recent advances in automation in clinical pathology
automation clinical pathology laboratory
recent advances automation clinical pathology laboratory 2024 2025
PMID: 39053633
PMID: 40307127
https://clpmag.com/lab-essentials/lab-automation/automation-…
total laboratory automation clinical chemistry robotics
digital pathology whole slide imaging artificial intelligence
PMID: 38704465
automated hematology analyzer machine learning CBC morphology
laboratory automation preanalytical error reduction turnaround time
PMID: 41750668
Recent Advances in Automation in Clinical Pathology
1. Total Laboratory Automation (TLA)
- Automated specimen input and bar-code / RFID tracking at every routing decision point
- Automated centrifuges (self-balancing, refrigerated or ambient)
- Decapper and recapper stations
- Level detection and specimen integrity checking (hemolysis, lipemia, icterus - often spectrophotometric at multiple wavelengths)
- Aliquot modules and automated diluters
- Refrigerated storage and retrieval units
- Autoverification middleware using rules-based logic to release results without technologist intervention
- Autoretrieval for reflex and repeat testing
2. Collaborative Robotics (Cobots) and Autonomous Mobile Robots (AMRs)
- Cobots (collaborative robots): Work safely alongside humans with sub-millimeter precision for fine-motor tasks such as colony picking, tube manipulation, and bench-level specimen handling - tasks that fixed conveyor lines cannot reach.
- Autonomous Mobile Robots (AMRs): Navigate hospital corridors autonomously to transport pathology carts, specimens, and medical supplies. Diligent Robotics' "Moxi" AMR has completed hundreds of thousands of supply deliveries in real hospital settings.
- Hybrid ecosystems: TLA "islands" are increasingly connected by cobotic workcells and AMRs, orchestrated by AI-enabled middleware, creating a modular rather than monolithic architecture.
3. Digital Pathology and Whole Slide Imaging (WSI)
- Multiple FDA-approved WSI scanners and image management systems (DICOM-based) are now operational
- New CPT codes for digital pathology facilitate billing and reimbursement
- Modern LIS platforms must handle DICOM WSI, integrate AI algorithms in an auditable/compliant manner, and support hybrid glass-plus-digital workflows
4. Artificial Intelligence in Pathology
a) Morphologic Diagnosis Automation
- Prostate cancer grading (Gleason scoring)
- Colorectal cancer detection
- Cervical cytology screening programs
b) Hematology - Automated Differential and Cell Classification
c) Foundation Models and Generative AI
d) AI for Oncology Biomarker Discovery
- Automated tumor detection and classification
- Identification of prognostic molecular biomarkers from H&E slides (without requiring IHC or molecular testing)
- Prediction of treatment response and patient outcomes
- Multi-omics integration for patient stratification
5. Laboratory Information Systems (LIS) - From Records to Action
- AI-first, cloud-native LIS: Moving from compliance-driven systems to AI-first architectures with cloud deployment and advanced interoperability
- Embedded AI agents: Clinisys CLS v2025.2 introduced an AI chat support agent (CLS CARE) with multilingual guidance built directly into the LIS environment
- TEFCA alignment and QHIN integration: Labs connecting to national interoperability networks for value-based care and public health reporting
- Orchestration layer: The LIS is now the human-plus-AI pathology orchestration hub, managing DICOM images, AI algorithm outputs, audit trails, and hybrid workflows
- Global LIS market estimated at ~$891 million in 2024, projected to reach ~$1.3 billion by 2032
6. Preanalytical Quality and Error Reduction
7. Microbiology and Molecular Diagnostics
- MALDI-TOF MS for rapid microbial identification is now standard
- Automated blood culture systems (e.g., BD BACTEC, bioMérieux BacT/ALERT) continuously monitor and flag positive cultures
- COPAN's WASP/WASPLab platforms automate plating, streaking, incubation, and imaging of culture plates - combined with AI for automated colony recognition and presumptive identification
- Next-generation sequencing (NGS) workflows are increasingly automated, with pool-to-pool testing and bioinformatic pipelines integrated into LIS platforms
Summary Table
| Domain | Key Advance (2023-2026) |
|---|---|
| TLA / Physical Automation | Cobots + AMRs extending beyond fixed tracks; hybrid ecosystems |
| Digital Pathology | FDA-cleared WSI, CPT reimbursement, remote sign-out |
| AI - Morphology | Foundation models, >96% sensitivity in meta-analyses |
| AI - Oncology | Molecular biomarker prediction from H&E slides |
| Hematology | Automated digital differentials, ML-based reflex rules |
| LIS/Middleware | AI-first cloud-native, TEFCA interoperability, AI chat agents |
| Preanalytical | RFID tracking, automated integrity checks, cobot specimen handling |
| Microbiology | COPAN automated culture imaging + AI colony recognition |
- Mukherjee S et al. Diagnostics 2026 - Cobots, AMRs, TLA [PMID 41750668]
- Marra A et al. Ann Oncol 2025 - AI in oncology pathology [PMID 40307127]
- Zhang DY et al. Lab Invest 2024 - Digital pathology implementation [PMID 39053633]
- McGenity C et al. npj Digit Med 2024 - AI diagnostic accuracy meta-analysis [PMID 38704465]
- Tietz Textbook of Laboratory Medicine, 7th Ed., pp. 879-880 (TLA systems)
- Henry's Clinical Diagnosis and Management by Laboratory Methods (TLA chapter)
Recent trends in the diagnosis, differential diagnosis of small round cell tumours
small round cell tumour diagnosis differential molecular classification
small round cell tumours recent advances diagnosis differential 2024 2025 molecular pathology
PMID: 38280658
PMID: 39510958
PMID: 41886300
PMID: 38315310
PMID: 41167264
PMID: 41615867
desmoplastic small round cell tumor DSRCT molecular diagnosis EWSR1-WT1
CIC rearranged sarcoma BCOR sarcoma diagnosis pathology
next generation sequencing RNA fusion sarcoma diagnosis bone soft tissue
PMID: 39576278
PMID: 40716917
NUT carcinoma SMARCA4 deficient undifferentiated tumor diagnosis immunohistochemistry
Recent Trends in the Diagnosis and Differential Diagnosis of Small Round Cell Tumours (SRCTs)
Overview
Classic Histology
1. The WHO 2020 Framework: Undifferentiated Small Round Cell Sarcomas (USRCS)
| WHO 5th Ed. Entity | Molecular Hallmark | Key IHC |
|---|---|---|
| Ewing sarcoma | EWSR1-ETS fusions (EWSR1-FLI1 ~85%, EWSR1-ERG ~10%) | CD99 (diffuse membranous), NKX2.2, FLI1 |
| CIC-rearranged sarcoma | CIC-DUX4 (most common), CIC-FOXO4 fusions | WT1, ETV4, DUX4, CD99 (focal/weak) |
| Sarcoma with BCOR genetic alterations | BCOR-CCNB3 (most common); BCOR ITD | BCOR, CCNB3 (in BCOR-CCNB3), CD99 (variable) |
| Round cell sarcoma with EWSR1-non-ETS fusions | EWSR1/FUS::NFATc2; EWSR1::PATZ1 | CD99 variable; NFATc2 (nuclear) |
- Robbins & Kumar Basic Pathology, p. 786; Quick Compendium of Clinical Pathology, p. 411
2. Entity-by-Entity Features and Diagnostic Advances
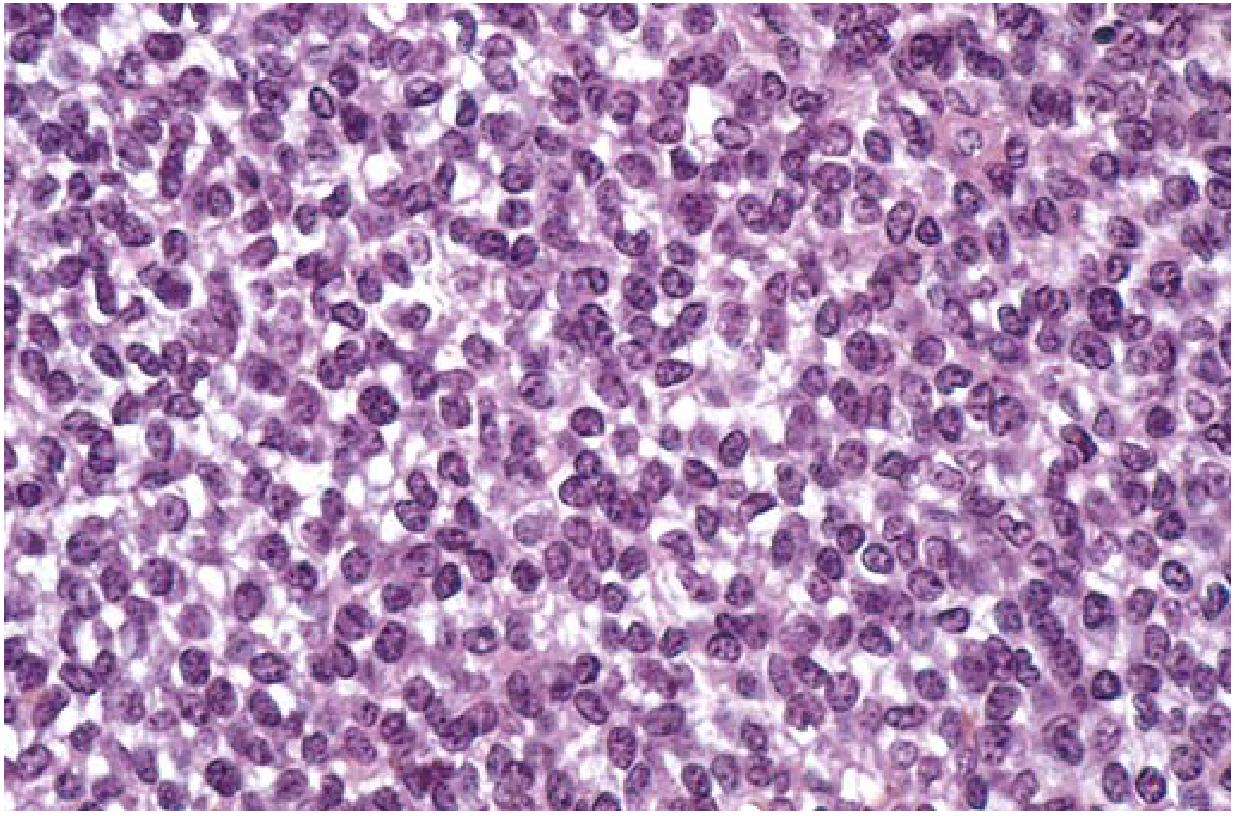
2.1 Ewing Sarcoma
- Morphology: Sheets of small round cells, slightly larger than lymphocytes, scant clear glycogen-rich cytoplasm; Homer-Wright rosettes (pseudorosettes with a central fibrillary core) in ~10%
- Molecular: >90% carry EWSR1::FLI1 t(11;22)(q24;q12); rarer partners include ERG, FEV, ETV1, ETV4. EWSR1 is on 22q12, highly prone to rearrangement
- IHC panel: CD99 (diffuse strong membranous - hallmark but not specific), NKX2.2 (nuclear, more specific than CD99), FLI1 (nuclear), vimentin+; keratin/desmin/S100 negative
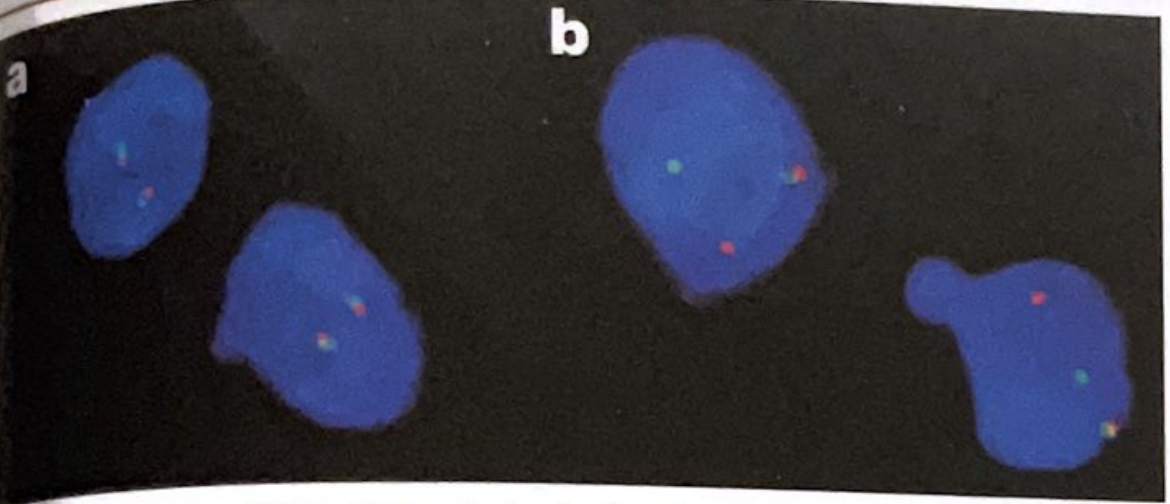
- FISH: EWSR1 break-apart probe (dual-colour) is the standard confirmatory test (see image below); note the separate red and green signals in rearranged nuclei
- Pitfall: EWSR1 FISH is positive in many non-Ewing tumours (DSRCT, clear cell sarcoma, myxoid liposarcoma); it is a "rule-in for EWSR1 rearrangement," not specific for Ewing
- Imaging (2026 update): Lytic "moth-eaten" bone destruction with aggressive periosteal reaction (onion-skin), large extraosseous soft tissue mass (Mori et al., RadioGraphics 2026, PMID 41886300)
- Prognosis: 75% 5-year survival with neoadjuvant chemotherapy + surgery ± radiation
2.2 CIC-Rearranged Sarcoma
- Demographics: Predominantly young adults; predominantly soft tissue (rarely bone)
- Morphology: Slightly larger cells than Ewing, more irregular nuclei, geographic necrosis, myxoid stroma; sometimes spindled cells
- Key IHC: WT1 (nuclear - useful), ETV4 (nuclear - highly sensitive), DUX4 (nuclear); CD99 is focal or absent (key distinguishing feature from Ewing)
- Molecular: CIC-DUX4 rearrangement (CIC on 19q13, DUX4 on 4q35 or 10q26) detected by FISH or RNA-seq fusion panels
- Prognosis: More aggressive than Ewing sarcoma; poor response to standard Ewing chemotherapy - an important clinical reason to distinguish it (Mori et al., RadioGraphics 2026)
- Imaging: Well-circumscribed lobulated soft tissue masses with extensive internal necrosis and haemorrhage, no calcification
2.3 Sarcoma with BCOR Genetic Alterations
- Two main subtypes:
- BCOR-CCNB3: X-linked inversion (inv X(p11;p13)), predominantly adolescent boys, long bone metaphyses/pelvis
- BCOR internal tandem duplication (ITD): Overlaps with infantile fibrosarcoma
- Morphology: Primitive round to spindle cells; myxoid stroma; occasional whorling
- Key IHC: BCOR (nuclear), CCNB3 (nuclear, specific for BCOR-CCNB3 subtype), CD99 (variable), TLE1 (nuclear)
- Imaging: Osteolytic or sclerotic lesion in long bones/pelvis, often with calcification in extraosseous component - helps distinguish from Ewing
- Prognosis: Potentially more favourable than Ewing; still benefits from Ewing-type chemotherapy regimens (Mori et al., 2026)
2.4 EWSR1/FUS::NFATc2 and EWSR1::PATZ1 Sarcomas (Newly Recognised)
- EWSR1 or FUS fuses with NFATc2 (transcription factor)
- Morphologically overlaps with Ewing but shows unique features including lobulated architecture and fibromyxoid stroma
- NFATc2 IHC (nuclear) serves as a surrogate marker
- Limited response to neoadjuvant chemotherapy compared with Ewing - critical for management
- Distinct methylation, transcriptomic, and epigenetic profile from Ewing sarcoma
- Definitive diagnosis requires NGS-based fusion detection
3. The Broader SRCT Differential
3.1 Desmoplastic Small Round Cell Tumour (DSRCT)
- Hallmark: Growth within strikingly desmoplastic stroma - the most distinctive morphologic clue
- Demographics: Adolescent/young adult males; intra-abdominal/peritoneal most common; rare sites include head/neck and GI tract
- Unique IHC profile: Polyphenotypic - expresses epithelial (EMA, cytokeratin), neural (NSE, synaptophysin), and mesenchymal (desmin - dot-like perinuclear) markers simultaneously. WT1 (C-terminal antibody, nuclear) is key
- Molecular: t(11;22)(p13;q12) fusing EWSR1 with WT1 - highly specific, detectable by RT-PCR or RNA-seq
- Recent work (2026, Brahmi et al., Curr Opin Oncol) highlights the role of androgen receptor (AR) expression in DSRCT - AR positivity in ~70% of cases, with implications for targeted therapy with AR antagonists. Multi-layered molecular profiling is informing novel treatment strategies in this ultra-rare tumour
- Prognosis: Poor; median survival ~2-4 years; hyperthermic intraperitoneal chemotherapy (HIPEC) under investigation
3.2 Neuroblastoma
- Age: Predominantly <5 years; arises from adrenal gland or sympathetic ganglia
- Morphology: Neuropil background (Homer-Wright rosettes); ranges from undifferentiated to differentiating
- IHC: Synaptophysin+, chromogranin+, NSE+, CD56+; PHOX2B (nuclear) is highly sensitive/specific
- Biochemical marker: Elevated urinary catecholamine metabolites (VMA, HVA) and MIBG avidity - unlike other SRCTs
- Molecular: MYCN amplification (poor prognosis), ALK mutations (targetable), segmental chromosomal aberrations
- Differential clue: The presence of neuropil is "highly distinctive" and essentially excludes other SRCTs; positive MIBG scan rules out all non-adrenergic SRCTs (Tietz Textbook)
3.3 Rhabdomyosarcoma (RMS)
- Subtypes: Embryonal (most common, children), Alveolar (PAX3/7-FOXO1 fusions, worse prognosis), Pleomorphic (adults), Spindle cell/Sclerosing (MYOD1 mutations)
- IHC: Desmin+, myogenin+ (nuclear, most specific), MyoD1+ (nuclear), MSA+; these myogenic markers are the diagnostic cornerstone
- Molecular: Alveolar RMS - t(2;13)(q35;q14) PAX3-FOXO1 or t(1;13)(p36;q14) PAX7-FOXO1; detection by FISH or RT-PCR is prognostically important (PAX3-FOXO1 = worse)
- Emerging markers: MYOD1 L122R mutation (spindle cell/sclerosing RMS) detectable by sequencing; relevant for targeted PI3K pathway inhibition
3.4 Wilms Tumour (Nephroblastoma)
- Classically presents in children <5 years as a renal mass; characterised by the classic triphasic pattern (blastema + epithelial + stromal)
- The blastemal component is the SRCT component
- IHC: WT1 (nuclear), cyclin D1, CD56; blastemal component is CD99+
- Molecular: WT1 mutations, WTX mutations, CTNNB1 mutations; anaplastic Wilms - TP53 mutations. Newer: SIX1/SIX2 mutations in blastemal-predominant Wilms
3.5 Lymphoma/Leukaemia
- Burkitt lymphoma: Extremely rapid proliferation; "starry sky" pattern; MYC rearrangement (8q24)
- Precursor B/T-ALL: Terminal deoxynucleotidyl transferase (TdT)+, CD34+, lineage-specific markers
- IHC differentiator: LCA (CD45) positivity effectively separates lymphoma from other SRCTs; TdT distinguishes precursor lesions
- Clinical clue: High WBC count, lymph node enlargement, bone marrow infiltration pattern (Tietz Textbook)
3.6 NUT Carcinoma (Midline Carcinoma)
- An aggressive carcinoma of midline structures (mediastinum, sinonasal, head/neck) with SRCT morphology; occasional "abrupt squamous differentiation"
- IHC: NUT IHC (nuclear, speckled pattern) - highly sensitive and specific; a single positive IHC is now considered diagnostic
- Molecular: BRD4-NUT t(15;19), BRD3-NUT, or NSD3-NUT fusions
- Bell et al. (Head Neck Pathol 2024, PMID 38315310) reviewed sinonasal SRCTs emphasising NUT IHC as a key "hack" in the IHC panel for poorly differentiated sinonasal SRCTs
3.7 Merkel Cell Carcinoma and Small Cell Carcinoma
- Merkel cell carcinoma: Neuroendocrine SRCT of skin; CK20+ (dot-like perinuclear), synaptophysin+, chromogranin+; associated with Merkel cell polyomavirus (MCPyV) - LT antigen IHC (CM2B4 antibody) positive in ~80%
- Small cell lung carcinoma: TTF-1+, CK7+, neuroendocrine markers+; rarely metastasises with SRCT morphology to sites that mimic primary SRCTs
4. Emerging and Recently Defined Entities
4.1 EWSR1::ATF1 and FET::CREB Fusion Tumours
4.2 SMARCA4-Deficient Undifferentiated Tumour
- Highly aggressive SRCT occurring in adults (especially thoracic)
- Loss of SMARCA4 (BRG1) protein by IHC - now a standard panel member in mediastinal/thoracic SRCTs
- WHO 2022 thoracic tumour classification recognises this as a distinct entity
4.3 Infantile Fibrosarcoma / Congenital Fibrosarcoma
- SRCT variant in neonates/infants; ETV6-NTRK3 fusion (targetable with TRK inhibitors - larotrectinib, entrectinib)
- NTRK IHC pan-Trk (EPR17341) serves as a screening tool before confirming by FISH/NGS
5. Diagnostic Approach: Tiered Algorithm
Step 1: Morphology + clinical context (age, site, serum markers)
↓
Step 2: First-line IHC panel
• CD99, TdT, LCA, desmin/myogenin, synaptophysin/chromogranin, WT1,
NKX2.2, S100, pan-keratin, NUT IHC, SMARCA4
↓
Step 3: Targeted molecular testing based on IHC
• EWSR1 FISH (break-apart) → if positive, partner identification needed
• BCOR IHC + CCNB3 IHC (for BCOR-CCNB3)
• CIC FISH (break-apart) + ETV4 IHC
↓
Step 4: RNA-based NGS fusion panel (if Steps 1-3 inconclusive)
→ Detects all known fusion transcripts in a single assay
→ Identifies rare/novel fusions (EWSR1::NFATc2, EWSR1::PATZ1, etc.)
↓
Step 5: Methylation array profiling (in research/reference centres)
→ Can resolve diagnostically challenging cases
→ WHO 5th edition recognises "essential" vs. "desirable" diagnostic criteria
to allow diagnosis in centres without full molecular capabilities
6. Role of Next-Generation Sequencing (NGS)
- Detects known and novel gene fusions simultaneously in one assay
- Required for definitive classification of EWSR1/FUS::NFATc2 and EWSR1::PATZ1 sarcomas
- Cytology specimens (FNA smears, cell blocks) yield high-quality nucleic acid and are now validated for NGS in round cell sarcomas (Gajdzis & Klijanienko, Acta Cytol 2026, PMID 41615867)
- DNA methylation profiling complements fusion detection for borderline/unclassifiable cases
- The 2025 reviews emphasise that accurate subclassification of EWSR1/FUS fusion variants carries direct therapeutic implications - different chemotherapy sensitivity and prognosis (Jennings et al., 2025)
7. Summary IHC Differential Table
| Tumour | CD99 | NKX2.2 | Desmin | Myogenin | Synaptophysin | WT1 | LCA | Key Molecular |
|---|---|---|---|---|---|---|---|---|
| Ewing sarcoma | +++ (membranous) | + | - | - | - | - | - | EWSR1-ETS fusions |
| CIC-rearranged | +/- (focal) | - | - | - | - | + (nuclear) | - | CIC-DUX4 |
| BCOR-CCNB3 | +/- | - | - | - | - | - | - | BCOR-CCNB3, CCNB3+ |
| DSRCT | + | - | + (dot) | - | + | + | - | EWSR1-WT1 |
| Rhabdomyosarcoma | - | - | + | ++ | - | - | - | PAX3/7-FOXO1 (alveolar) |
| Neuroblastoma | - | - | - | - | +++ | - | - | MYCN amp, ALK |
| Lymphoma/ALL | +/- | - | - | - | - | - | +++ | Lineage fusions |
| NUT carcinoma | - | - | - | - | - | - | - | BRD4/3/NSD3-NUT |
| SMARCA4-def. | - | - | - | - | - | - | - | SMARCA4 loss (IHC) |
| Merkel cell ca. | - | - | - | - | + | - | - | CK20 dot, MCPyV |
Key Recent References
- Dehner CA et al. "Updates on WHO classification for small round cell tumors: Ewing sarcoma vs. everything else." Hum Pathol 2024 - PMID 38280658
- Mori K et al. "Undifferentiated Small Round Cell Sarcomas: Radiologic-Pathologic Correlation for the Updated WHO 5th Ed." RadioGraphics 2026 - PMID 41886300
- Davis JL & Cheesman E. "Emerging round cell sarcomas in children." Virchows Arch 2025 - PMID 39576278
- Jennings LJ et al. "EWSR1/FUS::NFATC2 Sarcomas: Clinicopathologic review." Arch Pathol Lab Med 2025 - PMID 41167264
- Marcelis L & Sciot R. "Undifferentiated small round cell sarcomas of bone and soft tissue." Ann Pathol 2025 - PMID 39510958
- Makise N & Yoshida A. "Undifferentiated Small Round Cell Sarcomas of Bone." Surg Pathol Clin 2025 - PMID 40716917
- Gajdzis P & Klijanienko J. "Cytological, Immunocytochemical, and Molecular Findings of Extraskeletal Round Cell Sarcomas in Paediatric Patients." Acta Cytol 2026 - PMID 41615867
- Bell D. "Top IHC/ISH Hacks for Sinonasal Small Round Cell Tumors." Head Neck Pathol 2024 - PMID 38315310
- Robbins & Kumar Basic Pathology, p. 786 (Ewing sarcoma morphology)
- Quick Compendium of Clinical Pathology 5th Ed., p. 411 (EWSR1 family)
- Tietz Textbook of Laboratory Medicine 7th Ed. (neuroblastoma differential)