Composition of blood and their functions notes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed to write comprehensive notes. Here they are:
Composition of Blood and Their Functions
Blood is a specialized connective tissue that circulates through the cardiovascular system. In a healthy adult, total blood volume is approximately 5 liters. Blood consists of two major components: plasma (the liquid portion, ~55%) and formed elements (cells and cell fragments, ~45%).
Overview: Components of Blood
| Component | % of Blood Volume | Key Elements |
|---|---|---|
| Plasma | ~55% | Water, proteins, electrolytes, nutrients, hormones |
| Formed Elements | ~45% | RBCs, WBCs, Platelets |
The percentage of blood occupied by red blood cells is called the hematocrit (normal: ~42-47% in females, ~45-52% in males).
1. PLASMA
Plasma is the straw-colored liquid matrix of blood. It is approximately 90% water, with the remaining 10% consisting of dissolved substances.
Composition of Plasma
| Substance | Approximate Content | Functions |
|---|---|---|
| Water | ~90% | Solvent; transports dissolved substances; regulates temperature |
| Plasma Proteins | 6-8 g/dL | See below |
| Electrolytes | Na+, K+, Ca2+, Cl-, HCO3- | Osmotic balance, acid-base regulation, nerve/muscle function |
| Nutrients | Glucose, amino acids, lipids, vitamins | Energy source, tissue repair |
| Waste Products | Urea, creatinine, bilirubin | Transported to kidneys/liver for excretion |
| Hormones | Insulin, cortisol, thyroid hormones | Endocrine signaling |
| Dissolved Gases | O2, CO2, N2 | Respiratory exchange |
Plasma Proteins
Plasma proteins are produced mainly by the liver and constitute the major solutes in plasma.
| Protein | Normal Value | Functions |
|---|---|---|
| Albumin | ~4.5 g/dL (largest fraction) | Maintains colloid osmotic (oncotic) pressure; transports fatty acids, bilirubin, drugs, hormones |
| Globulins (alpha, beta) | ~2.5 g/dL | Transport lipids (lipoproteins), metals (transferrin), fat-soluble vitamins; complement proteins |
| Gamma-globulins (immunoglobulins) | Part of globulin fraction | Antibodies - immune defense |
| Fibrinogen | ~0.3 g/dL | Precursor to fibrin; essential for blood clotting |
| Clotting Factors | Trace | Factor V, VIII, IX, X, etc. - coagulation cascade |
Serum = plasma with fibrinogen and clotting factors removed (i.e., what remains after blood clots).
2. FORMED ELEMENTS
A. Erythrocytes (Red Blood Cells - RBCs)
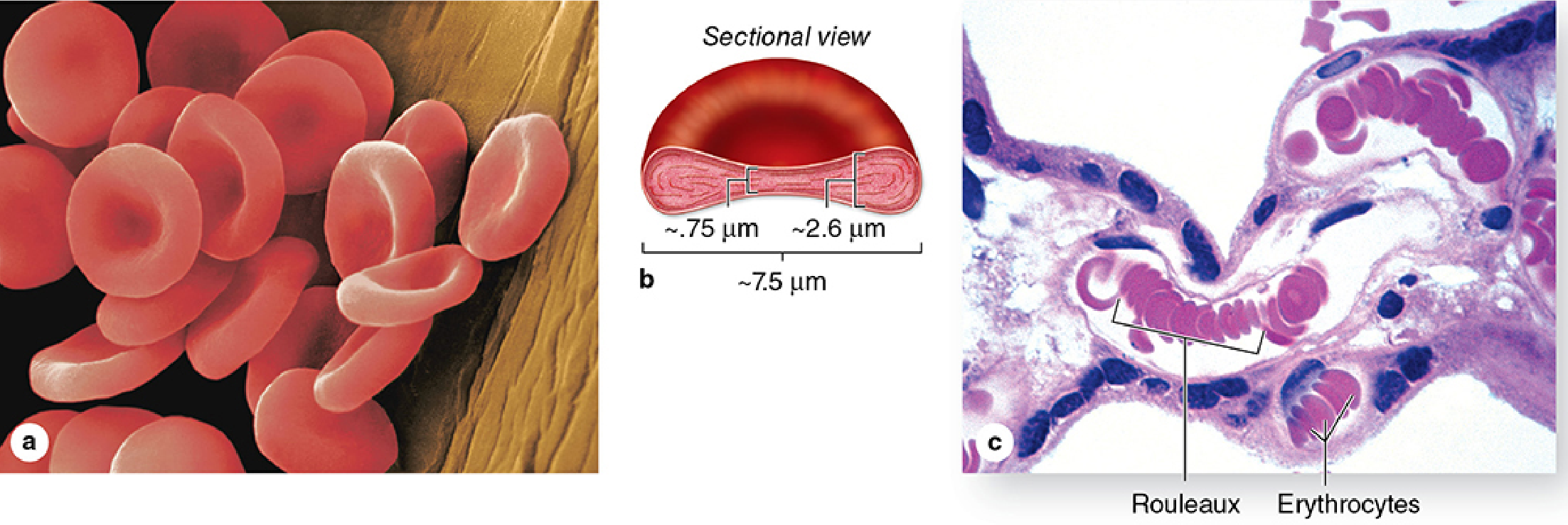
Morphology:
- Biconcave discs, ~7.5 μm in diameter, 2.6 μm thick at the rim, 0.75 μm thick in the center
- Anucleate (lack a nucleus) and lack organelles
- Cytoplasm completely filled with hemoglobin
- Membrane: ~40% lipid, 10% carbohydrate, 50% protein (includes Band 3 protein, glycophorin A - basis of ABO blood group)
- Submembranous cytoskeleton: spectrin + actin + ankyrin network maintains shape and flexibility
Normal Count:
- Women: 3.9-5.5 million/μL
- Men: 4.1-6.0 million/μL
Life Span: ~120 days; removed by macrophages in the spleen, liver, and bone marrow
Functions:
- Oxygen transport - Hemoglobin binds O2 (as oxyhemoglobin) and delivers it to tissues
- Carbon dioxide transport - Hemoglobin binds CO2 (as carbaminohemoglobin) and returns it to the lungs
- Acid-base buffering - Hemoglobin acts as a buffer by binding/releasing H+ ions
- Internal size standard - Uniform dimensions allow estimation of other cell sizes in histology
Energy: Rely on anaerobic glycolysis (no mitochondria)
Clinical Note: Anemia = RBC count below normal range. Polycythemia = increased RBC count (e.g., high-altitude adaptation).
B. Leukocytes (White Blood Cells - WBCs)
Normal count: ~7,000 WBCs/μL (vs. 5 million RBCs/μL)
Leukocytes are the mobile units of the body's immune and defense system. Unlike RBCs, they leave the vasculature to function in tissues - entering via diapedesis (extravasation) through capillary walls.
Genesis:
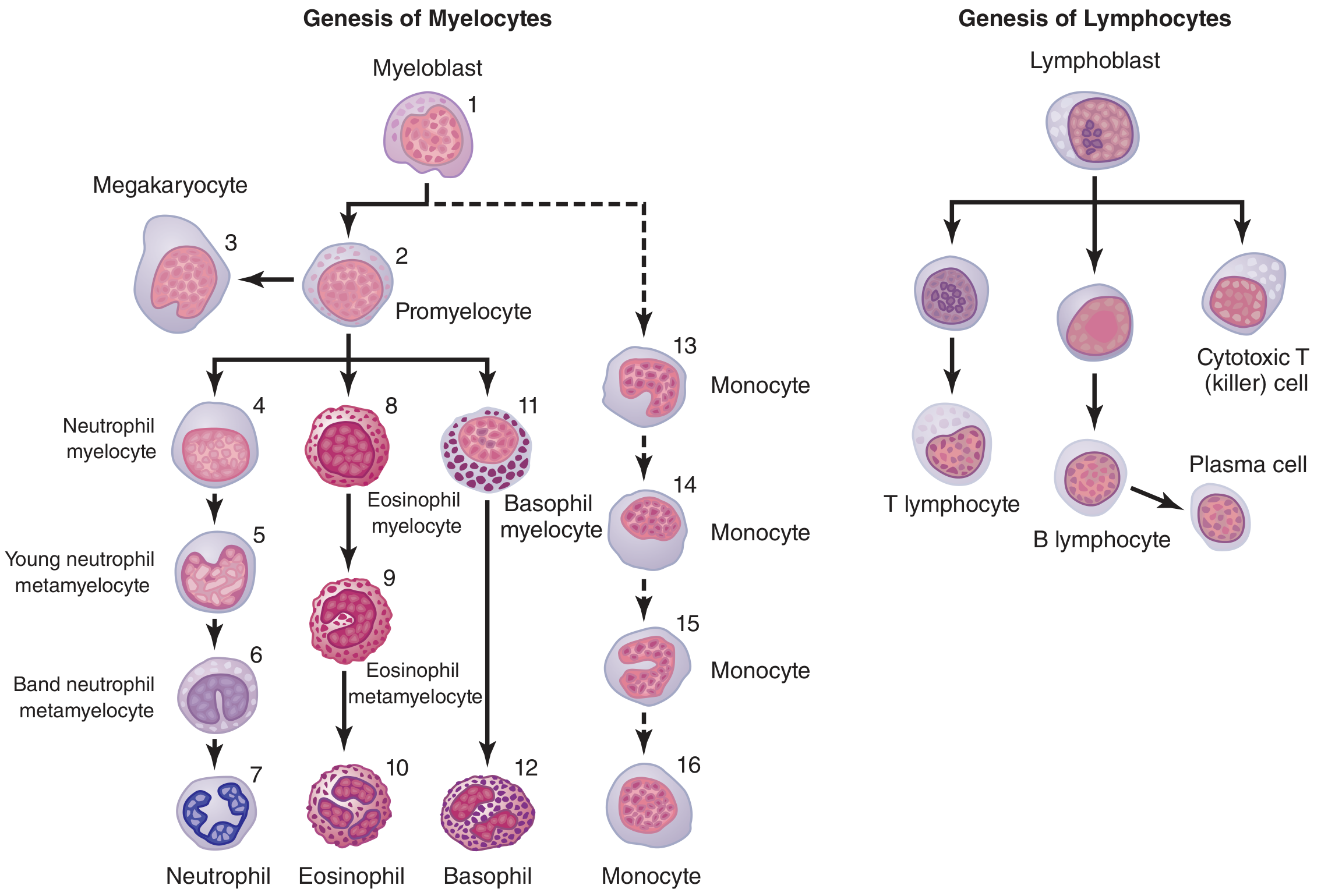 Genesis of white blood cells showing the myelocytic lineage (neutrophils, eosinophils, basophils, monocytes) and lymphocytic lineage (T cells, B cells, plasma cells). - Guyton & Hall Textbook of Medical Physiology
Genesis of white blood cells showing the myelocytic lineage (neutrophils, eosinophils, basophils, monocytes) and lymphocytic lineage (T cells, B cells, plasma cells). - Guyton & Hall Textbook of Medical Physiology
WBCs are divided into Granulocytes and Agranulocytes:
GRANULOCYTES (have prominent cytoplasmic granules; multilobed nuclei)
1. Neutrophils
- Most abundant WBC: 62% of total WBCs
- Nucleus: multilobed (3-5 lobes, "polymorphonuclear")
- Granules: azurophilic (primary - contain MPO, defensins, lysozyme) + specific/secondary (collagenase, lactoferrin)
- Life span: 4-8 hours in blood, 1-4 days in tissues
- Functions:
- Primary defense against bacterial infections
- Phagocytosis: engulf and destroy bacteria in phagolysosomes
- Release superoxide radicals (O2-) and H2O2 (oxidative burst) for microbial killing
- Lactoferrin binds iron, starving bacteria
- Short-lived; dying neutrophils + bacteria + tissue fluid = pus
- Release proresolving mediators and chemokines to recruit other immune cells
2. Eosinophils
- 2.3% of total WBCs (1-4% range)
- Nucleus: bilobed
- Granules: large, acidophilic (pink/red); contain Major Basic Protein (MBP), eosinophilic peroxidase
- Life span: similar to neutrophils; concentrated in gut mucosa and lung tissue
- Functions:
- Defense against parasitic infections (helminths)
- Modulate allergic responses (asthma, hay fever) by releasing chemokines, cytokines, and proresolving lipid mediators
- Phagocytose antigen-antibody complexes
- Increased in helminthic infections and allergic diseases (eosinophilia)
3. Basophils
- Least common: 0.4% of total WBCs
- Nucleus: bilobed or irregular, obscured by granules
- Granules: large, intensely basophilic (purple-blue); contain histamine and heparin
- Functions:
- Release histamine - triggers vasodilation and increased vascular permeability in allergic reactions
- Release heparin - local anticoagulant, promotes blood flow at inflammatory sites
- Role in immediate hypersensitivity (Type I) reactions
- Analogous to tissue mast cells
AGRANULOCYTES (few or no visible granules; non-lobed nuclei)
4. Monocytes
- 5.3% of total WBCs; largest WBC (12-20 μm diameter)
- Nucleus: kidney-shaped, indented, or C-shaped; basophilic cytoplasm with fine azurophilic granules
- Transit in blood: only 10-20 hours, then migrate to tissues
- In tissues: differentiate into macrophages (swelling up to 60-80 μm, much more potent)
- Functions:
- Phagocytosis of bacteria, cellular debris, and foreign particles (as macrophages)
- Antigen presentation to lymphocytes
- Tissue macrophages: long-lived tissue defense (months)
- Monocyte recruitment is key in both acute and chronic inflammation
5. Lymphocytes
- 30% of total WBCs; second most abundant
- Small cells (6-12 μm); large, round, dark nucleus occupying most of the cell
- Produced in bone marrow; mature in thymus (T cells) or bone marrow/lymphoid tissue (B cells)
- Circulate continuously: blood → lymph → tissues → lymph → blood
- Life span: weeks to months depending on activation state
- Functions:
- T lymphocytes (T cells): Cell-mediated immunity - destroy virus-infected/tumor cells (cytotoxic T cells); regulate immune responses (helper T cells)
- B lymphocytes (B cells): Humoral immunity - differentiate into plasma cells that produce antibodies (immunoglobulins)
- Natural Killer (NK) cells: Innate immunity against tumor and virus-infected cells
6. Plasma Cells (derived from B cells)
- Found mainly in tissues, rarely in blood
- Produce large quantities of specific antibodies
- Identified by "clock-face" chromatin pattern in nucleus
C. Platelets (Thrombocytes)
Morphology:
- Tiny, non-nucleated cell fragments, only 2-4 μm in diameter
- Derived by budding from megakaryocytes in bone marrow
- Contain alpha-granules (fibrinogen, vWF, growth factors) and dense granules (ADP, serotonin, Ca2+)
- Open canalicular system (OCS) for rapid granule secretion
Normal Count: 150,000-400,000/μL (average ~300,000/μL)
Life Span: ~10 days; ~150 billion platelets produced daily
Functions:
- Primary hemostasis - rapidly adhere to damaged vessel wall (collagen exposure) via vWF, aggregate to form a "platelet plug"
- Activate coagulation cascade - release ADP, thromboxane A2, and other factors that trigger secondary hemostasis (fibrin clot formation)
- Repair microvascular tears - plug minor leaks in capillaries and venules
- Wound healing - release growth factors (PDGF, VEGF) promoting tissue repair
Clinical notes:
- Thrombocytopenia (< 150,000/μL) = increased bleeding risk
- Thrombocytosis (> 400,000/μL) = increased clotting risk
Summary Table: Formed Elements
| Cell | Normal Count | Life Span | Key Function |
|---|---|---|---|
| Erythrocytes (RBCs) | 4-6 million/μL | 120 days | O2/CO2 transport, acid-base buffering |
| Neutrophils | 62% of WBCs | 4-8 h (blood); 1-4 days (tissue) | Phagocytosis, bacterial defense |
| Eosinophils | 2.3% of WBCs | Similar to neutrophils | Anti-parasitic, allergic modulation |
| Basophils | 0.4% of WBCs | Similar to neutrophils | Allergic reactions (histamine, heparin) |
| Monocytes | 5.3% of WBCs | 10-20 h (blood); months (tissue as macrophages) | Phagocytosis, antigen presentation |
| Lymphocytes | 30% of WBCs | Weeks to months | Adaptive immunity (T & B cell responses) |
| Platelets | 150,000-400,000/μL | 10 days | Hemostasis, clot formation, vessel repair |
Key Terminology
- Hematocrit: % of blood volume occupied by RBCs (~45%)
- Hemoglobin: Iron-containing protein in RBCs; each molecule carries 4 O2 molecules
- Diapedesis: WBC migration through capillary walls into tissues
- Chemotaxis: Directed WBC movement toward chemical signals at sites of infection/inflammation
- Phagocytosis: Engulfment and destruction of pathogens/debris by neutrophils and macrophages
- Serum: Plasma minus clotting factors (what remains after a clot forms)
- Rouleau: Stacking of RBCs in low-flow conditions, like coins in a roll
Sources: Guyton & Hall Textbook of Medical Physiology; Junqueira's Basic Histology, 17e; Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.