Gastric ulcer
Reading File
Finding Sources
Searching PubMed
"peptic ulcer disease"[MeSH Terms] AND "gastric ulcer"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative surgical and medical textbooks. Let me compose the full response.
Gastric Ulcer
A gastric ulcer is a discrete macroscopic mucosal defect in the stomach wall, extending into the submucosa or muscularis propria, resulting from an imbalance between aggressive luminal forces (acid and pepsin) and the mucosal defense mechanisms. - Current Surgical Therapy 14e
Epidemiology
- In the US, approximately 90,000 new cases/year - about one-fifth the incidence of duodenal ulcers.
- In Japan, gastric ulcers are 5-10 times more common than duodenal ulcers.
- More common in men than women.
- Occurs ~10 years later in life than duodenal ulcers.
-
- Maingot's Abdominal Operations
Etiology & Pathophysiology
The primary causes are:
- Helicobacter pylori infection - the most common underlying factor; causes chronic mucosal inflammation that primes the lamina propria with inflammatory cells and mediators, impairing local defenses.
- NSAIDs / Aspirin - block prostaglandin production, impairing mucus secretion, mucosal blood flow, and epithelial restitution.
- Smoking - decreases mucosal blood flow and impairs medical therapy.
- Physiologic or psychological stress - impairs mucosal blood flow, gastric motility, and acid secretion.
- Cocaine use - can cause rapidly forming ulcers.
Mucosal defense relies on: mucus secretion by surface epithelial cells (SECs), rapid epithelial restitution, augmented mucosal blood flow, and prostaglandin signaling. Any of the above agents disrupts one or more of these layers. - Current Surgical Therapy 14e
Modified Johnson Classification (Types)
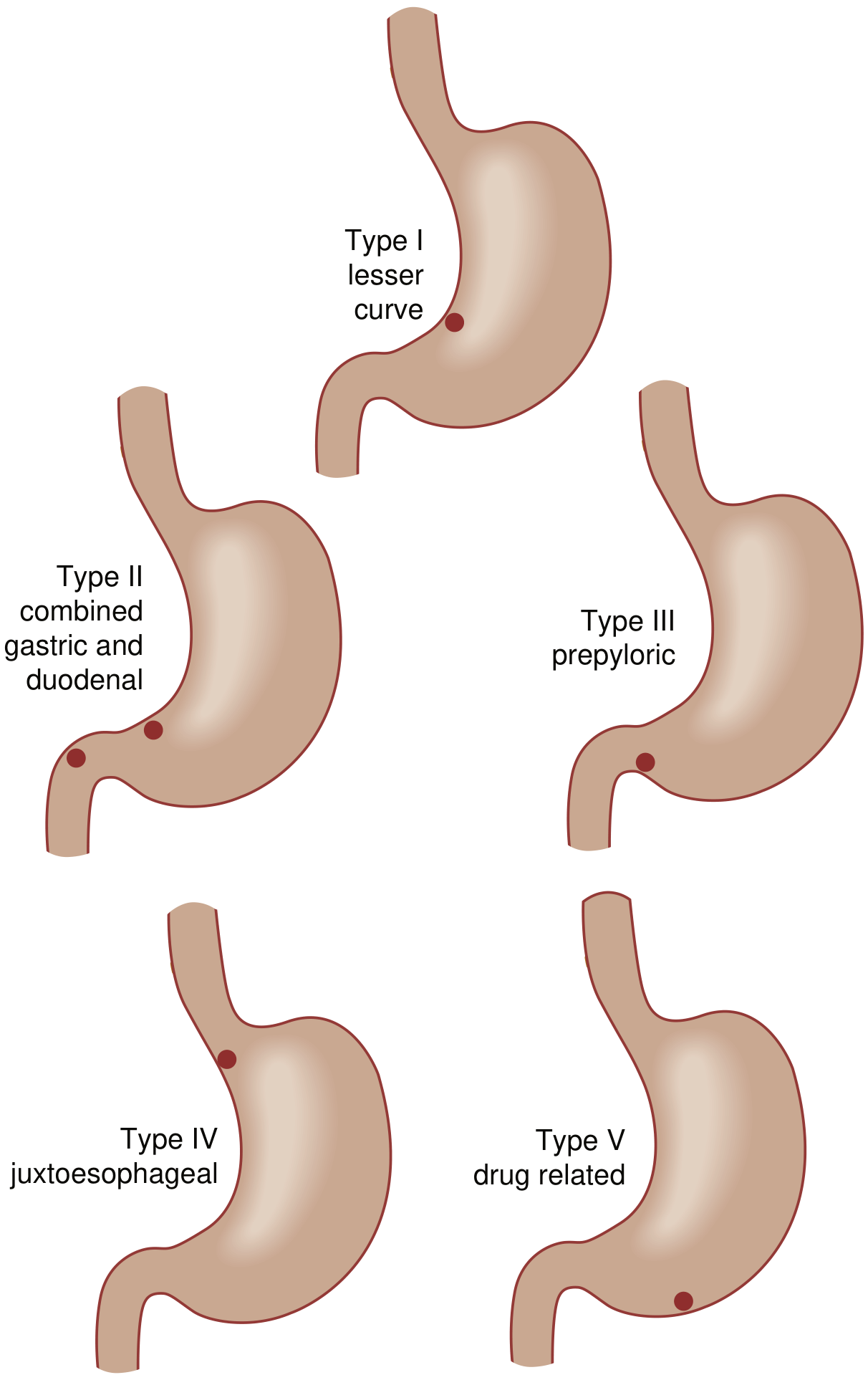
| Type | Location | Acid Hypersecretion | Notes |
|---|---|---|---|
| I | Lesser curvature, near incisura angularis | No | Most common type |
| II | Body/incisura + concurrent duodenal ulcer | Yes | Resembles duodenal ulcer pathophysiology |
| III | Prepyloric | Yes | Resembles duodenal ulcer pathophysiology |
| IV | High lesser curvature, near GE junction | No | Technically challenging to resect |
| V | Anywhere (medication-induced) | No | Typically greater curvature; drug-related |
- Current Surgical Therapy 14e
Key surgical implication: Types II and III resemble duodenal ulcers physiologically and therefore require truncal vagotomy as part of surgical treatment (in addition to resection). Types I, IV, and V do not.
Clinical Manifestations
- Recurrent epigastric pain (often worsened by food, unlike duodenal ulcer where food relieves pain)
- Nausea, vomiting
- Iron deficiency anemia
- Complications: bleeding, perforation, obstruction, rarely gastrocolic fistula
Key distinction from duodenal ulcer: Malignancy must always be excluded in gastric ulcers. Duodenal ulcers are virtually never malignant. All gastric ulcers require multiple biopsies from the perimeter of the lesion at endoscopy. - Sabiston Textbook of Surgery
Pain radiation to the back suggests posterior penetration into the pancreas. Diffuse peritoneal signs indicate free perforation.
Diagnosis
Upper GI Endoscopy (preferred)
- Benign appearance: smooth, flat ulcer with gray fibrous exudate; raised, erythematous margin.
- Visual appearance alone cannot distinguish benign from malignant - biopsy is mandatory.
- Multiple biopsies + endoscopic brushings increase accuracy to ~95%.
- Repeat endoscopy in 2-3 months to document healing and perform repeat biopsy.
- Risk of missing gastric adenocarcinoma/lymphoma with proper biopsy protocol: ~1%.
Upper GI Barium Radiology
- Demonstrates barium within the ulcer crater (round or ovoid).
- Used as an adjunct but less preferred than endoscopy.
Labs
- CBC, liver chemistries, creatinine, amylase, calcium.
- Serum gastrin level in refractory or recurrent ulcers (to exclude Zollinger-Ellison syndrome).
- Sabiston Textbook of Surgery
Location
-
50% are on the lesser curvature, proximal to the incisura angularis.
- <10% on the greater curvature.
- Most lie within 2 cm of the histologic transition between fundic and antral mucosa.
- Maingot's Abdominal Operations
Medical Management
First-line treatment:
- H. pylori eradication (antibiotic triple/quadruple therapy) - response rates equivalent to duodenal ulcer; recurrence after eradication equals the rate of reinfection.
- Cease NSAIDs/aspirin - mandatory for healing.
- Stop smoking.
- PPI therapy for 2-3 months.
If all three causative factors are eliminated, almost all gastric ulcers heal with a 2-3 month PPI course. If any persist, recurrence after stopping acid suppression is the rule. Patients requiring long-term NSAIDs post-operatively should receive long-term acid suppression; selective COX-2 inhibitors may carry lower ulcer risk. - Current Surgical Therapy 14e
Indications for Surgery
Surgery is reserved for complications:
- Perforation (most common indication for operative intervention)
- Hemorrhage (most frequent complication overall)
- Obstruction (especially type II and III, must exclude carcinoma)
- Nonhealing/intractability (raises concern for malignancy - unlike duodenal ulcer, this is itself an indication for operation)
Surgical Options
By Ulcer Type (Elective)
| Type | Option 1 (Resect Ulcer) | Option 2 (Biopsy + Leave) |
|---|---|---|
| I | Distal gastrectomy | Vagotomy + drainage (± wedge) |
| II | Distal gastrectomy + vagotomy | Vagotomy + drainage |
| III | Distal gastrectomy + vagotomy | Vagotomy + drainage |
| IV | Csendes (Roux) or Pauchet procedure | Kelling-Madlener or vagotomy + drainage |
| V | Wedge resection | Patch/oversew |
- Current Surgical Therapy 14e
Note: In unstable patients, simple patch/oversew with biopsy is appropriate for any type.
By Complication (Emergency)
| Indication | Option 1 | Option 2 | Option 3 |
|---|---|---|---|
| Perforation | Patch/wedge excision | Patch + vagotomy + drainage | Distal gastrectomy* |
| Bleeding | Oversew/wedge excision | Oversew + vagotomy + drainage | Distal gastrectomy* |
| Obstruction | Vagotomy + distal gastrectomy | Vagotomy + gastrojejunostomy | - |
| Nonhealing | Distal gastrectomy (+ vagotomy for II/III) | Wedge + vagotomy + drainage | - |
Add vagotomy for type II and III.
Reconstruction after distal gastrectomy:
- Billroth I (gastroduodenostomy)
- Billroth II (gastrojejunostomy) - preferred with concomitant duodenal ulcer
- Roux-en-Y - preferred with small gastric remnant or proximal anastomosis
Elective operative mortality: ~2-3%. Ulcer recurrence rate after surgery: <5%.
Complications in Detail
Perforation
- Anterior lesser curvature is the most common site.
- Presents with acute abdominal pain, peritoneal signs, free intraperitoneal air on CT.
- Management: IV fluids, IV antibiotics (cefazolin + fluconazole), NG tube decompression, surgery within ~2 hours.
- Laparoscopic or open approach. Copious peritoneal irrigation (5-10 L warm saline).
- In stable, sealed perforations without sepsis: non-operative management may be considered.
- Current Surgical Therapy 14e
Bleeding
- Most frequent complication overall.
- Endoscopic hemostasis is first-line.
- Rockall score is used to stratify rebleeding risk and mortality (incorporates age, shock, comorbidities, diagnosis, and endoscopic stigmata).
Gastric Outlet Obstruction
- More commonly from type II or III ulcers.
- Must distinguish benign obstruction from carcinoma.
Benign vs. Malignant Gastric Ulcer
| Feature | Benign | Malignant |
|---|---|---|
| Margins | Smooth, regular | Irregular, nodular |
| Base | Gray fibrous exudate | Necrotic, irregular |
| Surrounding folds | Radiate to ulcer edge | Interrupted, clubbed |
| Visual alone | Cannot reliably distinguish | |
| Biopsy | Mandatory for all |
All gastric ulcers require multiple biopsies. Visual appearance alone, even to an experienced endoscopist, cannot exclude malignancy.
Key Takeaways
- Gastric ulcer differs from duodenal ulcer in that malignancy must always be excluded.
- The modified Johnson classification (Types I-V) guides surgical approach.
- H. pylori eradication + PPI + cessation of NSAIDs/smoking heals most ulcers medically.
- Surgery is indicated for complications (perforation, bleeding, obstruction) and nonhealing (raises malignancy concern).
- Types II and III require vagotomy due to associated acid hypersecretion; Types I, IV, V do not.
Sources: Current Surgical Therapy 14e; Maingot's Abdominal Operations; Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.