Fistula
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"fistula in ano" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from multiple surgical textbooks. Here is the complete overview:
Anal Fistula (Fistula-in-Ano) - Complete Overview
Definition
A fistula is an abnormal communication between two epithelium-lined surfaces. A fistula-in-ano is a chronic abnormal tract connecting the internal opening in the anal canal (at the dentate line) to one or more external openings on the perianal skin. The tract is usually lined by granulation tissue, but may become epithelialised in chronic cases. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Aetiology & Pathogenesis (Cryptoglandular Theory)
The dominant theory is cryptoglandular infection. Infected anal glands in the intersphincteric space form an abscess that then discharges through the sphincter complex to the perianal skin, completing the fistulous tract from internal opening to external skin. Approximately 50% of patients with a perianal abscess will ultimately develop a fistula. - Sabiston Textbook of Surgery
Other causes include:
- Crohn's disease (13-54% of Crohn patients develop anal fistulas)
- Tuberculosis
- Carcinoma
- Trauma / previous anorectal surgery
- Actinomycosis
Differential diagnoses for perianal fistulas include:
- Hidradenitis suppurativa - inflammation of apocrine glands; tracts are superficial and do not extend into the anal canal
- Pilonidal disease - foreign body reaction to hair in the gluteal cleft
- Mulholland and Greenfield's Surgery, 7th Ed.
Parks Classification
The most widely used classification, based on the relationship of the primary tract to the external sphincter:
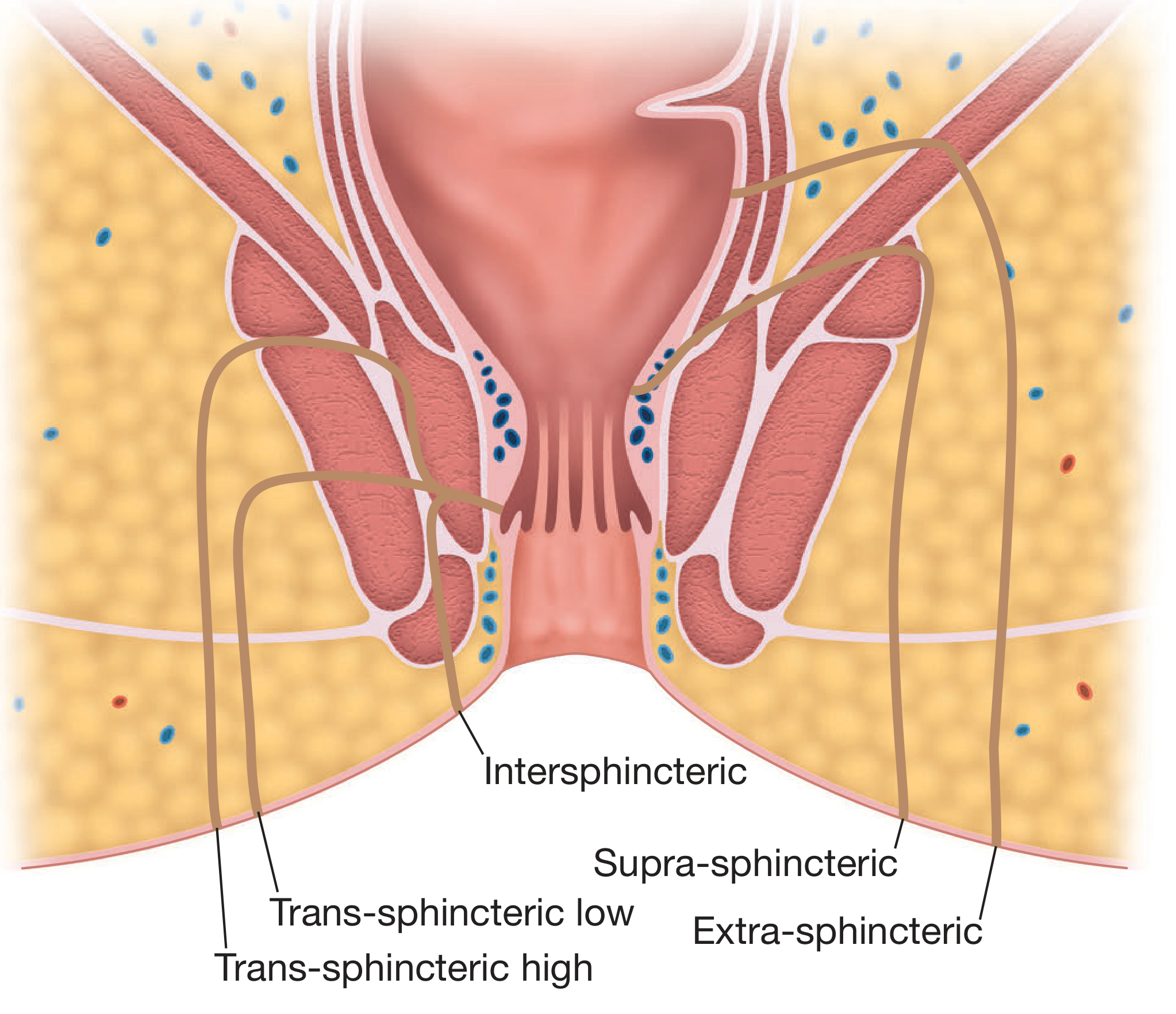
| Type | Frequency | Description |
|---|---|---|
| Intersphincteric | ~45% | Does NOT cross the external sphincter; runs through the intersphincteric plane to the perianal skin |
| Trans-sphincteric | ~40% | Crosses both internal and external sphincters at a variable level, then passes through the ischiorectal fossa to skin |
| Suprasphincteric | ~10% | Runs up above the puborectalis, then curls downward through the levators and ischioanal fossa to skin; often caused by excessive probing |
| Extrasphincteric | ~5% | Runs without relation to the sphincters; usually results from pelvic disease or trauma |
AGA (Simpler) Classification
The American Gastroenterological Association condenses Parks' into a clinically useful two-tier system:
| Simple fistula | Low tract (superficial or low inter-/trans-sphincteric); single external opening |
| Complex fistula | High tract; extra- or suprasphincteric; presence of abscess; anovaginal fistula; anal stricture |
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Clinical Features
- Perianal discharge - intermittent purulent (may be bloody) with temporary relief when pus drains
- Perianal pain - cyclical: builds up then releases with discharge
- Recurrent perianal abscess - the most common presentation
- Visible or palpable external opening - often with granulation tissue
- Passage of flatus or faeces through the external opening suggests a rectal (rather than anal) internal opening
- "Watering-can perineum" (multiple external openings) - raises strong suspicion for Crohn's disease
- Bailey and Love's; Mulholland and Greenfield's Surgery
Goodsall's Rule
An important rule to predict the internal opening location from the position of the external opening:
- Anterior external opening (anterior to a transverse anal line): tracks radially and directly to the nearest anal crypt
- Posterior external opening: tracks in a curvilinear fashion to a posterior midline internal opening
- Exception: an anterior external opening >3 cm from the anal verge may be an anterior extension of a posterior horseshoe fistula
- Sabiston Textbook of Surgery; Mulholland and Greenfield's
Investigation
Clinical assessment:
- Full history including obstetric, GI, surgical history, and continence status
- Identify: (1) site of internal opening, (2) site of external openings, (3) course of primary track, (4) secondary extensions, (5) complicating conditions
- Palpable induration suggests track course; dilute hydrogen peroxide instilled via the external opening helps identify the internal opening
- Proctosigmoidoscopy and examination under anaesthesia (EUA)
Imaging:
| Modality | Role |
|---|---|
| MRI (gold standard) | STIR sequences identify pus/granulation tissue; shows secondary extensions missed at surgery; preoperative MRI reduces recurrence in complex disease |
| Endoanal ultrasound (EAUS) | Useful for simple vs complex; enhanced with hydrogen peroxide injection; shows sphincter integrity |
| Fistulography / CT | Useful if extrasphincteric fistula is suspected |
- Grainger & Allison's Diagnostic Radiology; Bailey and Love's
Management
Principle: Eradicate the fistula while preserving continence. The most important determinant of post-operative function is the amount of sphincter muscle left behind, not the amount divided. At minimum, 2 cm of external sphincter should be retained. - Bailey and Love's
Surgical Options
1. Fistulotomy (Laying Open)
- Division of all structures between external and internal openings; wound heals by secondary intention
- Indicated for: intersphincteric fistulas; trans-sphincteric fistulas involving <30% of the external sphincter (avoid anterior fistulas in women)
- Healing rate: up to 90%
- Mulholland and Greenfield's Surgery
Recent evidence: A 2025 systematic review and meta-analysis (PMID 40125894) compared fistulotomy vs. fistulectomy for simple fistula-in-ano, confirming equivalent outcomes for simple tracts.
2. Fistulectomy
- Coring out the fistula tract (usually by diathermy)
- Better defines fistula anatomy and level of sphincter crossing; longer healing time than fistulotomy
3. Seton Placement
Loose seton:
- Non-absorbable thread tied without tension around the encircled muscle
- Used for: staged fistulotomy (allowing sepsis resolution before definitive surgery), long-term palliation in Crohn's disease, or in patients who refuse to risk incontinence
Cutting (tight) seton:
- Gradually tightened at 2-4 week intervals; gradually erodes through ("cheese-wires") the sphincter
- Allows slow fibrosis so divided muscle does not spring apart
- Success rates up to 94%, but incontinence risk 23-22%
- A 2023 meta-analysis (PMID 38091125) confirmed high healing rates but noted meaningful risk to continence
Ksharasutra (Ayurvedic method): A chemically active seton that burns through tissue; shown equivalent to one-stage fistulotomy for intersphincteric and distal trans-sphincteric fistulas
4. LIFT Procedure (Ligation of Intersphincteric Fistula Tract)
- Incision over the intersphincteric groove; fistula tract is ligated and divided; infected glands removed
- Sphincter-preserving: no sphincter muscle is divided
- Requires a mature, single straight trans-sphincteric tract (often after prior loose seton)
- Systematic reviews report healing rates of ~75% with no or minimal incontinence
- Bailey and Love's; Mulholland and Greenfield's
5. Endoanal Advancement Flap
- A broad-based, well-vascularised flap of anorectal mucosa and internal sphincter is raised; internal opening closed; flap advanced over it
- Used for complex fistulas where sphincter division is unsafe
- Success rate: 66-87%
- A repeat flap can be performed after a recovery interval if the first fails
6. Fibrin Glue & Fistula Plug
- Associated with high recurrence rates; NOT recommended as primary treatment
- Mulholland and Greenfield's Surgery
7. Biological Agents (emerging)
- Mesenchymal stem cells, cross-linked porcine dermal collagen
- Antibiotics (metronidazole, ciprofloxacin) for associated sepsis; also have immunomodulatory value in Crohn's disease
Crohn's-Related Anal Fistulas
- Affect 13-54% of Crohn's patients
- Asymptomatic fistulas do not need treatment
- Often complex: multiple external openings, branching tracts
- First step: unroof branching tracts to create a single track at the internal opening
- Anti-TNF agents (e.g. infliximab) are first-line medical management
- Long-term loose seton with medical therapy provides symptomatic control
- Temporary diversion may facilitate healing; proctectomy may be needed for severe perianal disease
- Mulholland and Greenfield's Surgery, 7th Ed.
Track Preparation Concept
An increasingly accepted concept before definitive surgery. Loose seton drainage followed by thorough debridement removes epithelialisation of the track and drains secondary extensions, creating better conditions for procedures like LIFT, advancement flap, or FiLaC (Fistula Tract Laser Closure). - Bailey and Love's
Summary Table: Surgery Selection by Fistula Type
| Fistula Type | Preferred Options |
|---|---|
| Intersphincteric (simple) | Fistulotomy |
| Trans-sphincteric, low | Fistulotomy |
| Trans-sphincteric, high | Seton (loose then cutting) or LIFT or Advancement flap |
| Suprasphincteric / Extrasphincteric | Seton palliation, Advancement flap |
| Anterior in women | Avoid fistulotomy; prefer LIFT or Advancement flap |
| Crohn's-associated | Loose seton + anti-TNF; LIFT or flap once inflammation controlled |
Sources: Bailey and Love's Short Practice of Surgery 28th Ed. | Sabiston Textbook of Surgery | Mulholland and Greenfield's Surgery 7th Ed. | Grainger & Allison's Diagnostic Radiology | Recent PubMed meta-analyses (PMIDs 40125894, 38091125, 37460830)
This is a shared conversation. Sign in to Orris to start your own chat.