Teach me p53
Reading File
Finding Sources
Finding Sources
Searching PubMed
p53 TP53 tumor suppressor cancer
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have rich material from multiple authoritative textbooks plus a clear diagram. Let me compile the comprehensive teaching response.
p53 - The Guardian of the Genome
1. What is p53?
p53 is a 393-amino acid nuclear phosphoprotein encoded by the TP53 gene located on chromosome 17p13.1. It functions as a transcription factor and the cell's central stress monitor. The nickname "guardian of the genome" captures its core role: detecting damage to the DNA, halting the cell cycle to allow repair, and - if repair fails - triggering either senescence or apoptosis to eliminate the damaged cell.
Key structural facts:
- Transactivation domain (aa 1-93): binds MDM2/HDM2
- DNA-binding domain (aa 93-312): most mutations cluster here ("hot spots" at R248, R249, R175, etc.)
- Tetramerization domain (aa 307-355): p53 works as a homotetramer
- Negative regulatory domain (aa 356-393)
2. The p53 Pathway - Step by Step
Here is the mechanism, summarized visually:
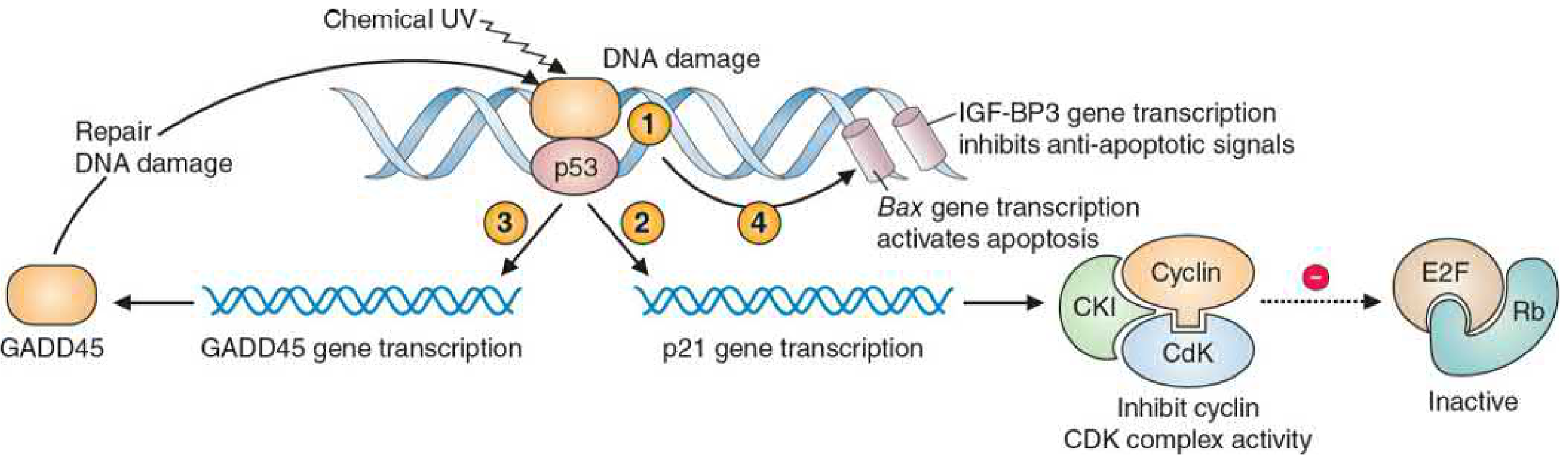
Figure: p53 and cell-cycle arrest pathway (Basic Medical Biochemistry, 6e, Fig. 17.10)
Step-by-step mechanism:
| Step | Event |
|---|---|
| Trigger | DNA damage from mutagens, UV, ionizing radiation, anoxia, oncogene activation |
| Sensing | ATM/ATR kinase complexes sense DNA double/single strand breaks |
| p53 stabilization | ATM/ATR phosphorylate p53, releasing it from MDM2/HDM2 (its ubiquitin ligase) - normally MDM2 constantly tags p53 for proteasomal degradation keeping levels low |
| p53 rises | Free, active p53 accumulates in the nucleus |
| Cell cycle arrest | p53 transcribes p21 (a CKI - cyclin-dependent kinase inhibitor) → p21 blocks cyclin-CDK complexes → Rb remains hypophosphorylated → E2F transcription factors stay inactive → cell cannot enter S phase (G1/S checkpoint blocked) |
| DNA repair | p53 also transcribes GADD45 (growth arrest and DNA damage gene) → DNA repair enzymes are recruited |
| If repaired | p53 activates the MDM2 gene → MDM2 protein re-degrades p53 → negative feedback restores normal cycle |
| If not repaired | p53 activates pro-apoptotic genes: Bax, Puma, Noxa, Apaf-1 (mitochondrial/intrinsic apoptosis) and Fas, TRAIL, TRAIL-R2 (death receptor/extrinsic apoptosis); also activates IGF-BP3 which blocks anti-apoptotic growth factor signaling |
| Senescence | Alternatively, p53 can trigger irreversible cell cycle arrest (senescence) |
"p53 is the central monitor of stress in the cell and can be activated by anoxia, inappropriate signaling by mutated oncoproteins, or DNA damage." - Robbins Pathologic Basis of Disease
3. MDM2 - The Key Regulator of p53
- MDM2 (mouse double minute 2, human homolog = HDM2) is the primary negative regulator of p53
- MDM2 is itself a transcriptional target of p53 - this creates an autoregulatory feedback loop
- MDM2 ubiquitinates p53 → marks it for proteasomal degradation → p53 half-life is very short (minutes) under normal conditions
- ATM phosphorylation of p53 disrupts the p53-MDM2 interaction → p53 is stabilized
- Clinical relevance: Some cancers overexpress MDM2 (gene amplified) as an alternative to mutating p53 itself - same net result (p53 inactivation)
4. p53 in Cancer - "Most Mutated Gene"
- >50% of all human cancers carry biallelic loss-of-function mutations in TP53 - the single most commonly mutated gene in cancer
- Follows the two-hit hypothesis (like Rb): both alleles must be inactivated
Mechanisms of p53 inactivation in cancer:
| Mechanism | Example |
|---|---|
| Point mutations in DNA-binding domain | Colorectal, lung, breast, bladder, etc. |
| Homozygous deletion | Colon, bladder cancers |
| MDM2 amplification/overexpression | Soft-tissue sarcomas (~30%) |
| Viral oncoprotein binding | HPV E6 binds p53 → ubiquitin degradation (cervical cancer) |
| Loss of ATM upstream | Ataxia-telangiectasia |
Common mutation "hot spots":
Point mutations H179L, R249W, and I255F are among the most frequent. Many mutant p53 proteins have increased half-lives and accumulate in tumor cells (gain-of-function mutations) - these mutant proteins can sometimes actively promote transformation.
5. Clinical Syndromes
Li-Fraumeni Syndrome
- Germline (inherited) heterozygous TP53 mutation
- Autosomal dominant, rare
- Very high lifetime cancer risk: sarcomas, breast cancer, brain tumors, leukemia, adrenocortical carcinoma (the "SBLA" cancers)
- Second-hit somatic mutation eliminates the remaining wild-type allele
Other cancers with prominent p53 mutation:
- Colorectal carcinoma - p53 mutation is a late event in the adenoma-carcinoma sequence
- Lung cancer - p53 mutation correlates with cigarette smoking (Goldman-Cecil Medicine)
- Cervical cancer - HPV E6 inactivation of p53
- Osteosarcoma - associated with RB1 and TP53 abnormalities (Li-Fraumeni)
- Uterine serous carcinoma - p53 overexpression (aberrant) is a defining molecular feature
6. p53 as a Transcription Factor - Key Target Genes
| Gene activated | Effect |
|---|---|
| p21 (CDKN1A) | Inhibits cyclin-CDK complexes → G1/S arrest |
| GADD45 | DNA repair |
| MDM2 | Negative feedback (p53 self-regulation) |
| Bax | Pro-apoptotic (BCL-2 family) |
| Puma / Noxa | Pro-apoptotic (BH3-only proteins) |
| Apaf-1 | Apoptosome formation |
| Fas / TRAIL-R2 | Death receptor pathway activation |
| IGF-BP3 | Blocks IGF-mediated survival signals |
| Autophagy regulators | Stress response (newly recognized role) |
7. p53 in the Lab / Diagnostics
From Henry's Clinical Diagnosis (clinical laboratory perspective):
- IHC (immunohistochemistry): Wild-type p53 is rapidly degraded and shows minimal/no nuclear staining. Mutant p53 accumulates → strong nuclear overexpression on IHC = surrogate for TP53 mutation (used in gynecologic oncology, especially uterine serous carcinoma and vulvar SCC)
- Serum anti-p53 antibodies: Detectable in cancer patients; their presence correlates with TP53 mutation. However, absence is not reassuring (homozygous deletions produce no p53 protein to generate antibodies)
- Serum p53 protein: Elevated in some cancers, but complex to interpret because different antibodies recognize different mutant forms
8. Oncogene vs. Tumor Suppressor - Where p53 Fits
| Feature | Oncogene | Tumor Suppressor (p53) |
|---|---|---|
| Alleles needed for effect | 1 (dominant) | 2 (both must be lost) |
| Effect | Gain-of-function → promotes growth | Loss-of-function → removes brakes |
| Inheritance | Somatic mutations only | Can be germline (Li-Fraumeni) |
| p53 classification | "Caretaker" and "Gatekeeper" gene |
Note: p53 is unusual - it functions as both a gatekeeper (regulates cell cycle and apoptosis) and a caretaker (preserves genomic integrity by coordinating DNA repair).
9. Summary Table
| Property | Detail |
|---|---|
| Gene | TP53, chromosome 17p13.1 |
| Protein | 393 aa, 53 kDa nuclear phosphoprotein |
| Function | Transcription factor, stress sensor, tumor suppressor |
| Active form | Homotetramer |
| Key activators | DNA damage, ATM/ATR kinases, oncogene activation, hypoxia |
| Key inhibitor | MDM2/HDM2 (ubiquitin ligase) |
| Main downstream effectors | p21, GADD45, Bax, Puma, MDM2 |
| Mutation frequency | >50% of all human cancers |
| Germline syndrome | Li-Fraumeni syndrome |
| Viral inactivation | HPV E6 protein |
| Cancer detection | IHC overexpression, serum anti-p53 antibodies |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Basic Medical Biochemistry 6e; Harper's Illustrated Biochemistry 32e; Scott-Brown's Otorhinolaryngology; Henry's Clinical Diagnosis and Management by Laboratory Methods; Goldman-Cecil Medicine; Katzung's Basic & Clinical Pharmacology 16e.
This is a shared conversation. Sign in to Orris to start your own chat.