65 year old paitent come with right sided weakness in arm and right sided toungue deviation what should be the next line of management
Reading File
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a full, authoritative answer.
Clinical Localization: Déjerine's Medial Medullary Syndrome (Déjerine Anterior Bulbar Syndrome)
Clarification first — the anatomical key:
| Finding | Side | Explanation |
|---|---|---|
| Right arm weakness | Right (contralateral to lesion) | Pyramid (corticospinal tract) involvement before decussation |
| Right tongue deviation | Right (ipsilateral to lesion) | LMN CN XII nucleus/fascicles in the right medulla |
The tongue deviates toward the lesion side in a LMN (nuclear/fascicular) lesion. Right tongue deviation + right arm weakness = RIGHT-sided medial medullary lesion (Déjerine syndrome).
This is a crossed (alternate) hemiplegia, the hallmark of brainstem pathology.
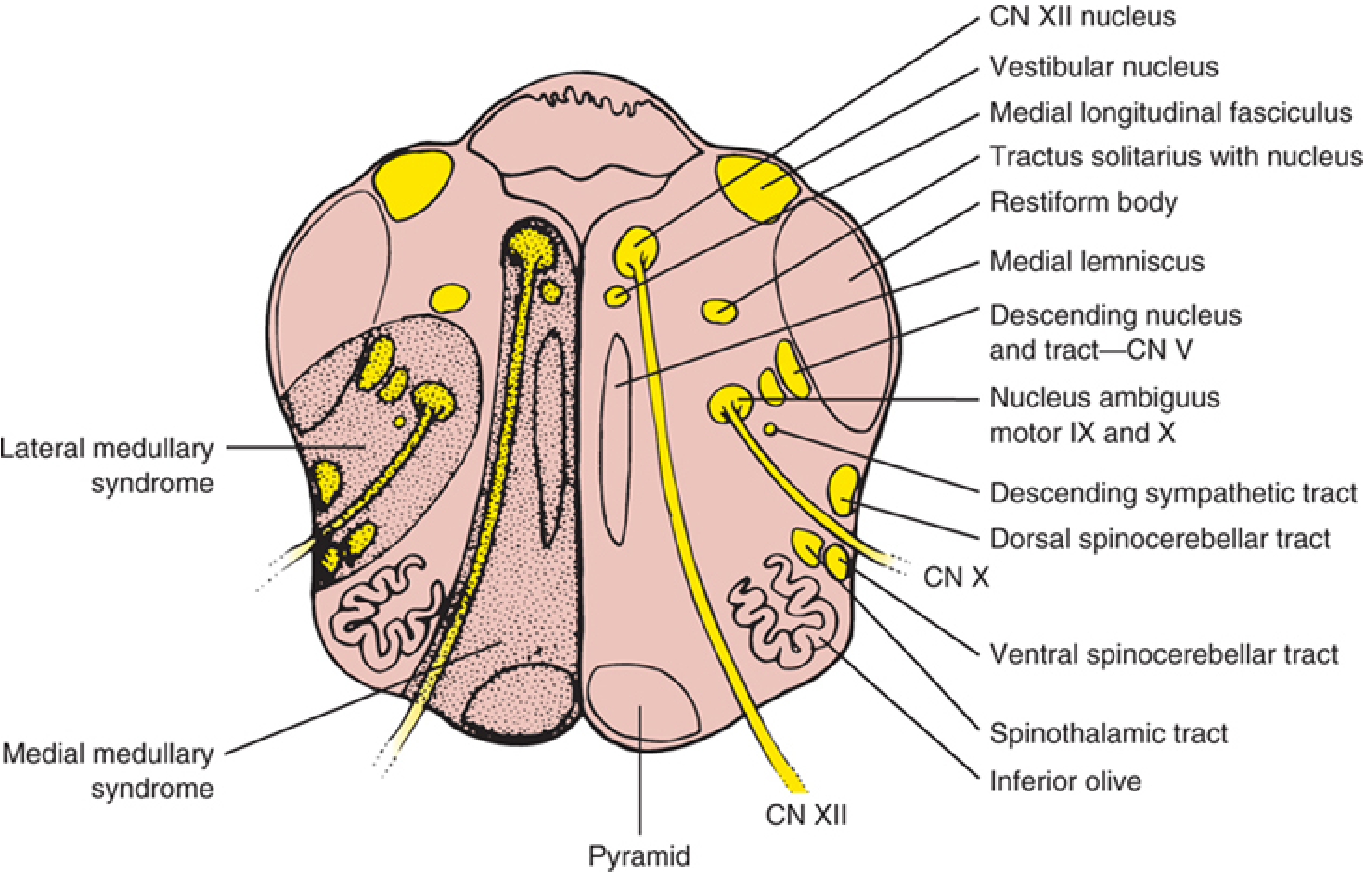
The medial medullary lesion zone involves: ipsilateral CN XII nucleus → tongue deviation ipsilaterally; the pyramid below its decussation → contralateral hemiplegia (arm > leg, face spared); and often the medial lemniscus → contralateral proprioception/vibration loss. — Localization in Clinical Neurology, 8e
Management — Next Steps (Acute Ischemic Stroke Protocol)
STEP 1 — Immediate Stabilization (within minutes)
| Action | Detail |
|---|---|
| Airway, Breathing, Circulation (ABCs) | Assess for airway compromise; pulse oximetry; supplemental O₂ if SpO₂ <94% |
| IV access + blood draw | CBC, PT/INR, aPTT, blood glucose (finger-stick immediately), BMP, LFTs, type & screen |
| Finger-stick glucose | Treat hypoglycemia (<60 mg/dL) immediately; avoid hyperglycemia |
| Cardiac monitoring | 12-lead ECG + continuous telemetry for at least 48 hours (AF, MI may co-occur in 3–20%) |
| NPO + aspiration precautions | Brainstem strokes have aspiration in >1/3 of cases; keep NPO until formal swallow assessment |
STEP 2 — Emergency Neuroimaging (within 25 minutes of arrival)
- Non-contrast CT head: Rule out hemorrhagic stroke — this is mandatory before any thrombolysis. CT is less sensitive for posterior fossa/brainstem infarcts.
- MRI brain with DWI (diffusion-weighted imaging): Far superior for brainstem lesions; will show restricted diffusion in the medial medulla. MRI + MRA (magnetic resonance angiography) to assess vertebral/basilar artery patency.
- CTA head + neck: If MRI not immediately available; evaluates vertebral artery occlusion (most common cause of medial medullary syndrome).
"Perform an emergency noncontrast head CT scan to differentiate between ischemic stroke and hemorrhagic stroke; there are no reliable clinical findings that conclusively separate ischemia from hemorrhage." — Harrison's Principles of Internal Medicine 22e
STEP 3 — Reperfusion Therapy (time-critical)
IV Thrombolysis — IV Alteplase (tPA)
- If within 4.5 hours of symptom onset and no contraindications → IV alteplase 0.9 mg/kg (max 90 mg); 10% as bolus, remainder over 60 min
- Pre-thrombolysis BP target: Must be <185/110 mmHg before administration (use IV labetalol or nicardipine)
- Key contraindications: Active hemorrhage, recent surgery, anticoagulant use with therapeutic INR, prior intracranial hemorrhage
Endovascular Thrombectomy (Mechanical)
- If large vessel occlusion (vertebral or basilar artery) is confirmed on CTA/MRA
- Can be considered up to 24 hours in selected patients with favorable imaging profile
- Basilar artery occlusion: thrombectomy has particular benefit given high mortality of untreated basilar occlusion
STEP 4 — Blood Pressure Management
| Scenario | BP Target |
|---|---|
| Not a thrombolysis candidate | Allow up to 220/120 mmHg (permissive hypertension to maintain perfusion) |
| Candidate for thrombolysis | Lower to <185/110 mmHg before tPA |
| After tPA | Maintain <180/105 mmHg for 24 hours post-infusion |
| Agent of choice for acute lowering | IV labetalol 10 mg over 1–2 min (repeat/double q10 min, max 300 mg) or IV nicardipine |
"Blood pressure should be reduced if it exceeds 220/120 mmHg... or if blood pressure is >185/110 mmHg and thrombolytic therapy is anticipated." — Harrison's 22e
STEP 5 — Antithrombotic Therapy (if tPA not given)
- Aspirin 325 mg within 24–48 hours of stroke onset
- For minor stroke/TIA: dual antiplatelet therapy (aspirin + clopidogrel) for 21 days reduces early recurrence
- Anticoagulation (heparin): Not routinely indicated for atherothrombotic stroke; may be considered for cardioembolic stroke (AF) after ruling out hemorrhagic transformation
STEP 6 — Etiology Workup (early, guides secondary prevention)
| Investigation | Purpose |
|---|---|
| MRI brain + MRA neck/head | Identify vertebral/basilar artery occlusion or stenosis |
| Echocardiography (TTE/TEE) | Cardioembolic source |
| Holter/prolonged cardiac monitoring | Paroxysmal AF |
| Lipid panel, HbA1c, fasting glucose | Vascular risk factors |
| Hypercoagulable workup | If cryptogenic stroke |
STEP 7 — Admit to Stroke Unit / ICU
- Specialized stroke unit admission: reduces mortality, length of stay, and nursing home discharge
- Avoid hyperthermia (treat fever aggressively — worsens ischemic outcome)
- Maintain euglycemia (avoid both hypo- and hyperglycemia)
- DVT prophylaxis: pneumatic compression stockings (safe even post-thrombolysis)
- Early physiotherapy, occupational therapy, and speech pathology assessment
Summary Flowchart
Acute presentation (right arm weakness + right tongue deviation)
↓
Localize → Right medial medullary stroke (Déjerine syndrome)
↓
IMMEDIATE: ABCs, IV access, glucose, cardiac monitoring, NPO
↓
URGENT: Non-contrast CT head (rule out hemorrhage)
↓
MRI DWI / CTA head & neck (confirm infarct + identify vessel)
↓
TIME WINDOW CHECK:
≤4.5 h + no contraindications → IV Alteplase (tPA)
Large vessel occlusion → Mechanical Thrombectomy (up to 24 h)
↓
BP management + Aspirin (if no tPA) + Stroke Unit admission
↓
Etiology workup → Secondary prevention
Sources:
- Harrison's Principles of Internal Medicine 22e (2025) — Chapter 438, Acute Ischemic Stroke
- Bradley and Daroff's Neurology in Clinical Practice — Chapter 65, General Management of Acute Ischemic Stroke
- Localization in Clinical Neurology, 8e — Chapter 15, Medial Medullary Syndrome (Déjerine Anterior Bulbar Syndrome)
This is a shared conversation. Sign in to Orris to start your own chat.