Sore throat – infectious and non infectious causes, red flag symptoms and signs, risk stratification, investigations, empirical management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
pharyngitis management guidelines
I now have all the material needed for a comprehensive, well-structured response. Let me compile it.
Sore Throat: A Comprehensive Clinical Overview
1. Causes
Infectious Causes
Viral (majority — 30–80% of cases)
| Virus | Presentation |
|---|---|
| Rhinovirus / Coronavirus | Common cold; mild pharyngitis with coryza |
| Adenovirus | Pharyngoconjunctival fever (pharyngitis + conjunctivitis) |
| Parainfluenza | Common cold, croup |
| Influenza A & B | Widespread outbreaks; nonexudative pharyngitis + systemic features |
| Epstein-Barr virus (EBV) | Infectious mononucleosis: exudative pharyngitis, posterior cervical lymphadenopathy, splenomegaly |
| Cytomegalovirus (CMV) | Mono-like illness; heterophile-negative |
| Herpes simplex 1 & 2 | Pharyngitis, gingivostomatitis, painful vesicles/ulcers |
| Coxsackievirus A | Herpangina (vesicular eruption on soft palate), hand-foot-mouth disease |
| HIV (acute retroviral syndrome) | Fever, pharyngitis, rash, mucocutaneous ulcers, nontender lymphadenopathy |
| RSV / Measles | Pharyngitis as part of systemic illness |
Bacterial (5–10% adults; 20–40% children)
| Organism | Notes |
|---|---|
| Group A β-haemolytic Streptococcus (GAS/GABHS) | Most common bacterial cause; complications include rheumatic fever, glomerulonephritis, peritonsillar abscess |
| Non-GAS streptococci (Groups B, C, G) | Similar presentation; glomerulonephritis is a sequela, but not rheumatic fever |
| Fusobacterium necrophorum | Young adults (15–45 yrs); primary agent of Lemierre syndrome (septic jugular thrombophlebitis) |
| Arcanobacterium haemolyticum | Teens; urticarial/scarlatiniform rash sparing face, palms, and soles |
| Neisseria gonorrhoeae | Sexually transmitted; white-yellow tonsillar exudate |
| Corynebacterium diphtheriae | Grey-green pseudomembrane; toxin causes myocarditis, neuritis; consider in unvaccinated/travellers |
| Mycoplasma pneumoniae / Chlamydia pneumoniae | Pharyngitis as part of atypical lower respiratory illness; crowded settings |
| Treponema pallidum | Secondary syphilis: pharyngitis ± localised adenopathy; primary syphilis: painless oral ulcer |
| Yersinia enterocolitica | Pharyngitis + enterocolitis |
| Francisella tularensis | Tularemia oropharyngeal form; false-positive monospot |
| Mixed anaerobes | Vincent angina (ulcerative gingivitis) |
Fungal
- Candida spp. — immunocompromised patients (HIV, chemotherapy, prolonged antibiotics, inhaled corticosteroids)
Adjacent Infections Presenting as Sore Throat
- Peritonsillar abscess, retropharyngeal abscess, parapharyngeal abscess, epiglottitis, Ludwig angina
Non-Infectious Causes
| Category | Examples |
|---|---|
| Neoplastic | Pharyngeal/tonsillar malignancy (unilateral tonsil enlargement, persistent symptoms) |
| Autoimmune | PFAPA syndrome, SLE, Behçet disease, Kawasaki disease |
| Mechanical/trauma | Foreign body, thermal burn, heroic snoring |
| Medication-induced | ACE inhibitor-related angioedema, methimazole/carbimazole (agranulocytosis), chemotherapy mucositis |
| Neurogenic pain | Glossopharyngeal neuralgia, Eagle syndrome |
| Thyroiditis | Referred pain to throat |
| Stevens-Johnson syndrome | Mucosal involvement |
| Pericarditis/myocarditis | Referred throat pain |
— ROSEN's Emergency Medicine, Table 61.1; K.J. Lee's Essential Otolaryngology, p. 685
2. Red Flag Symptoms and Signs
These indicate potentially life-threatening deep space infections, airway compromise, or severe systemic illness:
| Red Flag | Concern |
|---|---|
| Stridor | Airway compromise (epiglottitis, retropharyngeal abscess, angioedema) |
| Drooling / inability to swallow | Airway oedema or deep space infection |
| Muffled / "hot potato" voice | Peritonsillar or parapharyngeal abscess |
| Trismus (limited mouth opening) | Peritonsillar or parapharyngeal abscess |
| Sniffing position / tripod posturing | Epiglottitis |
| Neck stiffness or torticollis | Retropharyngeal abscess, meningitis |
| Uvular deviation | Peritonsillar abscess (uvula deviates away from abscess) |
| Unilateral tonsillar swelling | Abscess, malignancy |
| Toxic appearance / sepsis | Invasive GAS, Lemierre syndrome, necrotising fasciitis |
| Hypoxia | Severe airway compromise |
| Progressive symptoms > 1 week | Malignancy, abscess, atypical infection |
| Dyspnoea | Supraglottic/glottic oedema |
| Inability to open mouth | Parapharyngeal / masticator space abscess |
| Anterior neck swelling / "bull neck" | Diphtheria, Ludwig angina |
Stridor is a sign of true airway emergency. It is critical to determine severity, rate of onset, and progression. — ROSEN's Emergency Medicine, p. 883
3. Risk Stratification: Modified Centor Score (McIsaac Score)
Used to estimate the likelihood of GAS pharyngitis and guide testing/treatment decisions.
| Criterion | Points |
|---|---|
| History of fever (>38°C) | +1 |
| Tonsillar exudates | +1 |
| Tender anterior cervical lymphadenopathy | +1 |
| Absence of cough | +1 |
| Age 3–14 years | +1 |
| Age >45 years | −1 |
| Score | Estimated GAS Prevalence | Recommended Action |
|---|---|---|
| 0 or −1 | ~5–10% | No testing or antibiotics |
| 1 | ~10–15% | No testing or antibiotics |
| 2 | ~20–30% | Rapid antigen test (RADT) |
| 3 | ~33–38% | RADT; treat if positive |
| 4–5 | >50% | RADT; strong consideration for empirical treatment |
Testing and treatment should also be avoided when overt viral features are present (cough, rhinorrhoea, oral vesicles/ulcers, conjunctivitis) — a positive test in this context suggests GAS carriage rather than active infection. — ROSEN's Emergency Medicine / Goldman-Cecil Medicine, Table 397-2
4. Investigations
First-Line
| Test | Indication / Notes |
|---|---|
| Rapid antigen detection test (RADT) | Sensitivity ~80–90%, high specificity; positive result warrants treatment |
| Throat culture (swab) | Gold standard; sensitivity 90–95%; 18–48 hrs; use if RADT negative in children/adolescents |
| Nucleic acid amplification test (NAAT) | Sensitivity ~97.5%, specificity ~95%; preferred over RADT where available |
Selective / Second-Line
| Test | Indication |
|---|---|
| Monospot (heterophile antibody test) | Suspected EBV mononucleosis; low sensitivity in young children (<2 yrs) and early illness; negative test does not exclude EBV |
| EBV IgM/IgG serology | Confirms EBV if monospot negative but clinical suspicion high |
| FBC / blood film | Atypical lymphocytes suggest EBV/CMV; left shift in bacterial/TSS |
| Liver enzymes (ALT/AST) | EBV hepatitis (if right upper quadrant tenderness) |
| CMV IgM/IgG | Heterophile-negative mononucleosis |
| HIV fourth-generation test | Acute retroviral syndrome suspected |
| GC/Chlamydia PCR (throat swab) | Sexually active patients with atypical presentations |
| Syphilis serology (RPR/TPHA) | Secondary syphilis; unilateral tonsillar lesion |
| Contrast-enhanced CT neck | Suspected deep space infection (retropharyngeal/parapharyngeal abscess) — cannot be reliably excluded clinically |
| Transcervical or intraoral USS | Peritonsillar abscess diagnosis and drainage guidance |
| CXR / blood cultures | Diphtheria, Lemierre syndrome, sepsis |
| Lateral neck X-ray | Suspected epiglottitis (if patient stable; "thumbprint sign") |
Adult patients with Centor ≥3 should have RADT; in adults with negative RADT, backup throat culture is generally not required because of low GAS incidence and low rheumatic fever risk. In children, backup culture is recommended after negative RADT. — Goldman-Cecil Medicine
5. Empirical Management
Management Algorithm
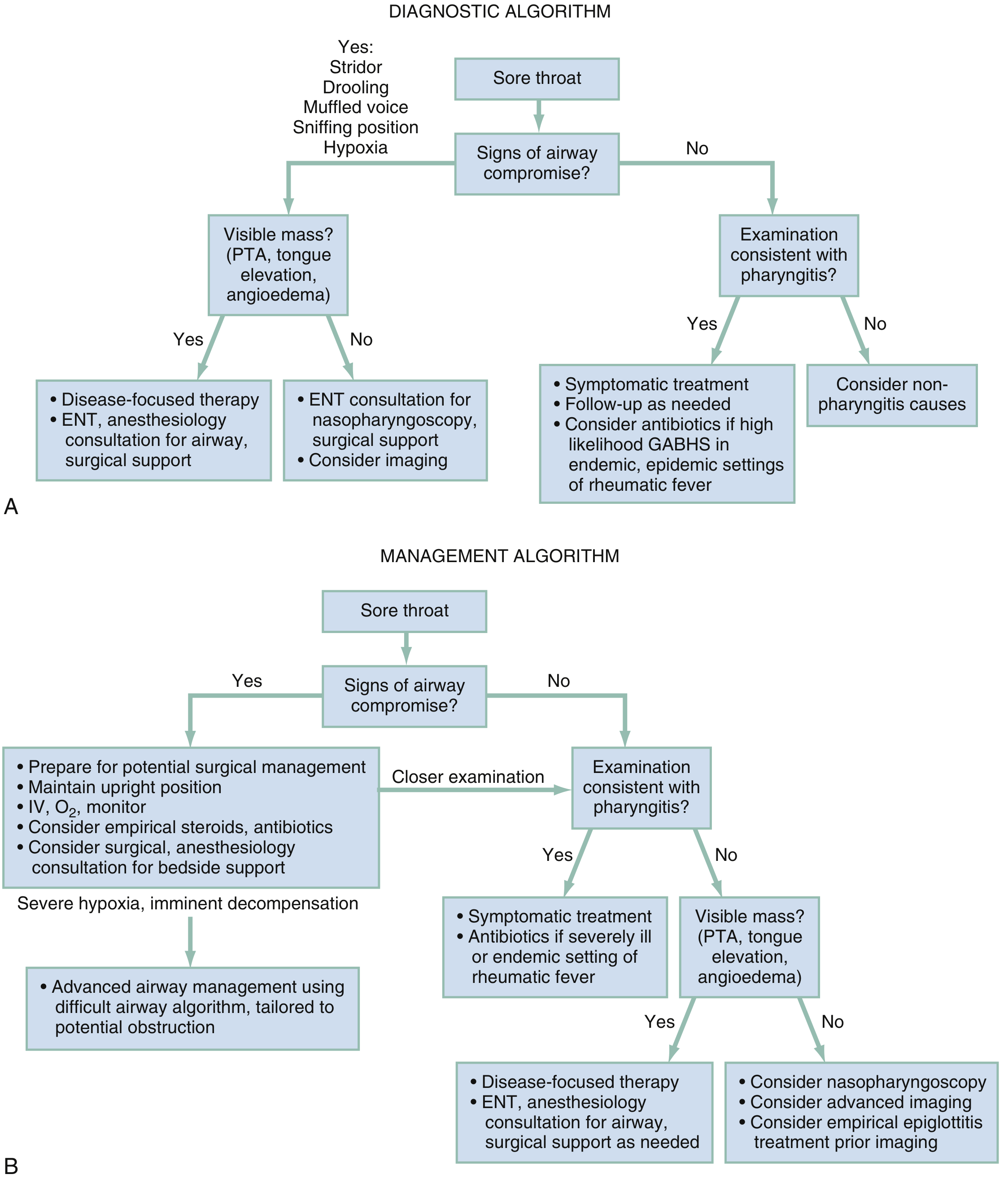
Step 1: Rule Out Airway Compromise (Priority)
- If stridor, drooling, muffled voice, sniffing posture, or hypoxia → prepare for difficult airway
- Maintain upright position; IV access; O₂ monitoring
- Empirical steroids + antibiotics
- Immediate ENT / anaesthesiology / surgical consultation
- Advanced airway management via difficult airway algorithm
Step 2: Symptomatic Treatment (All Cases)
- Analgesia: Paracetamol or NSAIDs (regularly, not PRN)
- Corticosteroids: Single dose dexamethasone 0.6 mg/kg (max 10 mg) PO or IM for patients >5 yrs with severe pain/dysphagia. Reduces pain duration and severity. (Supported by ESCMID guidelines; not routinely endorsed by IDSA for uncomplicated pharyngitis)
- Hydration: Ensure adequate oral intake; IV fluids if severe odynophagia/dehydration
Step 3: Antibiotic Therapy — Condition-Specific
| Pathogen / Condition | First-Line Treatment | Alternative |
|---|---|---|
| GAS pharyngitis | Penicillin V (phenoxymethylpenicillin): 500 mg PO BD × 10 days (adult); Benzathine penicillin G IM 1.2 million units (>27 kg) single dose | Amoxicillin 500 mg TDS × 10 days; Cefuroxime 250 mg BD × 10 days |
| Penicillin allergy (GAS) | Azithromycin 500 mg/day × 3 days; Clindamycin 300 mg QID × 10 days | |
| Recurrent GAS | Clindamycin 300 mg QID × 10 days; Amoxicillin-clavulanate 875 mg BD × 10 days | |
| Group G Streptococcus | Penicillin G IM | |
| Fusobacterium / Lemierre syndrome | Piperacillin/tazobactam; OR ceftriaxone 1g q24h + metronidazole 500 mg q8h | |
| Epiglottitis | Ceftriaxone 50 mg/kg (or 1g) IV OD; OR ampicillin/sulbactam 3g q6h | Levofloxacin 750 mg OD (penicillin allergy) |
| Retropharyngeal/Parapharyngeal abscess / Ludwig angina | Ampicillin/sulbactam 3g q6h; OR penicillin G + metronidazole 500 mg QID | Surgical drainage required |
| Peritonsillar abscess (PTA) | Drainage (definitive); Penicillin + metronidazole or clindamycin IV (parenteral: clindamycin 10 mg/kg or 900 mg TID + ceftriaxone 50 mg/kg or 1g q24h) | |
| Diphtheria | Antitoxin (urgent) + Penicillin/erythromycin | |
| Gonococcal pharyngitis | Ceftriaxone IM/IV | |
| Viral pharyngitis | No antibiotics — supportive care only | |
| Oral candidiasis | Nystatin suspension; Fluconazole for refractory/systemic |
For EBV mononucleosis: avoid amoxicillin/ampicillin (risk of maculopapular rash). Steroids may reduce tonsillar enlargement when swallowing or respiratory symptoms are attributed to enlarged tonsils. Counsel about splenic rupture risk — avoid contact sports until splenomegaly resolves.
Antibiotic Goals in GAS Treatment
- Shorten illness duration (by ~1 day)
- Prevent suppurative complications (PTA, sinusitis, otitis media)
- Prevent transmission (contagious period reduced from 2 weeks to 24 hours post-antibiotics)
- Prevent rheumatic fever (antibiotics must be started within 10 days of symptom onset)
- Note: Antibiotics do not reduce risk of post-streptococcal glomerulonephritis
Antibiotic Stewardship
- Viruses cause most pharyngitis; do not treat based on symptoms and exam alone
- Centor 0–1: no antibiotics, no testing
- Avoid empirical antibiotics without testing in adults (Centor ≥3 only)
- Patient education is key: explain lack of symptomatic benefit from antibiotics and risks (GI side effects, resistance, anaphylaxis, fungal infections)
Summary Table
| Domain | Key Points |
|---|---|
| Most common cause | Viral (rhinovirus, coronavirus, adenovirus) |
| Most important bacterial cause | GAS (S. pyogenes) |
| Risk stratification tool | Modified Centor / McIsaac score |
| Gold standard test | Throat culture (backup to RADT) |
| First-line antibiotic (GAS) | Penicillin V × 10 days |
| Absolute red flags | Stridor, drooling, trismus, uvular deviation, toxic appearance |
| Never do | Amoxicillin/ampicillin in suspected EBV; antibiotics for purely viral presentations |
| Deep space infections | Require contrast CT, ENT consultation, parenteral broad-spectrum antibiotics ± surgical drainage |
Sources:
- ROSEN's Emergency Medicine, Chapters 19 & 61
- Goldman-Cecil Medicine International Edition, Chapters 269 & 397
- K.J. Lee's Essential Otolaryngology, Chapter on Acute Pharyngitis
This is a shared conversation. Sign in to Orris to start your own chat.