Explain me antianginal drugs its mechanism of action and side effects with diagrams
Reading File
Finding Sources
Finding Sources
Searching Images
antianginal drugs mechanism of action diagram
Reading File
Finding Sources
Finding Sources
Searching Images
nitrates mechanism of action angina nitric oxide vascular smooth muscle
Reading File
Reading File
Searching Images
calcium channel blockers mechanism angina heart vascular
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Searching Images
antianginal drugs beta blockers angina pectoris mechanism pharmacology diagram
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information and diagrams needed for a comprehensive answer. Let me compile the complete response.
Antianginal Drugs: Mechanisms of Action & Side Effects
Angina pectoris results from an imbalance between myocardial oxygen demand and supply. Antianginal drugs work either by reducing oxygen demand (beta-blockers), increasing supply (nitrates, calcium channel blockers), or both.
Pathophysiology of Angina — The Basis of Drug Action
Three main types:
- Effort (stable) angina — atherosclerotic obstruction → ↑ demand exceeds fixed supply
- Vasospastic (Prinzmetal) angina — coronary vasospasm → ↓ supply
- Unstable angina (ACS) — plaque rupture + thrombus → ↓ supply acutely
Class 1: Organic Nitrates
Drugs: Nitroglycerin (GTN), Isosorbide dinitrate (ISDN), Isosorbide mononitrate (ISMN), Amyl nitrite
Mechanism of Action
Figure 12-1 — How vascular smooth muscle contraction and relaxation works (CCBs block Ca²⁺ influx; cGMP causes relaxation):
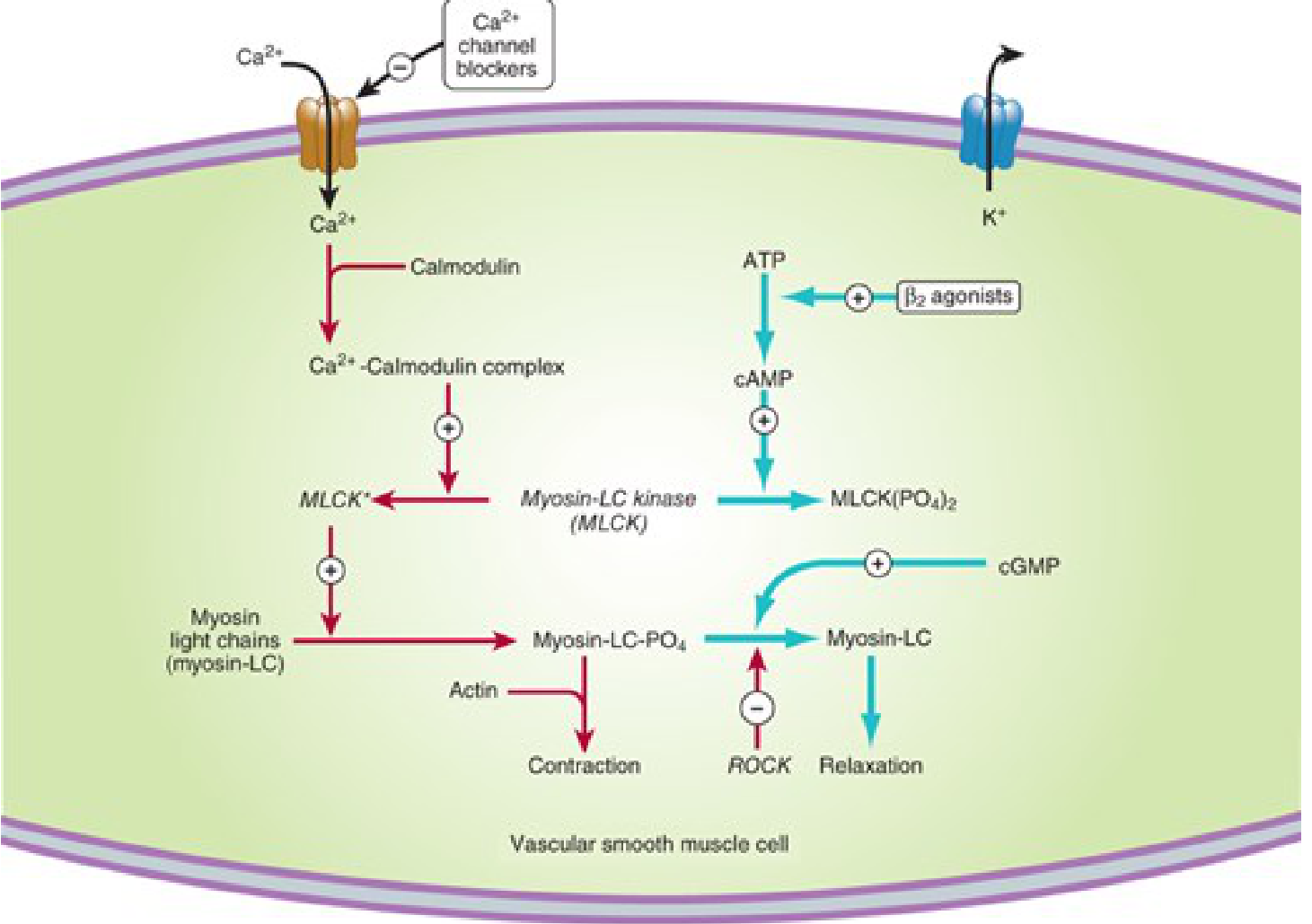
Figure 12-2 — The nitrate/NO mechanism in vascular smooth muscle:
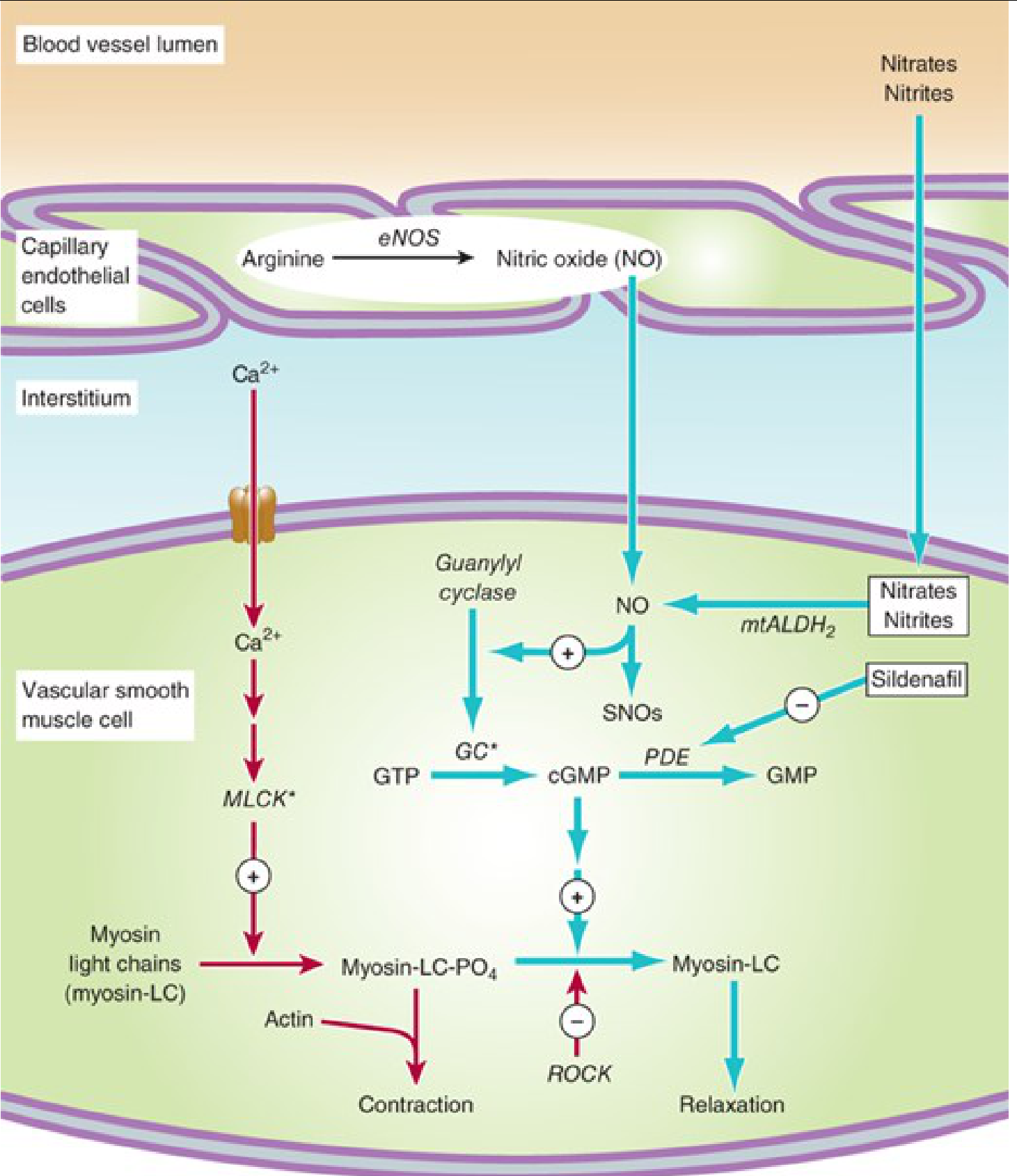
Step-by-step:
- Nitrates undergo bioactivation via mitochondrial aldehyde dehydrogenase-2 (mtALDH2) → release free nitrite → converted to nitric oxide (NO)
- NO activates guanylyl cyclase → GTP → ↑ cGMP
- cGMP activates protein kinase G → dephosphorylates myosin light chains → vascular smooth muscle relaxation
- Endothelium also produces NO via eNOS from L-arginine
Hemodynamic effects in angina:
| Effect | Result |
|---|---|
| Venodilation (large veins) | ↓ Preload (venous return) → ↓ LVEDV → ↓ O₂ demand |
| Arterial dilation | ↓ Afterload → ↓ wall stress → ↓ O₂ demand |
| Coronary dilation | ↑ O₂ supply, ↑ collateral flow; prevents/relieves spasm |
| ↓ Cardiac output | ↓ O₂ demand overall |
The dominant antianginal mechanism is reduction of oxygen demand via decreased preload and afterload. In vasospastic angina, prevention of coronary artery spasm is paramount.
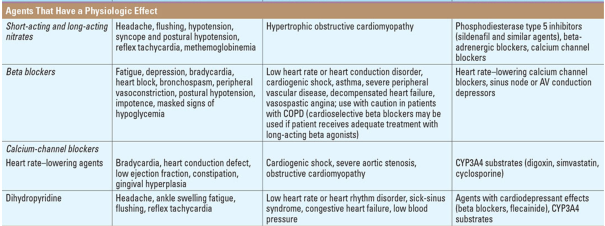
Side Effects
- Headache (most common — from cerebral vasodilation)
- Reflex tachycardia (baroreceptor response to ↓ BP)
- Postural hypotension / syncope
- Flushing
- Methemoglobinemia (rare, high doses)
- Nitrate tolerance — develops within 24h of continuous use; requires nitrate-free interval (8–12 h/day)
- Contraindicated with PDE-5 inhibitors (sildenafil, tadalafil) — severe refractory hypotension
- Contraindicated in hypertrophic obstructive cardiomyopathy, right ventricular infarction, severe aortic stenosis
Preparations & Routes
| Preparation | Route | Onset | Duration | Use |
|---|---|---|---|---|
| Nitroglycerin (sublingual) | SL | 1–3 min | 15–30 min | Acute relief |
| Nitroglycerin (IV) | IV | Immediate | During infusion | Unstable angina, HTN |
| ISDN | Oral/SL | 15–30 min | 4–6 h | Prophylaxis |
| ISMN | Oral | 30–60 min | 6–8 h | Prophylaxis (100% bioavailability) |
| GTN patch | Transdermal | 30–60 min | 24 h | Prophylaxis |
Class 2: Beta-Adrenoceptor Blockers (β-Blockers)
Drugs: Propranolol, Metoprolol, Atenolol, Bisoprolol, Carvedilol (also α-blocker), Nebivolol
Mechanism of Action
β-Blockers are not vasodilators (except carvedilol, nebivolol), but are the first-line prophylactic treatment for effort angina.
At β₁-receptors in the heart:
- ↓ Heart rate (negative chronotropy) → ↑ diastolic filling time → ↑ coronary perfusion time
- ↓ Myocardial contractility (negative inotropy)
- ↓ Conduction velocity (AV node)
Net effect: ↓ Myocardial oxygen demand at rest AND during exercise
β-Blockers reduce the "triple product" (HR × systolic BP × contractility), which is the main determinant of myocardial O₂ consumption.
Lower heart rate is particularly beneficial: coronary perfusion occurs mainly in diastole, so bradycardia prolongs perfusion time.
Side Effects
| Side Effect | Mechanism |
|---|---|
| Bradycardia / AV block | β₁ blockade |
| Fatigue, impaired exercise tolerance | ↓ Cardiac output |
| Bronchospasm | β₂ blockade (avoid non-selective in asthma/COPD) |
| Peripheral vasoconstriction | β₂ blockade → unopposed α |
| Worsening claudication | Peripheral vasoconstriction |
| Erectile dysfunction | |
| Masked hypoglycemia signs | (use with caution in diabetics on insulin) |
| Depression, insomnia, vivid dreams | CNS effects (lipophilic agents — propranolol) |
| Rebound angina on sudden withdrawal |
Contraindications
Acute decompensated heart failure, significant bradycardia, 2nd/3rd degree AV block, severe reactive airway disease, vasospastic (Prinzmetal) angina (may worsen spasm by unopposed α stimulation), cardiogenic shock.
Class 3: Calcium Channel Blockers (CCBs)
Drugs: Dihydropyridines: Nifedipine, Amlodipine, Felodipine | Non-DHPs: Verapamil, Diltiazem
Mechanism of Action
CCBs block voltage-gated L-type calcium channels — the dominant channel in cardiac and vascular smooth muscle.
Binding sites:
- Dihydropyridines (e.g., nifedipine) → bind α₁ subunit (one site)
- Verapamil & Diltiazem → bind related but distinct regions of α₁ subunit
The drugs bind from the inner side of the membrane, preferentially to open and inactivated channels (state-dependent block), reducing frequency of channel opening → ↓ Ca²⁺ influx.
Consequences by tissue:
| Tissue | Effect |
|---|---|
| Vascular smooth muscle | Relaxation → vasodilation → ↓ afterload |
| Coronary arteries | Dilation → relieves/prevents spasm |
| Heart (DHPs — minimal at therapeutic doses) | Modest ↓ contractility |
| Heart (verapamil/diltiazem) | ↓ SA node rate, ↓ AV conduction, ↓ contractility |
Dihydropyridines are predominantly vascular; verapamil and diltiazem have significant cardiac effects.
Side Effects
Dihydropyridines (nifedipine, amlodipine):
- Headache, flushing, dizziness (vasodilation)
- Ankle edema (arteriolar dilation without venodilation)
- Reflex tachycardia (especially short-acting nifedipine — dangerous in ACS)
- Gingival hyperplasia
Verapamil:
- Constipation (most common)
- Bradycardia, AV block
- ↓ Contractility (worsens heart failure)
- Raises digoxin levels (pharmacokinetic interaction)
Diltiazem:
- Bradycardia, AV block (less than verapamil)
- ↓ Contractility
- Relatively better tolerated
Class Contraindications:
- Verapamil/Diltiazem: severe LV dysfunction, bradycardia, AV block, concomitant β-blockers (additive AV block), cardiogenic shock
- Short-acting dihydropyridines: unstable angina / acute MI (↑ adverse cardiac events)
Class 4: Newer Antianginal Drugs
Ranolazine
- Mechanism: Inhibits the late inward sodium current (I_Na(late)) → prevents intracellular Na⁺ overload → prevents secondary Ca²⁺ overload (via Na⁺/Ca²⁺ exchanger) → ↓ diastolic wall tension and O₂ demand. Does not significantly lower HR or BP.
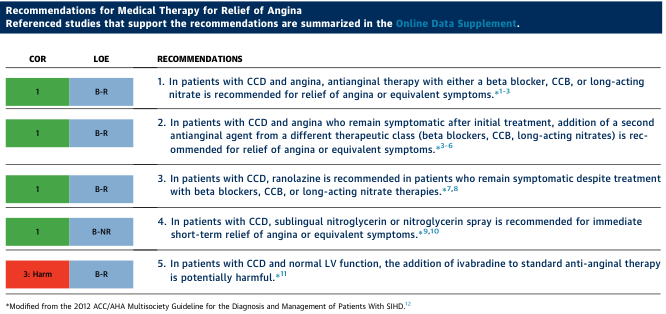
- Indications: Add-on therapy for chronic stable angina refractory to other agents (ACC/AHA Class I recommendation)
- Side effects: Dizziness, headache, constipation, nausea; prolongs QTc (contraindicated in pre-existing QT prolongation)
Ivabradine
- Mechanism: Selectively blocks the I_f (funny current) in SA node → reduces heart rate without affecting contractility or BP
- Indications: Symptomatic stable angina in patients with sinus rhythm and HR ≥70 bpm who cannot tolerate β-blockers. ACC/AHA notes it is potentially harmful as add-on to standard therapy in normal LV function.
- Side effects: Luminous phenomena (phosphenes — transient visual brightness), bradycardia, atrial fibrillation
Nicorandil
- Mechanism: Dual — activates K⁺-ATP channels (coronary dilation) + has nitrate-like component (venodilation)
- Used in Europe/Asia; not FDA-approved in USA
Trimetazidine
- Mechanism: Metabolic modulator — inhibits fatty acid β-oxidation → shifts myocardial metabolism to glucose → more O₂-efficient energy production
- Side effects: Extrapyramidal symptoms (parkinsonism), dizziness
- Not available in USA
Comparison of Antianginal Effects
| Parameter | Nitrates Alone | β-Blockers/CCBs Alone | Combined |
|---|---|---|---|
| Heart rate | ↑ (reflex) | ↓ | ↓ |
| Arterial pressure | ↓ | ↓ | ↓ |
| End-diastolic volume | ↓ | ↑ | None/↓ |
| Contractility | ↑ (reflex) | ↓ | None |
| Ejection time | ↓ | ↑ | None |
From Katzung's Basic and Clinical Pharmacology, 16th Ed., Table 12-3
Combination rationale: β-Blockers counteract the reflex tachycardia and increased contractility caused by nitrates; nitrates counteract the increased preload and end-diastolic volume caused by β-blockers. This complementary pharmacology makes them superior in combination.
Drug Selection by Angina Type
| Angina Type | First-Line | Second-Line | Avoid |
|---|---|---|---|
| Stable/Effort angina | β-Blockers + long-acting nitrates | CCBs | — |
| Vasospastic (Prinzmetal) | Nitrates + CCBs | — | β-Blockers |
| Unstable angina | IV nitroglycerin + β-blockers + antiplatelet | CCBs (add-on) | Short-acting DHPs |
| Refractory stable angina | Add ranolazine | Add ivabradine (if HR ≥70) | — |
Clinical Guidance Summary (Harrison's / ACC/AHA Guidelines)
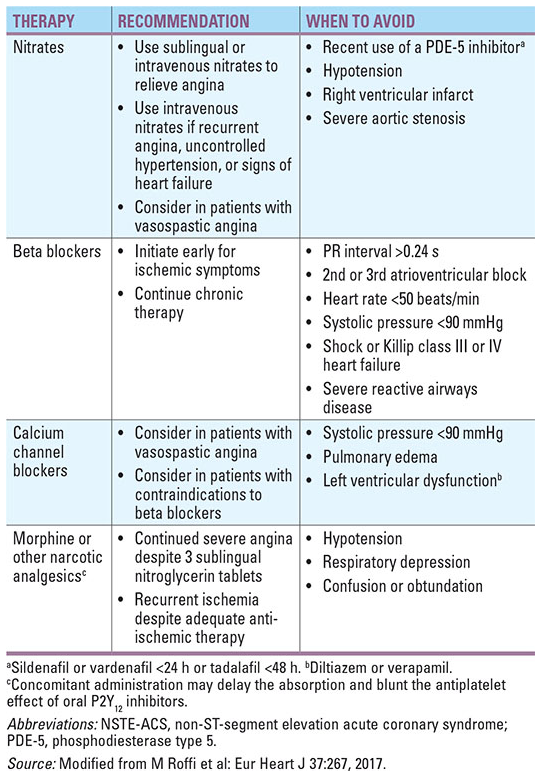
Key Pearls
- Nitrates + PDE-5 inhibitors (sildenafil) → absolute contraindication (severe hypotension, potentially fatal). Wait ≥24 h after sildenafil, ≥48 h after tadalafil before giving nitrates.
- Never abruptly stop β-blockers in angina — rebound ischemia/MI risk.
- Short-acting nifedipine is contraindicated in ACS — causes reflex tachycardia and worsens outcomes.
- Verapamil + β-blockers → risk of complete heart block and severe LV depression — avoid combination.
- Tolerance to nitrates develops within 24 hours of continuous exposure. A nitrate-free interval of 8–12 hours is essential.
- Ranolazine is uniquely effective without hemodynamic effects — ideal for patients who cannot tolerate rate-lowering drugs.
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed. | Harrison's Principles of Internal Medicine, 21st Ed. | ACC/AHA 2023 Chronic Coronary Disease Guideline
This is a shared conversation. Sign in to Orris to start your own chat.