculation (BOADICEA/IBIS)
-
If lifetime risk ≥20-25%: annual mammogram + annual MRI starting from age 30 (or earlier based on youngest age of cancer in family)
-
Familial breast cancer (without identifiable mutation) still carries elevated risk and needs surveillance
-
She does NOT need prophylactic mastectomy unless a confirmed pathogenic mutation is found
Sources: Schwartz's Principles of Surgery 11e; Bailey & Love's Surgery 28e; Current Surgical Therapy 14e; Sabiston Textbook of Surgery
Labetalol dosage
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have complete, precise dosing data from multiple sources. Here is the comprehensive answer:
Labetalol - Complete Dosage Reference
Mechanism
Labetalol is a combined α₁ + β₁ + β₂ adrenergic receptor blocker (non-selective beta + selective alpha-1).
- Oral: α₁:β blocking ratio = 1:3
- IV: β-blocking potency is more prominent
- Net effect: reduces heart rate, cardiac output, and peripheral vascular resistance
I. INTRAVENOUS DOSAGE - Hypertensive Emergency
A. Intermittent IV Bolus Method
| Step | Dose | Timing |
|---|---|---|
| Initial bolus | 20 mg IV over 2 minutes | - |
| Repeat doses | 40 mg then 80 mg IV | Every 10 minutes |
| Maximum cumulative dose | 220 mg | Stop if reached |
"20 mg IV, followed by doubled doses up to 80 mg (20→40→80) every 10 min; maximum total dose 220 mg"
- Tintinalli's Emergency Medicine
B. Continuous IV Infusion Method
| Parameter | Dose |
|---|---|
| Starting rate | 0.5-2 mg/min (or 2-8 mg/min per some protocols) |
| Titrate to | Target BP response |
| Maximum | 300 mg total dose |
"Labetalol 20-80 mg bolus every 10 minutes up to maximum dose of 300 mg, or 0.5-2 mg/min infusion"
- Plum & Posner's Diagnosis and Treatment of Stupor and Coma
"10 mg IV over 1-2 min, may repeat once; IV infusion 2-8 mg/min"
- Comprehensive Clinical Nephrology 7e (for stroke-associated hypertension)
C. Onset and Duration (IV)
- Onset: 2-5 minutes
- Peak: 5-15 minutes
- Duration: 3-6 hours
II. ORAL DOSAGE - Chronic Hypertension
| Parameter | Dose |
|---|---|
| Initial dose | 100 mg twice daily (BD) |
| Maintenance dose | 200-400 mg twice or thrice daily |
| Maximum dose | 1200-2400 mg/day (divided doses) |
| Dosing interval | BD (twice daily) |
| Peak response | 3 hours after oral dose |
| Duration of action | 8-12 hours |
"The usual initial dosages for treatment of hypertension are 100 mg orally twice daily, increasing gradually to a maintenance dosage of 200-400 mg twice or thrice daily."
- Brenner and Rector's The Kidney 2-Volume Set
III. Special Clinical Situations
| Situation | Dosage Notes |
|---|---|
| Preeclampsia / Eclampsia | 20 mg IV bolus → 40 → 80 mg every 10 min; max 220 mg; target sBP <160, dBP <105 mmHg |
| Aortic dissection | Combine with vasodilator (nitroprusside/NTG); target sBP <120 mmHg + HR <60 |
| Acute ischemic stroke | 10 mg IV over 1-2 min; can repeat; infusion 2-8 mg/min |
| Renal impairment (CKD) | No dose adjustment needed |
| Hepatic impairment | Dose reduction required - chronic liver disease decreases first-pass metabolism |
IV. Pharmacokinetics
| Parameter | Value |
|---|---|
| Metabolism | Hepatic (first-pass) |
| Excretion | 50-60% urine, remainder bile/feces |
| Dose adjustment in CKD | Not required |
| Dose adjustment in liver disease | Required (reduce dose) |
V. Contraindications
- Sinus bradycardia / heart block (>1st degree)
- Decompensated heart failure
- Severe bronchospasm / reactive airway disease (blocks β₂)
- Cardiogenic shock
- Note: In stroke with raised ICP, labetalol is preferred over nitroprusside because it does not increase ICP and does not lower cerebral blood flow - Comprehensive Clinical Nephrology 7e
Quick Reference Summary
| Route | Starting Dose | Max |
|---|---|---|
| IV bolus | 20 mg over 2 min | 220 mg total |
| IV infusion | 0.5-2 mg/min | 300 mg total |
| Oral | 100 mg BD | 2400 mg/day |
Sources: Tintinalli's Emergency Medicine; Brenner & Rector's The Kidney; Plum & Posner's Coma; Comprehensive Clinical Nephrology 7e
This is a shared conversation. Sign in to Orris to start your own chat.