Stages of cervical cancer
Reading File
search_medical_text
cervical cancer FIGO staging classification
search_medical_image
cervical cancer stages diagram
GradeResponse
GradeResponse
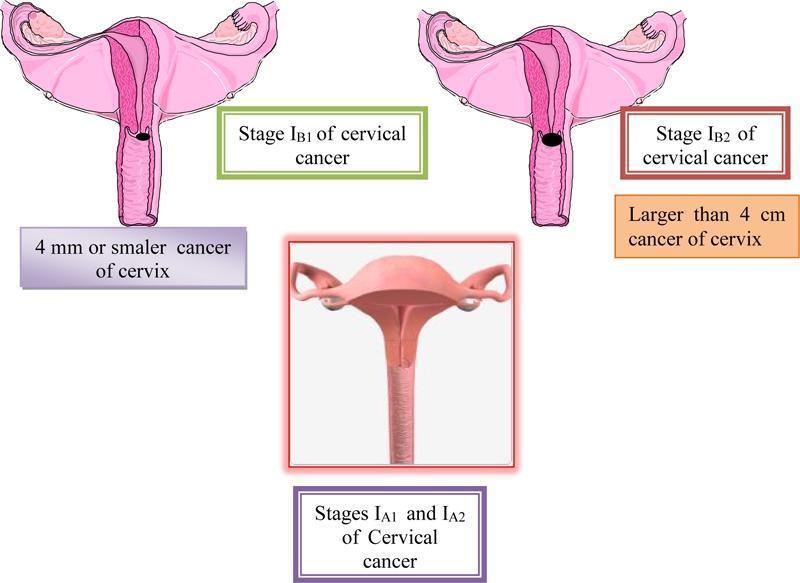
Stages of Cervical Cancer (FIGO 2018 Classification)
Cervical cancer is staged using the FIGO (International Federation of Gynecology and Obstetrics) system, revised in 2018. Staging is based on tumor size, local extension, lymph node involvement, and distant metastasis — and can incorporate imaging and pathological findings.
Stage I — Tumor Confined to the Cervix
| Sub-stage | Description |
|---|---|
| IA | Microscopic invasive carcinoma (diagnosed only by microscopy) |
| IA1 | Stromal invasion < 3 mm depth |
| IA2 | Stromal invasion ≥ 3 mm and < 5 mm depth |
| IB | Clinically visible lesion confined to cervix, or microscopic > Stage IA |
| IB1 | Invasive carcinoma ≤ 2 cm in greatest dimension |
| IB2 | Invasive carcinoma > 2 cm and ≤ 4 cm |
| IB3 | Invasive carcinoma > 4 cm |
Stage II — Tumor Extends Beyond the Cervix but Not to Pelvic Wall or Lower Third of Vagina
| Sub-stage | Description |
|---|---|
| IIA | Extension to the upper 2/3 of the vagina, no parametrial invasion |
| IIA1 | Tumor ≤ 4 cm |
| IIA2 | Tumor > 4 cm |
| IIB | Parametrial invasion, but not to pelvic wall |
Stage III — Tumor Extends to Pelvic Wall and/or Lower Vagina, or Causes Hydronephrosis
| Sub-stage | Description |
|---|---|
| IIIA | Involves lower third of vagina, no extension to pelvic wall |
| IIIB | Extension to pelvic wall and/or hydronephrosis or non-functioning kidney |
| IIIC | Regional lymph node metastasis (regardless of tumor size/extent) |
| IIIC1 | Pelvic lymph node metastasis |
| IIIC2 | Para-aortic lymph node metastasis |
FIGO 2018 update: Stage IIIC was newly added to incorporate lymph node status, previously not included in clinical staging. Imaging (CT, MRI, PET) or pathology can be used to assign IIIC.
Stage IV — Tumor Invades Adjacent Organs or Distant Metastasis
| Sub-stage | Description |
|---|---|
| IVA | Invasion of bladder or rectal mucosa (biopsy confirmed) |
| IVB | Distant metastasis (including peritoneum, lungs, liver, bones) |
Key Prognostic Considerations
- Histology: Squamous cell carcinoma is most common (~70%), followed by adenocarcinoma. Prognosis is more strongly influenced by tumor size, extent, and lymph node involvement than by histology alone.
- Lymph node involvement (Stage IIIC): Significantly worsens prognosis even when the primary tumor appears localized.
- 5-year survival rates approximate: Stage I ~80–95%, Stage II ~60–75%, Stage III ~30–50%, Stage IV ~5–15%.
Treatment Overview by Stage
| Stage | Primary Treatment |
|---|---|
| IA1 (no LVSI) | Cone biopsy or simple hysterectomy |
| IA1–IB1 | Radical hysterectomy ± pelvic lymph node dissection, or definitive radiotherapy |
| IB2–IIB | Concurrent cisplatin-based chemoradiation |
| III–IVA | Concurrent chemoradiation ± brachytherapy |
| IVB | Systemic chemotherapy ± immunotherapy (e.g., pembrolizumab) |
Staging directly guides treatment planning and predicts outcomes. Imaging (MRI preferred for local extent, PET-CT for nodal/distant disease) is integral to modern staging despite FIGO historically relying on clinical examination.
This is a shared conversation. Sign in to Orris to start your own chat.