Bronchial asthma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"asthma"[MeSH Terms] AND "management"[MeSH Terms]
Finding Sources
Searching PubMed
"asthma" AND "treatment"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have extensive material from multiple authoritative textbooks. Let me compile a comprehensive answer.
Bronchial Asthma
Definition
Bronchial asthma is a chronic inflammatory disorder of the airways characterized by three key elements:
- Reversible airway obstruction
- Airway inflammation (involving multiple cell types)
- Increased airway hyperresponsiveness to a variety of stimuli
It manifests clinically as recurrent episodes of wheezing, breathlessness, chest tightness, and cough - particularly at night or early morning. Unlike COPD, it is usually not a progressive disease, but if untreated, airway remodeling can occur. - Textbook of Family Medicine 9e, p. 463
Pathophysiology
Airflow obstruction in asthma results from three concurring processes:
- Bronchoconstriction - smooth muscle contraction
- Airway wall inflammation - mucosal edema from inflammatory cell infiltration
- Excessive mucus secretion - plugging the lumen
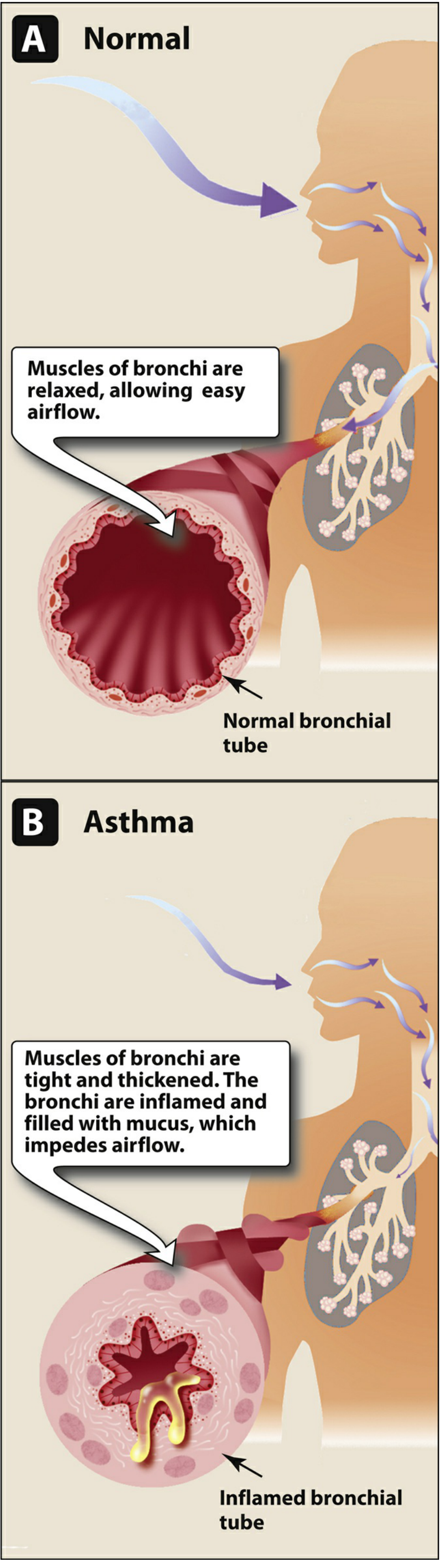
Fig. 1: Comparison of normal and asthmatic bronchi (Lippincott Illustrated Reviews: Pharmacology)
Inflammatory Cascade
- Allergens/triggers activate mast cells via IgE cross-linking -> release of histamine, leukotrienes, prostaglandins
- Eosinophils are recruited by IL-5 and contribute to epithelial damage
- T-lymphocytes (Th2 cells) drive the cytokine milieu (IL-4, IL-5, IL-13) sustaining eosinophilic inflammation
- Cysteinyl leukotrienes (LTC4, LTD4, LTE4) cause sustained bronchoconstriction, edema, and eosinophil migration
- Autopsies in fatal asthma show lungs with luminal plugs of inflammatory cells, desquamated epithelium, and mucus - ROSEN's Emergency Medicine, p. 928
Triggers / Precipitating Factors
| Category | Examples |
|---|---|
| Allergens | Dust mites, animal dander, pollen, mold, cockroach |
| Infections | Viral URIs (rhinovirus, RSV) |
| Exercise | Exercise-induced bronchoconstriction |
| Irritants | Smoke, air pollution, strong odors, cold air |
| Medications | Aspirin/NSAIDs, beta-blockers, ACE inhibitors |
| Stress / emotions | Psychogenic triggers |
| Occupational | Isocyanates, flour dust, latex |
| GERD | Micro-aspiration and vagal reflex |
Diagnosis
The diagnosis proceeds in three stages:
- Suggestive symptoms with precipitating factors
- Confirmatory testing (spirometry, bronchodilator reversibility, methacholine challenge)
- Symptomatic improvement with appropriate asthma therapy
Key spirometry finding: Post-bronchodilator FEV1 improvement ≥12% and ≥200 mL confirms reversible obstruction.
Differential Diagnosis:
| In Children | In Adults |
|---|---|
| Cystic fibrosis | COPD |
| Foreign body | Congestive heart failure |
| Viral bronchiolitis | Pulmonary embolism |
| GERD | GERD |
| Paradoxical vocal cord motion | ACE inhibitor cough |
- Textbook of Family Medicine 9e, p. 463
Classification of Severity (NHLBI / GINA)
| Severity | Symptoms | Nighttime Awakening | FEV1 % predicted |
|---|---|---|---|
| Intermittent | <2 days/week | ≤2x/month | >80% |
| Mild Persistent | >2 days/week but not daily | 3-4x/month | >80% |
| Moderate Persistent | Daily | >1x/week | 60-80% |
| Severe Persistent | Continual | Often 7x/week | <60% |
Classification is assigned based on the highest step at which any feature occurs, and should be reassessed over time. - Textbook of Family Medicine 9e, p. 464
Pharmacological Treatment (GINA 2024 Stepwise Approach)
GINA guidelines recommend all patients receive both a controller and a reliever medication.
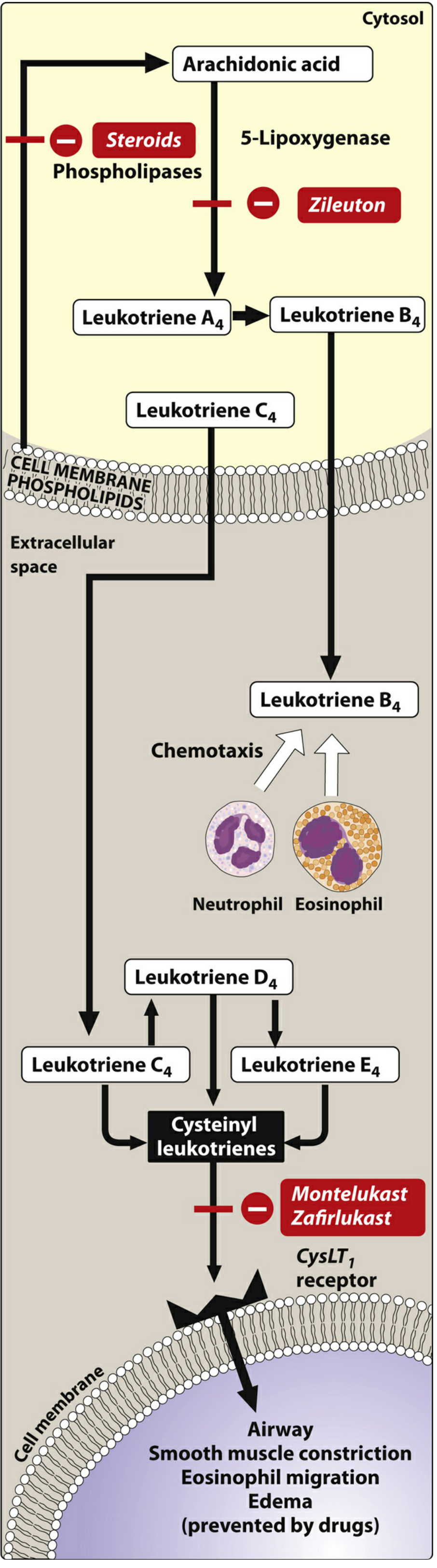
Fig. 2: Sites of action of asthma medications in the arachidonic acid/leukotriene pathway (Lippincott Illustrated Reviews: Pharmacology)
Step-Based Treatment (adults ≥12 years)
| Symptom Frequency | Preferred Controller | Preferred Reliever |
|---|---|---|
| <2x/month | Low-dose ICS-formoterol as needed | (as needed) |
| >2x/month but <daily | Low-dose ICS-formoterol as needed | (as needed) |
| Most days / ≥1x/week awakening | Low-dose maintenance ICS-formoterol | Low-dose ICS-formoterol PRN |
| Daily symptoms + low lung function | Medium-dose maintenance ICS-formoterol | Low-dose ICS-formoterol PRN |
Note: ICS/formoterol is the preferred reliever; SABAs are an alternative. - Lippincott Illustrated Reviews: Pharmacology, p. 1390
Drug Classes
1. Inhaled Corticosteroids (ICS) - Foundation of Controller Therapy
- Mechanism: Inhibit phospholipase A2 -> reduce arachidonic acid release -> decrease leukotriene synthesis; decrease eosinophils, macrophages, T-lymphocytes; reverse mucosal edema; reduce airway hyperresponsiveness
- Examples: Budesonide, fluticasone, beclomethasone, mometasone
- Adverse effects: Oropharyngeal candidiasis, hoarseness; rinse mouth after use
- Oral/IV corticosteroids (methylprednisolone, prednisone) reserved for severe exacerbations - no taper needed for short courses
2. Short-Acting β2 Agonists (SABA)
- Mechanism: Direct relaxation of airway smooth muscle; rapid onset 5-15 min; duration 3-6 h
- Examples: Albuterol (salbutamol), levalbuterol
- Role: Rescue/reliever therapy; prevention of exercise-induced bronchospasm
- Adverse effects: Tachycardia, tremor, hypokalemia, hypomagnesemia, hyperglycemia
- SABA monotherapy for persistent asthma is not recommended
3. Long-Acting β2 Agonists (LABA)
- Examples: Salmeterol (onset slow), formoterol (rapid onset)
- Duration ≥12 hours; formoterol can serve as both controller and reliever
- LABA monotherapy is contraindicated in asthma - must always be combined with ICS
- LABA monotherapy carries risk of severe/fatal exacerbations
4. Leukotriene Receptor Antagonists (LTRA)
- Examples: Montelukast, zafirlukast - block CysLT1 receptors
- Zileuton - inhibits 5-lipoxygenase (upstream in pathway)
- Role: Add-on controller therapy; particularly useful in aspirin-sensitive asthma and allergic rhinitis coexistence
5. Anticholinergics
- Ipratropium (short-acting): Blocks vagally mediated bronchoconstriction; slower onset than SABA; useful as add-on in acute exacerbations in ED; not routine monotherapy
- Tiotropium (long-acting): Add-on therapy for severe asthma with history of exacerbations
6. Theophylline
- Methylxanthine bronchodilator; narrow therapeutic index; largely replaced by β2 agonists and ICS
- Risk of seizures and fatal arrhythmias with overdose; requires serum level monitoring
- CYP1A2 substrate - many drug interactions
7. Monoclonal Antibodies (Biologics) - for Severe Persistent Asthma
| Drug | Target | Indication |
|---|---|---|
| Omalizumab | Anti-IgE | Allergic asthma, poorly controlled |
| Mepolizumab / Reslizumab / Benralizumab | IL-5 / IL-5Rα | Eosinophilic asthma |
| Dupilumab | IL-4Rα (blocks IL-4 + IL-13) | Severe eosinophilic / type 2 asthma |
All are add-on therapy for severe persistent asthma inadequately controlled on conventional therapy. Limited by high cost and parenteral administration. - Lippincott Illustrated Reviews: Pharmacology, p. 1398
Acute Exacerbations / Status Asthmaticus
Features of Severe Exacerbation
- PEFR or FEV1 <40% predicted
- PaCO2 rising (initially hypocapnia, then normocapnia/hypercapnia = sign of fatigue)
- Accessory muscle use, inability to speak in full sentences, cyanosis
- Pulsus paradoxus >10 mmHg
ED Management (stepwise)
- Initial assessment: Severity classification by PEFR, SpO2, respiratory effort
- Mild: SABA q20 min x 3 in first hour (albuterol 0.15 mg/kg nebulized, max 5 mg)
- Moderate-Severe:
- Inhaled SABA (continuous or frequent) + ipratropium bromide
- Systemic corticosteroids early (oral prednisolone or IV methylprednisolone)
- Supplemental O2 to maintain SpO2 ≥92-94%
- Refractory / Near-fatal:
- IV magnesium sulfate (2g IV over 20 min - evidence-based benefit in severe ED asthma)
- Heliox (helium-oxygen mixture) to reduce airway resistance
- Consider IV epinephrine or terbutaline
- Non-invasive or invasive ventilation (last resort; ventilating asthma carries high risk due to dynamic hyperinflation)
A key factor in asthma mortality is delayed corticosteroid initiation in the ED. - ROSEN's Emergency Medicine, p. 928
Asthma in Special Populations
Pregnancy
- ~4% of pregnant women have asthma; 1/3 will have exacerbations during pregnancy
- Moderate-severe asthma increases risk: preterm labor, LBW, perinatal death, preeclampsia
- FEV1 and PEFR are unchanged in normal pregnancy (unlike tidal volume, which increases)
- Key: undertreated asthma poses more risk to mother and fetus than asthma medications
- ICS are safe in pregnancy - Textbook of Family Medicine 9e, p. 489
Non-pharmacological / Adjunct Management
- Identify and avoid triggers (allergens, occupational agents, NSAIDs if aspirin-sensitive)
- Written asthma action plan for patients
- Control comorbid allergic rhinitis (upper-lower airway connection)
- Allergen immunotherapy for select patients with clear allergen sensitization
- Patient and family education on inhaler technique, spacer use, trigger avoidance
- Bronchial thermoplasty - bronchoscopic procedure for severe refractory asthma; reduces smooth muscle mass in airways (Murray & Nadel's Textbook of Respiratory Medicine)
Monitoring / Impairment Rating
The American Thoracic Society (ATS) impairment rating for asthma uses three domains scored together (Murray & Nadel's, p. 836):
- A. Post-bronchodilator FEV1 (0-4 points)
- B. Reversibility or degree of airway hyperresponsiveness (PC20) (0-3 points)
- C. Minimum medication requirement (0-4 points)
- Total score maps to Impairment Classes 0-V
Recent Evidence Update (2025)
A 2025 JAMA network meta-analysis (PMID 39465893) on inhaled reliever therapies for asthma supports ICS-formoterol as the preferred reliever over SABA alone, consistent with current GINA 2023/2024 guidance - as-needed ICS/formoterol reduces severe exacerbations without increasing overall ICS burden.
Sources:
- Lippincott Illustrated Reviews: Pharmacology (ICS, beta-agonists, biologics, drug mechanisms)
- Textbook of Family Medicine 9e (definition, diagnosis, classification, management steps)
- ROSEN's Emergency Medicine (acute exacerbation management, anatomy, epidemiology)
- Murray & Nadel's Textbook of Respiratory Medicine (impairment rating, thermoplasty)
- Fishman's Pulmonary Diseases and Disorders (allergic bronchial asthma, ABPA)
This is a shared conversation. Sign in to Orris to start your own chat.