Can u explain me action potential redting membrane potential in detail basics also and in cardia smooth skeletal muscles? I am preparing for fcps exam and i cant get it
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the material needed for a complete, detailed FCPS-level answer. Let me compose it:
Action Potential and Resting Membrane Potential - Complete Guide for FCPS
PART 1: RESTING MEMBRANE POTENTIAL (RMP)
What is it?
The resting membrane potential is the electrical potential difference across the cell membrane when the cell is NOT firing. By convention, it is expressed as the intracellular potential relative to extracellular (which is set at 0 mV).
- Neurons and skeletal muscle: -70 mV
- Ventricular myocytes / Purkinje fibers: -85 to -95 mV
- SA node / AV node: -50 to -60 mV (less negative)
The inside of the cell is negative relative to outside.
Why is the inside negative? - The ionic basis
The RMP is set up by two forces acting simultaneously:
| Ion | Conc. OUTSIDE | Conc. INSIDE | Equilibrium Potential |
|---|---|---|---|
| Na+ | 142 mEq/L | 14 mEq/L | +61 mV |
| K+ | 4 mEq/L | 140 mEq/L | -94 mV |
| Cl- | 104 mEq/L | 4 mEq/L | -90 mV |
| Ca2+ | 2.4 mEq/L | 0.0001 mEq/L | +132 mV |
The KEY concept: At rest, the membrane is far more permeable to K+ and Cl- than to Na+ or Ca2+. K+ dominates the resting potential.
- K+ wants to diffuse OUT (down its concentration gradient)
- As K+ leaves, it takes positive charge with it, making the inside more negative
- The inside gets negative enough to pull K+ back electrically
- The point where these two forces balance = the K+ equilibrium potential (-94 mV)
- The actual RMP (-70 mV) doesn't quite reach -94 mV because a small amount of Na+ leaks in, slightly depolarizing it
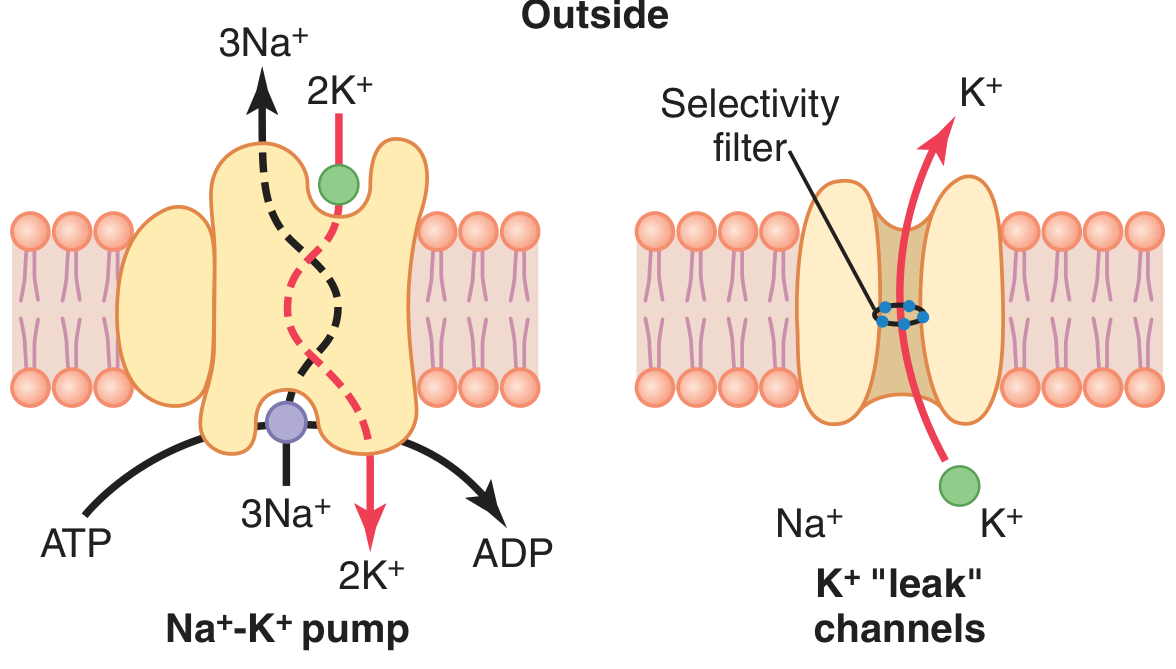
Role of the Na+-K+ ATPase pump
The Na+-K+ pump has two contributions to RMP:
- Direct (electrogenic): Pumps 3 Na+ OUT for every 2 K+ IN. This unequal exchange directly creates a small negative charge inside (-3 to -5 mV).
- Indirect (far more important): Maintains the concentration gradients for Na+ and K+ that drive the diffusion potentials. Without the pump, these gradients would run down and RMP would collapse.
The Goldman / Chord Conductance Equation
$$E_m = \frac{G_{K^+}}{G_T}E_{K^+} + \frac{G_{Na^+}}{G_T}E_{Na^+} + \frac{G_{Cl^-}}{G_T}E_{Cl^-} + \frac{G_{Ca^{2+}}}{G_T}E_{Ca^{2+}}$$
Each ion's contribution is weighted by its conductance. At rest, G(K+) >> G(Na+), so the RMP is pulled toward E(K+).
Source: Costanzo Physiology, 7th Ed.
PART 2: ACTION POTENTIAL - BASICS (Nerve/Skeletal Muscle)
Key Terminology (FCPS loves these!)
| Term | Definition |
|---|---|
| Depolarization | Membrane becomes LESS negative (Na+ rushes in) |
| Repolarization | Membrane returns to resting (K+ rushes out) |
| Hyperpolarization | Membrane becomes MORE negative than rest |
| Threshold | The voltage at which AP is inevitable (~-55 mV in nerve) |
| Overshoot | The portion where membrane potential goes POSITIVE (+35 mV) |
| Undershoot | The afterhyperpolarization below resting (-70 mV) |
| All-or-none | AP either fires fully or not at all |
Phases of the Nerve / Skeletal Muscle Action Potential
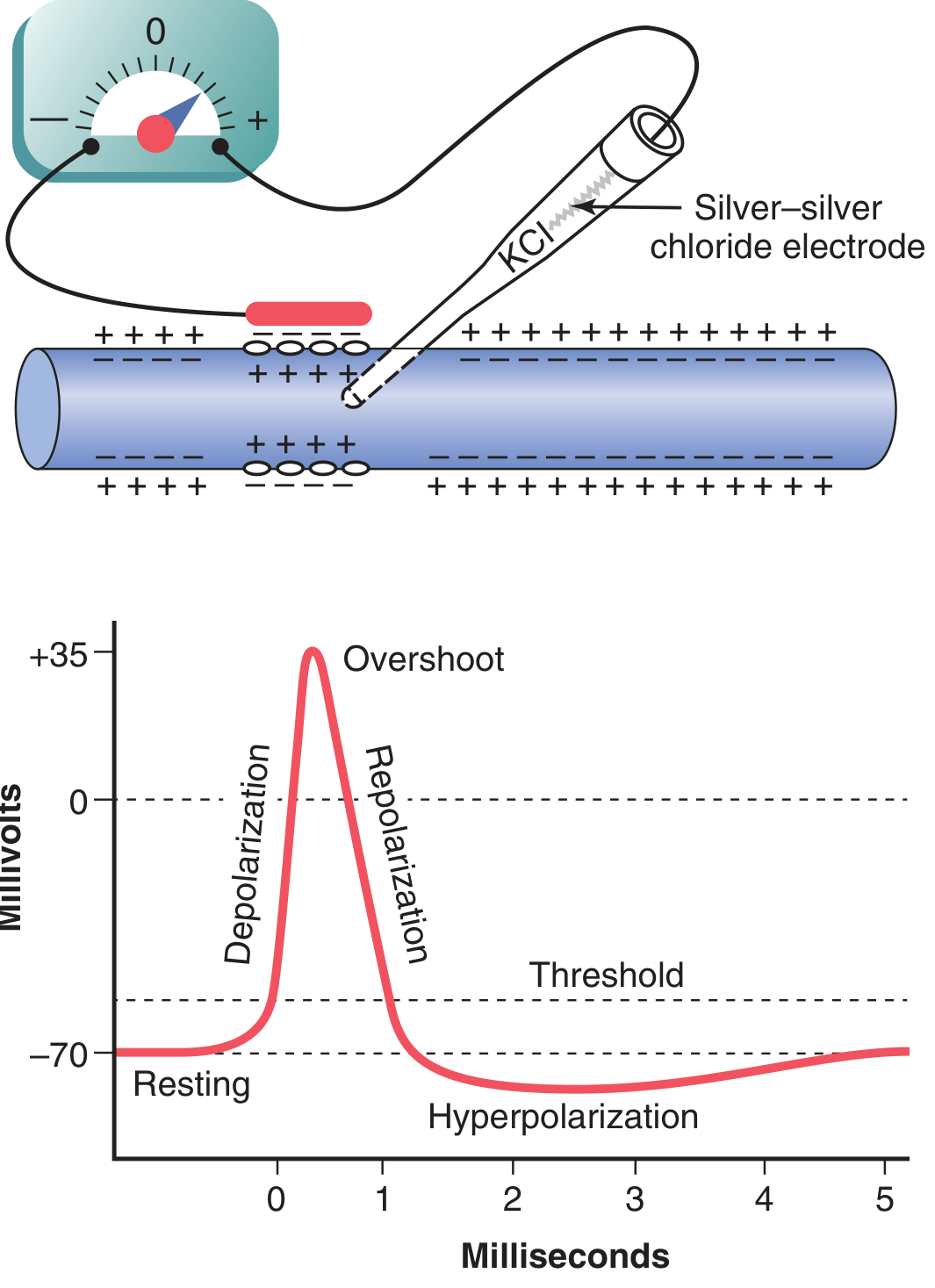
Phase 0 - Depolarization (upstroke):
- Stimulus brings membrane to threshold (~-55 mV)
- Voltage-gated Na+ channels open (activation gate opens)
- Na+ floods IN rapidly (inward current)
- Membrane potential shoots from -70 mV to +35 mV in <1 ms
- This is the "overshoot"
Phase 1 - Repolarization:
- Na+ channels start to INACTIVATE (inactivation gate closes)
- Voltage-gated K+ channels open (delayed rectifier)
- K+ rushes OUT (outward current)
- Membrane returns toward -70 mV
Phase 2 - Afterhyperpolarization (undershoot):
- K+ channels stay open slightly too long
- Membrane briefly dips BELOW -70 mV (more negative)
- This is called the undershoot or hyperpolarizing afterpotential
Recovery:
- K+ channels finally close
- Na+-K+ pump restores exact ion concentrations
- Membrane returns to -70 mV
Refractory Periods
| Period | When | What Happens | Clinical Meaning |
|---|---|---|---|
| Absolute Refractory Period (ARP) | During upstroke and most of repolarization | Na+ channels are INACTIVATED - can't open regardless of stimulus size | Cannot fire another AP - prevents re-entry; limits firing rate |
| Relative Refractory Period (RRP) | During afterhyperpolarization | Na+ channels are recovering; K+ conductance still elevated | Can fire AP but only with a STRONGER than normal stimulus |
PART 3: CARDIAC MUSCLE ACTION POTENTIAL
The cardiac AP is very different from nerve/skeletal muscle - it has 5 phases and lasts 200-400 ms (vs <2 ms for nerve). The reason: the plateau phase (phase 2) prevents re-excitation during contraction (like ARP).
The 5 Phases of Ventricular / His-Purkinje Action Potential
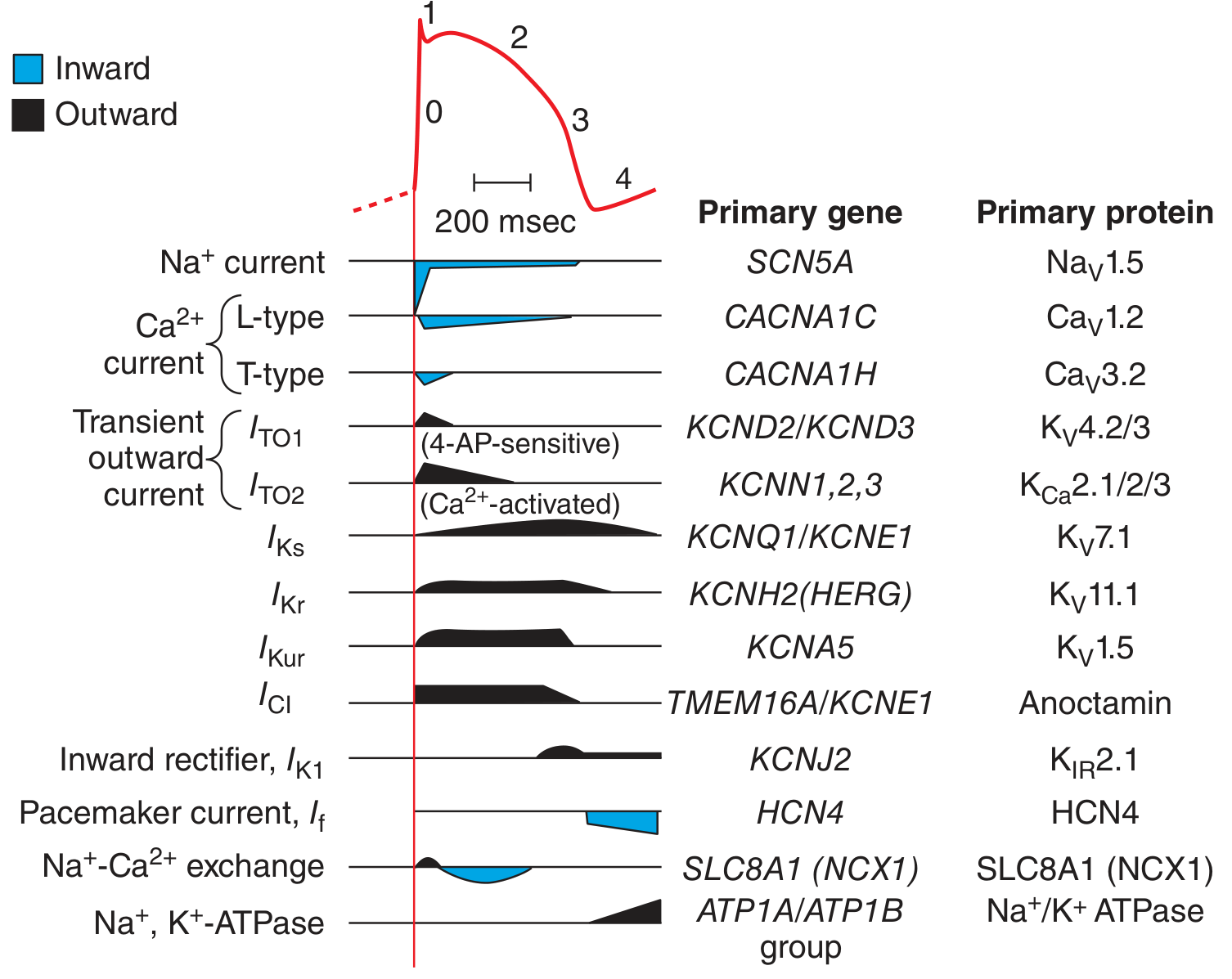
Phase 4 - Resting Membrane Potential (-85 to -95 mV):
- Maintained by the inwardly rectifying K+ channel (I_K1) - K+ leaks out, keeping the cell negative
- Stable in working atrial/ventricular myocytes (no spontaneous depolarization)
- The SA/AV node has a LESS negative RMP (-50 to -60 mV) because it has much less I_K1
Phase 0 - Rapid Depolarization (upstroke):
- Triggered by depolarization from an adjacent cell via gap junctions
- Voltage-gated fast Na+ channels (Nav1.5, encoded by SCN5A) open
- 10^7 Na+ ions/second rush in
- Membrane rapidly rises from -90 mV to +20 mV
- Na+ channels inactivate within ~1 ms
- The rate of rise (dV/dt = Vmax) determines conduction velocity
Phase 1 - Early Rapid Repolarization:
- Fast Na+ channels close (inactivated)
- Transient outward K+ current (I_to) activates - K+ moves out
- Small, brief repolarization creating the "notch" on the AP
Phase 2 - Plateau (the unique cardiac feature!):
- L-type Ca2+ channels (CaV1.2, CACNA1C) open - slow, sustained Ca2+ influx (inward)
- Slow K+ channels (I_Ks, I_Kr) provide a slow outward K+ current
- These two currents BALANCE each other, maintaining the plateau at ~0 mV for 200 ms
- This Ca2+ entering triggers more Ca2+ release from SR (calcium-induced calcium release = CICR)
- This is what causes excitation-contraction coupling in cardiac muscle
Phase 3 - Final Rapid Repolarization:
- L-type Ca2+ channels close (Ca2+ inflow stops)
- K+ channels (I_Ks, I_Kr, and I_K1 reactivates) open fully - rapid K+ efflux
- Membrane returns to -90 mV
SA Node Action Potential (Pacemaker AP)
The SA node is the pacemaker and has a fundamentally different AP:
- RMP is only -50 to -60 mV (much less negative)
- No stable phase 4 - it has spontaneous diastolic depolarization (the "funny current")
- No fast Na+ channels (they are inactivated at -55 mV, they need -90 mV to recover)
- Upstroke is driven by L-type Ca2+ channels - slow, making conduction velocity very slow (0.01-0.05 m/s)
Why does the SA node fire spontaneously? - The "Funny Current" (I_f):
- After each AP, HCN4 channels open - allow Na+ AND K+ to flow in
- This is a slow inward depolarizing current
- Called the pacemaker current - it gradually brings the membrane from -60 mV up to threshold
- Once threshold is reached, L-type Ca2+ channels open and fire the AP
FCPS exam tip: SA node AP uses Ca2+ for upstroke. Ventricular AP uses Na+ for upstroke. This is why Ca2+ channel blockers (verapamil, diltiazem) slow heart rate and AV conduction.
Comparison Table: Cardiac AP Types
| Feature | Ventricular / Purkinje | SA / AV Node |
|---|---|---|
| RMP | -85 to -95 mV | -50 to -60 mV |
| Upstroke (Phase 0) | Fast Na+ (Nav1.5) | L-type Ca2+ |
| dV/dt | Fast (200-1000 V/s) | Slow (1-10 V/s) |
| Conduction velocity | Fast (0.5-4 m/s) | Very slow (0.01-0.05 m/s) |
| Automaticity | None (stable Phase 4) | Yes (spontaneous Phase 4) |
| Effect of CCBs | Little on upstroke | Slows rate and conduction |
PART 4: SMOOTH MUSCLE ACTION POTENTIAL
Smooth muscle is the most variable and unique of the three - it can contract both with and without a formal action potential.
Key Features
- No troponin - regulation of contraction is via calmodulin, not troponin
- Two types:
- Multi-unit smooth muscle (iris, ciliary body, piloerector): each fiber contracts independently, controlled mainly by nerves - like skeletal muscle in its neural control
- Unitary (single-unit / visceral) smooth muscle (gut, uterus, ureters, blood vessels): cells are connected by gap junctions, contract as a syncytium, have spontaneous activity
Action Potential in Smooth Muscle
- The upstroke is carried by voltage-gated Ca2+ channels (NOT Na+ channels primarily)
- The AP is much slower than nerve or cardiac
- AP duration is variable - can be a simple spike, or can have a plateau
CRITICAL DIFFERENCE: In smooth muscle, sub-threshold depolarization (without a full AP) can still open voltage-gated Ca2+ channels enough to cause contraction. You do NOT always need a full AP.
Excitation-Contraction Coupling in Smooth Muscle
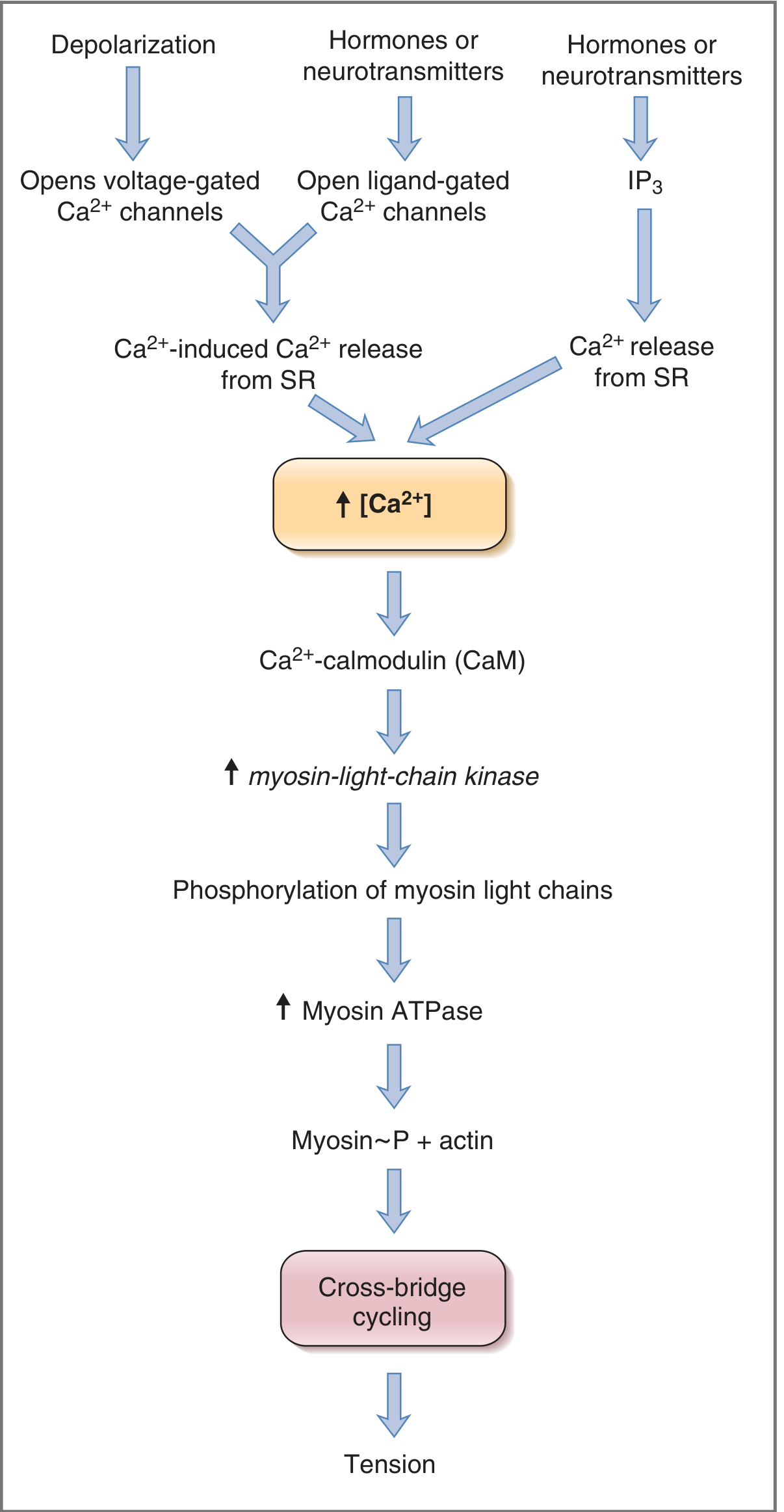
The steps:
- Depolarization (or hormones/neurotransmitters) → voltage-gated or ligand-gated Ca2+ channels open
- Ca2+ enters from ECF + Ca2+-induced Ca2+ release from SR → intracellular [Ca2+] rises
- Ca2+ binds calmodulin (4 ions cooperatively)
- Ca2+-calmodulin activates myosin-light-chain kinase (MLCK)
- MLCK phosphorylates myosin light chain → myosin head can now interact with actin
- Cross-bridge cycling → tension/contraction
Hormones and neurotransmitters can also trigger IP3 release, which opens IP3-gated Ca2+ channels on the SR - providing an additional Ca2+ source independent of membrane depolarization.
PART 5: COMPARISON TABLE - All Three Muscle Types
| Feature | Skeletal | Cardiac | Smooth |
|---|---|---|---|
| RMP | -70 to -90 mV | -85 to -95 mV (pacemaker: -55 mV) | -50 to -60 mV |
| Upstroke ion | Na+ (fast) | Na+ (fast, ventricular); Ca2+ (SA/AV node) | Ca2+ |
| AP duration | 1-2 ms | 200-400 ms | 50-300 ms (variable) |
| Plateau phase | No | Yes (Phase 2, Ca2+) | Sometimes |
| Automaticity | No | Yes (SA node) | Yes (some pacemaker cells, e.g., gut) |
| Ca2+ source for contraction | SR (ryanodine receptor, triggered by AP voltage) | SR + ECF entry (CICR) | ECF + SR (calmodulin pathway) |
| Contraction regulated by | Troponin-C | Troponin-C (+ calmodulin) | Calmodulin + MLCK |
| Gap junctions | No | Yes (intercalated discs) | Yes (unitary SM) |
| ARP covers | Most of AP | Entire contraction (protective) | Variable |
FCPS High-Yield Summary Points
- RMP is set mainly by K+ permeability - membrane is 100x more permeable to K+ at rest than to Na+
- Na+-K+ ATPase is electrogenic (3 Na+ out : 2 K+ in) but its main contribution is indirect - maintaining concentration gradients
- All-or-none law applies to nerve, skeletal, and cardiac muscle APs
- Cardiac Phase 2 plateau = L-type Ca2+ in = why cardiac AP is so long = why cardiac ARP covers the whole systole = why cardiac muscle cannot tetanize (protective!)
- SA node pacemaker fires because of I_f (funny current via HCN4) + T-type Ca2+ channels driving slow depolarization in phase 4
- SA node upstroke = Ca2+; Ventricular upstroke = Na+ - this is tested constantly
- Smooth muscle has NO troponin - uses calmodulin-MLCK pathway
- Smooth muscle can contract without a formal AP - subthreshold depolarization + hormones via IP3 are sufficient
- Conduction velocity: Purkinje > atrial > ventricular > AV node (AV node is slowest = AV delay = allows ventricles to fill)
- ARP of cardiac muscle = why you cannot give a tetanic stimulus to the heart - it cannot fuse contractions
Sources: Guyton and Hall Textbook of Medical Physiology, Costanzo Physiology 7th Ed., Braunwald's Heart Disease, Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.