Treatment of dry eyes in the most detailed manner
Reading File
Finding Sources
Finding Sources
Searching PubMed
"dry eye disease" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Searching the Web
dry eye disease treatment guidelines TFOS DEWS II 2023 2024 updated recommendations
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full detailed response.
Treatment of Dry Eye Disease - Comprehensive Guide
Sources: Kanski's Clinical Ophthalmology 10th Ed., Goodman & Gilman's Pharmacological Basis of Therapeutics, Firestein & Kelley's Textbook of Rheumatology, TFOS DEWS II/III guidelines
Overview and Treatment Philosophy
Dry eye disease (DED) is a multifactorial disorder driven by tear film instability, hyperosmolarity, ocular surface inflammation, and neurosensory abnormalities. The underlying causative processes are generally not fully reversible; management is therefore structured around:
- Control of symptoms
- Prevention of ocular surface damage
- Breaking the self-perpetuating cycle of inflammation
The TFOS DEWS II and III guidelines (the global standard) recommend a stepwise, severity-based approach, proceeding from least invasive to most aggressive interventions. The framework spans 4 levels.
TFOS DEWS Stepwise Management Framework
LEVEL 1 - First-Line Measures (Mild Disease)
A. Education and Lifestyle Modification
- Establish realistic expectations - explain that DED is usually chronic and manageable, not curable
- Blink training: Patients should be taught to blink consciously and completely while reading, watching TV, or using screens
- Screen positioning: Computer monitors should be placed below eye level to minimize palpebral aperture width and reduce evaporation
- Contact lens wear: Review lens material, replacement schedule, and wearing hours; consider switching to silicone hydrogel or reducing wear time
- Environmental modification: Increase indoor humidity using humidifiers, avoid direct airflow from fans/air conditioning, wear wraparound glasses outdoors
- Laser refractive surgery caution: Warn patients that LASIK can exacerbate or unmask pre-existing DED (corneal nerve disruption reduces reflex tearing)
- Reduce screen time or use the 20-20-20 rule
B. Systemic Medication Review
Many drugs reduce tear production or alter tear composition. Offending agents should be identified and, where possible, substituted or discontinued:
- Antihistamines (H1 blockers)
- Tricyclic antidepressants and SSRIs
- Beta-blockers (systemic and topical)
- Diuretics
- Isotretinoin
- Antipsychotics
- Anticholinergics (e.g., oxybutynin, scopolamine)
- Hormone replacement therapy (estrogen-only)
- Any topical preserved ophthalmic medication taken long-term
C. Artificial Tear Substitutes (Preserved Formulations at Level 1)
Tear substitutes are the backbone of DED management. They cannot replicate the complex structure of natural tears but provide lubrication and dilute inflammatory mediators. Key categories:
| Agent | Mechanism / Notes |
|---|---|
| Cellulose derivatives (hypromellose, methylcellulose, carboxymethylcellulose) | Appropriate for mild cases; short residence time |
| Carbomer gels (carbopol) | Mucoadhesive, longer-lasting; may cause transient blurring |
| Polyvinyl alcohol (PVA) | Increases tear film persistence; useful in mucin deficiency |
| Sodium hyaluronate | Viscoelastic, promotes epithelial healing; popular in moderate disease |
| Polyethylene glycol / propylene glycol | Lubricants found in many commercial formulations |
| Glycerin / polysorbate / povidone | Additional lubricant and stabilizing agents |
| Diquafosol | Topical P2Y2 receptor agonist - acts as a secretagogue stimulating both aqueous and mucin secretion |
- The optimal frequency of instillation varies with agent and disease severity
- No single preparation has demonstrated superiority; patient preference often guides selection
- Preservative-free (PF) formulations should be used for any patient requiring drops more than 3-4 times/day - benzalkonium chloride (BAK) is toxic to goblet cells and the epithelium
Ointments: White petrolatum/mineral oil ± lanolin. Highly viscous - cause marked blurring, so reserved for bedtime use, critically ill/sedated patients, or very severe DED.
Eyelid sprays: Liposome-based, applied to closed eyelids - stabilize the lipid layer and reduce evaporative loss. Useful in meibomian gland dysfunction (MGD).
Artificial tear inserts: Hydroxypropyl cellulose (Lacrisert) placed in the inferior cul-de-sac once or twice daily - dissolves slowly throughout the day for extended-duration treatment.
D. Eyelid Hygiene (Blepharitis/MGD)
- Warm compresses: Soften inspissated meibomian secretions; 5-10 min twice daily. A face cloth or commercial eyelid warming mask works
- Lid scrubs: Eyelid detergent (diluted baby shampoo 1:1 with water, or commercial lid wipes) to remove debris, crusts, and biofilm
- Some ophthalmologists avoid scrubs as they can irritate
- Reparative lid surgery (early consideration): Entropion, ectropion, lid laxity, or scleral show should be corrected promptly as they cause mechanical surface damage
Nocturnal lagophthalmos management:
- Tape lids closed at bedtime
- Swim goggles during sleep
- In extreme cases: lateral tarsorrhaphy
LEVEL 2 - Second-Line Measures (Mild-Moderate Disease)
A. Preservative-Free Tear Substitutes
Some guidelines classify non-preserved drops as a Level 2 measure (vs. preserved at Level 1). Excessive preserved drops cause toxicity, especially after punctal occlusion.
B. Anti-Inflammatory Agents
Inflammation is both a cause and consequence of DED - targeting it is central to disease modification.
1. Topical Corticosteroids
- Short courses (1-2 weeks) of low-potency steroids (loteprednol, fluorometholone) reduce acute surface inflammation and can "prime" the eye before starting cyclosporine
- Not for long-term use due to risks of IOP elevation, cataract, and infection
- Useful in flares of inflammatory DED
2. Cyclosporine (Ciclosporin) Ophthalmic Emulsion
- Restasis (0.05%) - FDA-approved for keratoconjunctivitis sicca (KCS)
- Mechanism: calcineurin inhibitor - blocks T-lymphocyte activation, reduces IL-2-driven inflammatory cascade on the ocular surface, restoring goblet cell density
- Clinical trials showed statistically significant improvement in tear production (Schirmer I test) and symptoms
- Onset of action: typically 3-6 months
- Side effect: burning/stinging on instillation (common; limits tolerability)
- Cequa (cyclosporine 0.09%) - nanomicellular aqueous formulation; FDA-approved with improved bioavailability and lower instillation site pain compared to Restasis
- Dosing: twice daily, both eyes
3. Lifitegrast (Xiidra, 5%)
- FDA-approved for DED signs and symptoms
- Mechanism: LFA-1 (lymphocyte function-associated antigen-1) antagonist - blocks the LFA-1/ICAM-1 interaction, disrupting T-cell recruitment and activation on the ocular surface
- Improves symptoms vs. placebo in RCTs; not directly compared with cyclosporine in head-to-head trials
- Side effects: ocular irritation, dysgeusia (unusual taste sensation due to nasolacrimal drainage)
- Dosing: twice daily; works faster than cyclosporine (some benefit within 2-12 weeks)
4. Oral Omega Fatty Acids
- Omega-3 fatty acids (EPA/DHA from fish oil) have anti-inflammatory properties
- May improve meibomian gland function and tear stability in MGD-driven evaporative DED
- Evidence is mixed (DREAM trial showed no significant benefit vs. olive oil placebo), but widely used
- Omega-6 (gamma-linolenic acid from evening primrose or borage oil) may also be beneficial
C. Tetracyclines (For MGD, Meibomianitis, Ocular Rosacea)
- Doxycycline (100 mg/day or 50 mg twice daily) is the preferred agent
- Mechanism: not purely antimicrobial - key effect is inhibition of matrix metalloproteinases (MMPs), which degrade tear film proteins and damage the epithelium; also reduces bacterial lipase activity, improving meibum quality; anti-inflammatory via NF-κB pathway inhibition
- Minocycline is an alternative
- Low-dose (sub-antimicrobial) doxycycline 40 mg/day (Oracea) is also effective with lower antibiotic resistance risk
- Duration: typically 3-6 months
D. Punctal Plugs (Temporary)
- Preserve natural tears by blocking nasolacrimal drainage
- Indicated when symptoms persist despite regular artificial tear use
- 90% of tears drain through the inferior punctae - plugs are therefore inserted in the two inferior punctae first
- Trial with temporary/dissolvable collagen plugs first before permanent occlusion (to ensure epiphora doesn't occur)
- Silicone intracanalicular or punctal plugs for longer-term use
- Most frequent complication: excessive tearing (epiphora)
E. Secretagogues
- Pilocarpine 5 mg 3-4x/day - M3 muscarinic agonist; stimulates lacrimal and salivary gland secretion; evidence from RCTs for both dry eye and dry mouth (especially in Sjögren's)
- Cevimeline - more selective M3/M1 agonist; longer duration than pilocarpine; 30 mg 3x/day
- Rebamipide - mucin secretagogue; stimulates goblet cell mucin production; widely used in Asia
- Varenicline nasal spray (Tyrvaya) - FDA-approved; activates the trigeminal parasympathetic pathway via the nose to stimulate tear production; novel delivery route; 0.03 mg twice daily
- Side effects of muscarinic agonists: sweating, flushing, urinary frequency, GI cramping, bradycardia - use with caution in asthma, cardiac disease, peptic ulcer
F. Moisture Chamber Spectacles
- Wraparound frames with side shields or sealed chambers reduce air exposure and evaporation
- Useful in severe evaporative DED and in occupational exposure to dry environments
LEVEL 3 - Third-Line Measures (Moderate-Severe Disease)
A. Serum Eye Drops
Autologous serum is prepared from the patient's own blood:
- Blood drawn from the patient, processed in a specialty laboratory
- Typically diluted to 20% concentration in saline
- Contains growth factors (EGF, TGF-β, fibronectin), vitamins (A, B12, C), IgA antibodies, antioxidants, and proteins absent from artificial tears
- Particularly effective in severe KCS, Sjögren syndrome, graft-versus-host disease (GVHD)-related DED, post-LASIK persistent epithelial defects, and recurrent erosions
- Requires refrigeration; limited shelf-life; preparation is resource-intensive
- Umbilical cord serum (allogeneic) is an alternative with potentially higher growth factor concentrations; avoids patient phlebotomy; emerging evidence
Platelet-rich plasma (PRP) drops are also being explored as an alternative blood derivative with concentrated growth factors.
B. Therapeutic Contact Lenses
- Scleral lenses: Large-diameter rigid gas-permeable lenses that vault the cornea entirely and rest on the scleral conjunctiva; reservoir of saline solution bathes the cornea continuously - highly effective in severe DED, irregular corneas, and Stevens-Johnson syndrome
- Bandage soft contact lenses: Protect the epithelium, reduce pain from erosions; used short-term in severe surface disease
- Both require careful fitting and compliance with hygiene
C. Permanent Punctal Occlusion
- Indicated when temporary plugs have proven beneficial without causing epiphora
- Methods:
- Silicone plugs (removable but sometimes poorly tolerated - can extrude or migrate)
- Thermal cautery (punctal cauterization) - outpatient procedure
- Laser cauterization
- Surgical occlusion (ligation)
- Permanent occlusion is particularly appropriate in patients with severe aqueous deficiency
LEVEL 4 - Fourth-Line Measures (Severe/Refractory Disease)
A. Systemic Anti-Inflammatory Therapy
- Indicated in severe DED associated with systemic autoimmune conditions (Sjögren syndrome, RA, SLE, GVHD)
- Hydroxychloroquine (often first-line for Sjögren's systemic features)
- Methotrexate, azathioprine, mycophenolate mofetil, cyclophosphamide - used by rheumatologists for severe extraglandular disease
- Rituximab (anti-CD20) - evidence in Sjögren's, particularly for reducing B-cell-driven salivary/lacrimal inflammation
- Short systemic corticosteroid courses for acute severe flares
B. Surgery
Eyelid Surgery:
- Tarsorrhaphy (lateral or medial): Partial permanent closure of the eyelid to reduce ocular surface exposure; used in severe neurotrophic keratopathy, facial palsy, or refractory severe DED
- Botulinum toxin injection to the orbicularis muscle: Controls the blepharospasm that often accompanies severe DED; injected at the medial canthus it can also reduce tear drainage
Corneal and Surface Surgery:
- Amniotic membrane transplantation: Provides anti-inflammatory, anti-scarring, and pro-epithelialization effects; used in acute severe surface disease and persistent epithelial defects
- Mucous membrane grafting: Autologous oral mucosa transplanted to reconstruct the conjunctival fornix in severe cicatricial disease (Stevens-Johnson, ocular pemphigoid)
- Salivary gland autotransplantation: Submandibular gland transposition to the orbit - the saliva acts as a tear substitute; reserved for end-stage bilateral severe DED with no other options; risk of mucus hypersecretion and stone formation
Disease-Specific Treatment Considerations
Evaporative Dry Eye (MGD-Dominant)
- First focus on lid hygiene (warm compresses, lid scrubs)
- Thermal pulsation devices (LipiFlow): In-office device that applies controlled heat from inside the eyelid + massage to express stagnant meibomian secretions; single treatment provides months of benefit
- Intense Pulsed Light (IPL): Used periocularly; reduces telangiectatic lid vessels, decreases inflammatory mediators reaching the meibomian glands; FDA-cleared for MGD
- Meibomian gland probing: Mechanical dilation of stenosed gland orifices
- Tetracyclines, eyelid sprays, omega-3 supplements
- Topical azithromycin (macrolide anti-inflammatory + antimicrobial on lid margin)
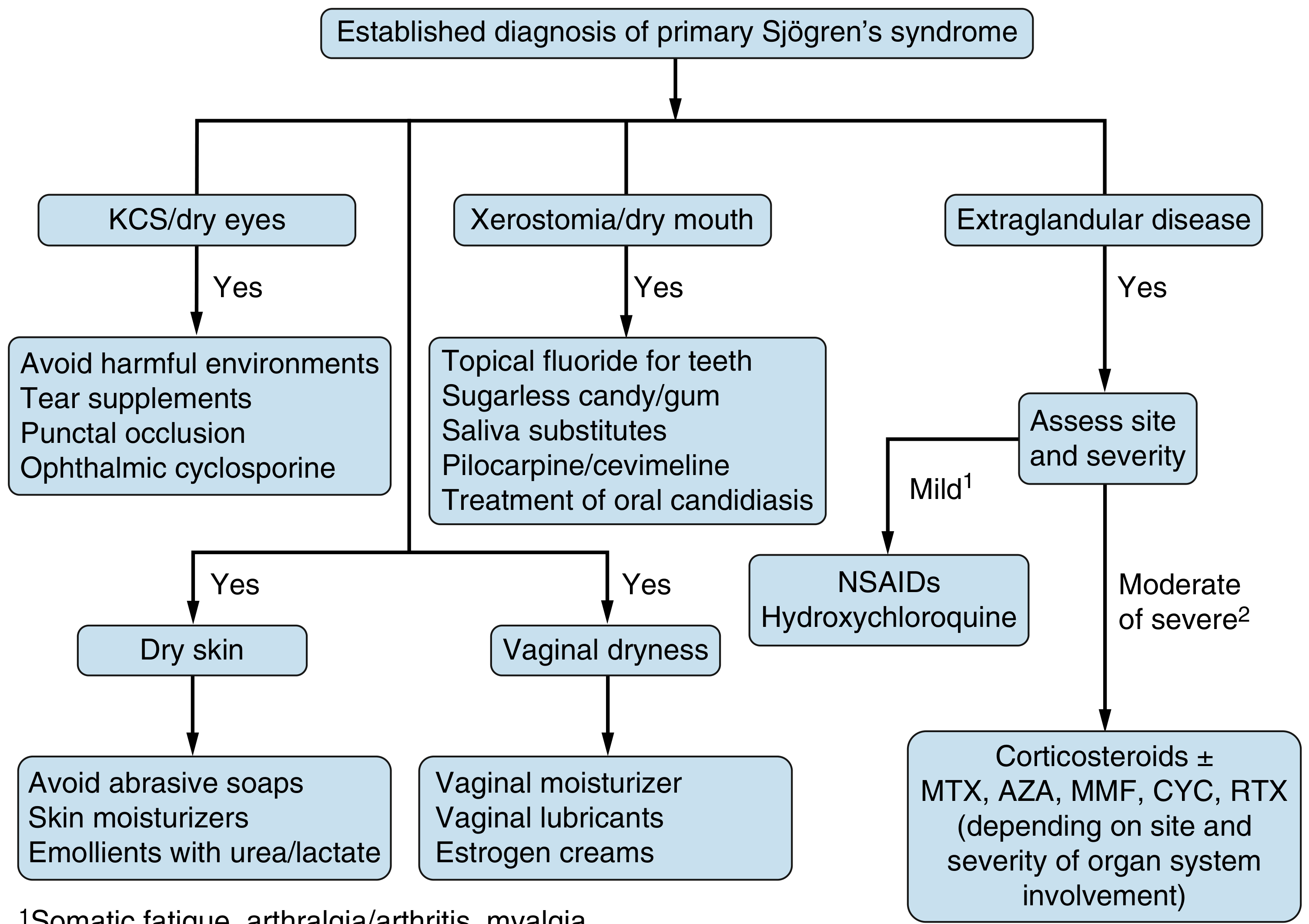
Aqueous-Deficient Dry Eye (Sjögren's Syndrome)
- Cyclosporine/lifitegrast for inflammation
- Pilocarpine/cevimeline to stimulate residual secretion
- Punctal occlusion to conserve tears
- Autologous serum drops in severe cases
- Address systemic disease with rheumatology
GVHD-Related Dry Eye
- Often severe and bilateral
- Autologous or umbilical cord serum drops are particularly effective
- Scleral lenses
- Topical tacrolimus or cyclosporine
- Systemic immunosuppression (managed by transplant team)
Neurotrophic Keratopathy (Reduced Corneal Sensation)
- Cenegermin (Oxervate) - recombinant human nerve growth factor (rhNGF) eye drops; FDA-approved; promotes corneal re-innervation and healing
- Preservative-free artificial tears
- Scleral lenses
- Tarsorrhaphy if severe
Drug-Induced / Iatrogenic Dry Eye
- Post-LASIK: usually self-limited 6-12 months; treat with preservative-free drops ± autologous serum if persistent
- BAK toxicity: switch all drops to preservative-free formulations
- Isotretinoin: dose reduction or cessation if tolerated clinically; supplemental lubrication
Emerging and Investigational Therapies
- Topical insulin eye drops: Systematic reviews (2025) show promise for persistent epithelial defects and neurotrophic disease
- Extracellular vesicles (exosomes): Early evidence for anti-inflammatory and regenerative properties in DED and Sjögren's (2025 systematic review)
- Blood component therapy (platelet-rich plasma, plasma-derived drops): Network meta-analysis (2024) supports their use in severe DED
- Tanezumab and other anti-NGF: For neuropathic ocular pain component
- SYL1001 (siRNA against TRPV1): Reducing pain hypersensitivity
- Stem cell-derived tear substitutes
Mucolytic Therapy
Acetylcysteine 5% drops:
- Useful specifically for patients with corneal filaments and mucous plaques, which the drug dissolves
- May cause stinging; has limited shelf-life and is malodorous
- Manual debridement of filaments is an alternative/adjunct
Preservative Management - Key Points
- Benzalkonium chloride (BAK): The most common preservative; toxic to goblet cells and epithelium with repeated exposure; prolongs surface exposure time but damages surface cells
- Polyquad and Purite: Newer preservatives with significantly lower ocular surface toxicity - preferred when preservative-free is unavailable
- Rule: Preservative-free drops should be used when instilling drops more than 3-4 times daily, in any moderate-severe disease, and in all patients with concurrent topical glaucoma therapy
Summary Table: Treatment by Severity
| Severity | First-line | Add-on | Advanced |
|---|---|---|---|
| Mild | Preserved AT, lid hygiene, lifestyle | Omega-3, treat blepharitis | - |
| Moderate | PF artificial tears, topical cyclosporine or lifitegrast | Punctal plugs, tetracyclines, secretagogues | Scleral lenses |
| Severe | PF AT, CsA/lifitegrast, punctal occlusion | Autologous serum, scleral lenses | Surgical options |
| Refractory | Autologous serum, systemic immunosuppression | Tarsorrhaphy, amniotic membrane | Salivary gland transplant |
Monitoring Response to Treatment
- Tear osmolarity (TearLab): correlates with treatment effectiveness in long-term follow-up; target <308 mOsm/L; inter-eye difference >8 mOsm/L suggests instability
- Schirmer test: improvement in strip wetting after cyclosporine therapy
- Corneal/conjunctival staining (fluorescein, lissamine green): reduction in staining area
- Symptom scores: OSDI (Ocular Surface Disease Index), SPEED questionnaire
- Tear meniscus height on slit-lamp or OCT
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed., pp. 179-183
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, pp. 1489-1490
- Firestein & Kelley's Textbook of Rheumatology, pp. 1573-1578
- TFOS DEWS III Management and Therapy Report (2025) - review article
- Blood component therapy meta-analysis PMID 39736981 (2024)
- Topical pharmacologic treatments systematic review PMID 40749992 (2025, Ocular Surface)
This is a shared conversation. Sign in to Orris to start your own chat.