Abnormality of placenta
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I have comprehensive content and images. Here is the full structured answer:
Abnormalities of the Placenta
The placenta can develop a range of structural and positional abnormalities, each with distinct clinical significance. These are grouped below into: abnormalities of position/implantation, abnormalities of invasion, abnormalities of morphology, and separation/vascular abnormalities.
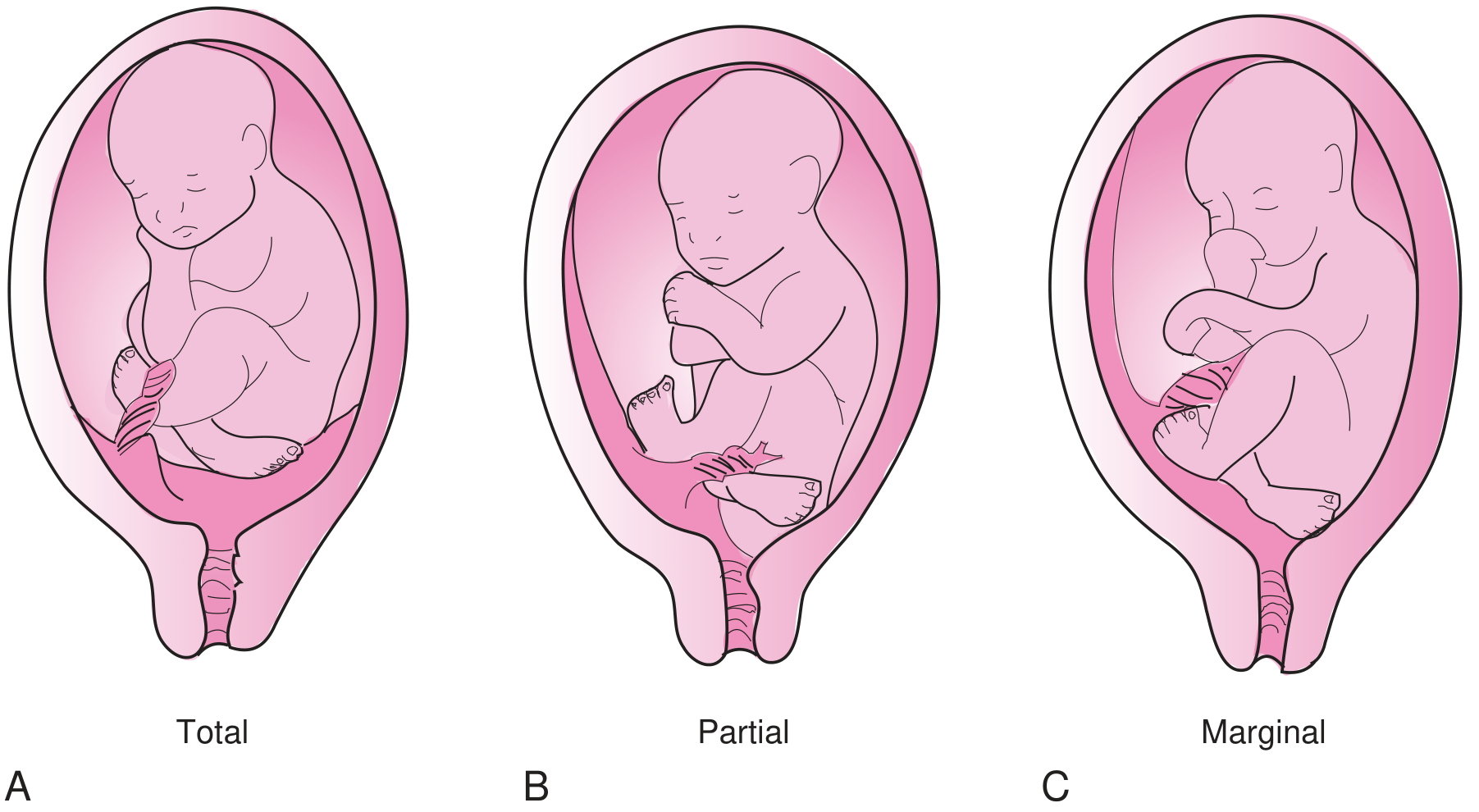
1. Placenta Previa
Definition
Placenta previa occurs when the placenta implants in the lower uterine segment such that it covers or lies near the internal cervical os. Modern guidelines define:
- Placenta previa: placenta covers the internal os
- Low-lying placenta: placental edge is within 2 cm of the internal os but does not cover it
The older subclassification into "complete," "partial," and "marginal" is no longer recommended by current guidelines, though it is still commonly used clinically for descriptive purposes.
Incidence
Affects approximately 1 in 200-250 pregnancies (~0.5% of all third-trimester pregnancies). Up to 10% of mid-trimester ultrasounds show a "previa" at that point, but 90% resolve due to placental migration (upward movement as the lower uterine segment grows). - Creasy & Resnik's Maternal-Fetal Medicine
Risk Factors
- Advanced maternal age
- Increased parity
- Prior cesarean delivery (most important)
- Prior uterine curettage
- Prior placenta previa
- Multiple gestation
- Tobacco use
- Uterine abnormalities
Clinical Features
- Painless vaginal bleeding in the third trimester - the classic hallmark
- First bleed typically at 27-32 weeks; initial bleeds are often not fatal but recur
- Abnormal fetal lie (transverse or breech) is a suspicious associated finding
- Digital vaginal examination is contraindicated until previa is excluded (may cause profuse hemorrhage)
Diagnosis
- Transabdominal ultrasound: accuracy ~93-98%
- Transvaginal ultrasound: required for accurate placental-to-os distance measurement; safe even in previa
- If placental edge >20 mm from internal os: report as normal
Associated Anomalies
- Placenta accreta spectrum
- Vasa previa
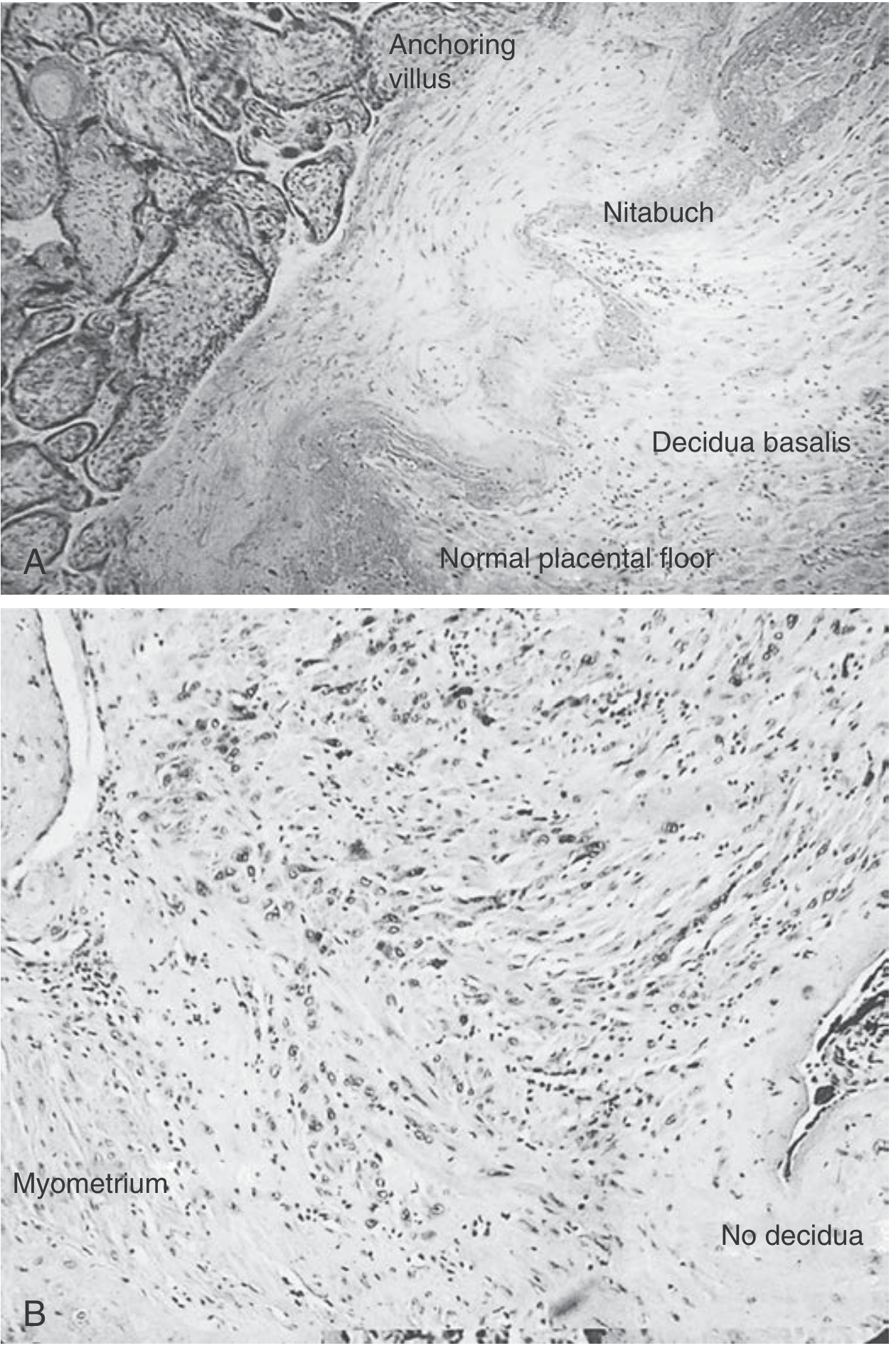
2. Placenta Accreta Spectrum (PAS)
Definition
Placenta accreta occurs when the trophoblast attaches to the myometrium without intervening decidua, due to failure of the normal Nitabuch fibrinoid layer boundary. Formerly called "morbidly adherent placenta."
Types (by depth of invasion)
| Type | Invasion | Frequency |
|---|---|---|
| Accreta | Into myometrium, not full thickness | 82% |
| Increta | Full thickness of myometrium, not beyond serosa | 12% |
| Percreta | Beyond uterine serosa, may involve bladder/pelvic organs | 6% |
Incidence & Risk Factors
- Rising incidence: approximately 1 in 300-500 pregnancies
- Most important risk factors: placenta previa + prior cesarean delivery (risk >60% with previa and 3+ cesareans)
- Other risks: prior curettage, endometrial ablation, myomectomy, in vitro fertilization, pelvic radiation, smoking, advanced maternal age
Ultrasound Diagnostic Features
- Loss of retroplacental hypoechoic zone (the normal "clear zone" representing decidua and myometrium)
- Placental lacunae: irregular hypoechoic spaces within placenta giving "Swiss cheese" appearance; turbulent, high-velocity flow on Doppler
- Bridging vessels: vessels crossing from placenta through myometrium beyond serosa
- Retroplacental myometrial thickness <1 mm
- Placental bulge: placental tissue distorting uterine contour
- Exophytic mass: placental tissue extruding beyond uterine serosa (percreta)
Ultrasound sensitivity/specificity ~80-90%, though blinded studies report lower sensitivity (~55%).
3. Abruptio Placentae (Placental Abruption)
Definition
Premature separation of a normally implanted placenta from the uterine wall before delivery of the fetus.
Pathophysiology
- Bleeding into the decidua basalis initiates separation
- Hematoma formation progressively separates the placenta, compressing vessels and compromising fetal blood supply
- Rising intrauterine pressure causes uterine tenderness, hypertonicity, and fetal distress
- Couvelaire uterus: in extensive abruption, retroplacental blood penetrates through the uterine wall into the peritoneal cavity, weakening the myometrium
Types (by bleeding pattern)
- Revealed (external): blood tracks through membranes and exits as vaginal bleeding
- Concealed: blood is trapped behind the placenta - no visible vaginal bleeding, but usually more dangerous
Incidence
- Significant abruption results in fetal mortality rate of 0.2%
- Near-complete or complete abruption: fetal death is inevitable unless immediate cesarean is performed
Clinical Features
- Painful vaginal bleeding in the third trimester - key distinguishing feature from placenta previa
- Uterine tenderness, hypertonicity
- Fetal distress
- ~80% have vaginal bleeding; ~66% have uterine/back pain; ~60% have fetal distress
- High baseline uterine pressure with frequent contractions (1-2 min apart) on monitoring
Etiology/Risk Factors
- Hypertension (40-50% of cases)
- Cocaine use (causal association - well established)
- Trauma (1.5-9.4%)
- Excessive alcohol use
- Sudden uterine decompression (e.g., delivery of first twin)
- Post-amniocentesis
- Tobacco use
Diagnosis
- Primarily a clinical diagnosis (ultrasound has high false-negative rate)
- Ultrasound negative predictive value only 63-88%
Management
- Aggressive IV fluid resuscitation
- Labs: CBC with platelets, PT/PTT, fibrinogen, D-dimer, fibrin degradation products, blood type, Kleihauer-Betke test
- Watch for DIC (disseminated intravascular coagulation) - a feared complication
- Urgent cesarean if fetal compromise
- Rh-negative mothers: administer D immune globulin
4. Vasa Previa
Definition
Fetal blood vessels (from velamentous cord insertion) traverse the fetal membranes below the presenting part over or within 20 mm of the internal cervical os, unsupported by Wharton's jelly or placental tissue.
Clinical Significance
- On membrane rupture (spontaneous or artificial), these vessels rupture, causing rapid fetal exsanguination
- Fetal mortality rate: 33-100% if undiagnosed antenatally
- Antenatal diagnosis (by Doppler ultrasound) is the key to prevention
Incidence
- 1 in 2,000-5,000 singleton deliveries
- 1 in 200-300 multifetal deliveries
Risk Factors / Associated Conditions
- Velamentous cord insertion
- Succenturiate (accessory) placental lobe
- Low-lying or previa placentation
- Multifetal gestation
- In vitro fertilization
Diagnosis
- Transvaginal color/power Doppler ultrasound showing umbilical vessels in membranes within 2 cm of endocervical os
- Pulsatile vessels felt on digital exam preceding the fetal vertex
Management
- Planned preterm cesarean delivery before membrane rupture (typically 35-37 weeks)
5. Abnormalities of Placental Morphology
Succenturiate (Accessory) Lobe / Bilobed Placenta
- A smaller or equal-sized accessory placental lobe forms adjacent to the main placenta
- Bridging vessels connect the two lobes but are often not visible on ultrasound
- Risks:
- Bridging vessels may cross the cervical os (creating vasa previa)
- Retained accessory lobe post-delivery → postpartum hemorrhage
Circumvallate Placenta
- Chorionic membranes insert at the inner edge of the placenta rather than at the periphery, giving a rolled edge and central depression
- Associated with: chronic placental abruptions, preterm delivery, fetal growth restriction
Placenta Membranacea
- Placenta is abnormally thin and membranous, covering a large portion of the uterus
- Rare but associated with: antepartum and postpartum hemorrhage, placenta previa
Key Comparison: Previa vs. Abruption
| Feature | Placenta Previa | Abruptio Placentae |
|---|---|---|
| Pain | Painless | Painful |
| Bleeding | Vaginal (bright red) | Vaginal ± concealed |
| Uterus | Soft, non-tender | Tender, rigid, hypertonic |
| Fetal presentation | Often abnormal lie | Usually normal |
| Ultrasound | Reliable (~96%) | Often false-negative |
| DIC risk | Low | High (especially with concealed) |
| Digital exam | Contraindicated | May perform cautiously |
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice
- Textbook of Family Medicine, 9th Edition
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Grainger & Allison's Diagnostic Radiology
- Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.