Make notes on thyroid anatomy 1st year MBBS
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content from Gray's Anatomy for Students, Guyton & Hall's Medical Physiology, and Junqueira's Basic Histology. Let me compile detailed, 1st year MBBS-level notes.
Thyroid Gland - Anatomy Notes (1st Year MBBS)
1. Overview
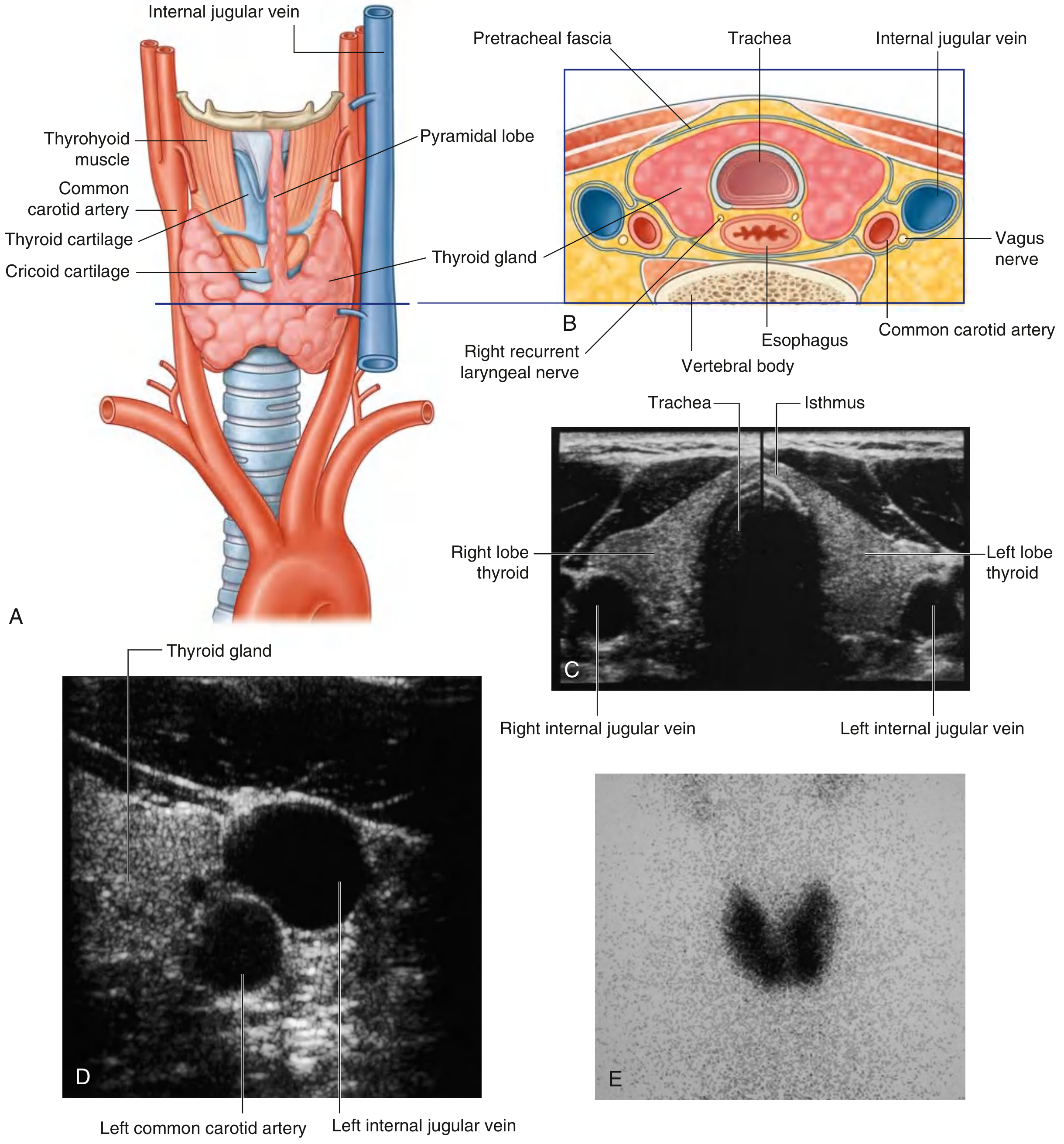
The thyroid gland is a highly vascular, butterfly-shaped endocrine gland located in the anterior neck, below and lateral to the thyroid cartilage, and anterior to the trachea. It is the largest endocrine gland in the body and the only endocrine gland that stores its secretory product extracellularly (in colloid).
2. Gross Anatomy
Shape and Parts:
- Two lateral lobes connected by an isthmus
- The lateral lobes cover the anterolateral surfaces of the:
- Trachea
- Cricoid cartilage
- Lower part of the thyroid cartilage
- The isthmus crosses the anterior surfaces of the 2nd and 3rd tracheal cartilages
- A pyramidal lobe may extend upward from the isthmus along the path of the thyroglossal duct (present in ~50% of individuals)
Dimensions (approximate):
- Weight: 25-30 g in adults
- Each lobe: ~5 cm long, 3 cm wide, 2 cm thick
Position:
- Lies in the visceral compartment of the neck
- Deep to: sternohyoid, sternothyroid, and omohyoid muscles
- Enclosed by the pretracheal layer of deep cervical fascia
Fig. 8.181 - Gray's Anatomy for Students
3. Embryology (Development)
| Feature | Detail |
|---|---|
| Origin | Median outgrowth from the floor of the pharynx (foregut endoderm) near the base of the tongue |
| Site of origin | Foramen cecum of the tongue |
| Path of migration | Thyroglossal duct - descends anterior to the hyoid bone to the final position |
| Timing | Develops early in embryonic life |
| Normal remnant | Foramen cecum (a small pit at the junction of the anterior 2/3 and posterior 1/3 of the tongue) |
Developmental anomalies:
-
Thyroglossal duct cyst - most common anomaly; midline neck swelling that moves upward on swallowing AND on protrusion of tongue (diagnostic sign)
-
Lingual thyroid - ectopic thyroid at the base of the tongue
-
Ectopic thyroid - anywhere along the path of descent
-
Gray's Anatomy for Students, p. 1157
4. Capsule and Fascia
- Covered by a true fibrous capsule
- Septa extend inward, dividing the gland into lobules
- Septa carry blood vessels, nerves, and lymphatics
- Enclosed externally by the pretracheal fascia (false capsule)
- A posterior thickening of the capsule forms the ligament of Berry (posterior suspensory ligament), which binds the thyroid to the trachea and cricoid cartilage - important surgical landmark due to its relation to the recurrent laryngeal nerve
5. Blood Supply
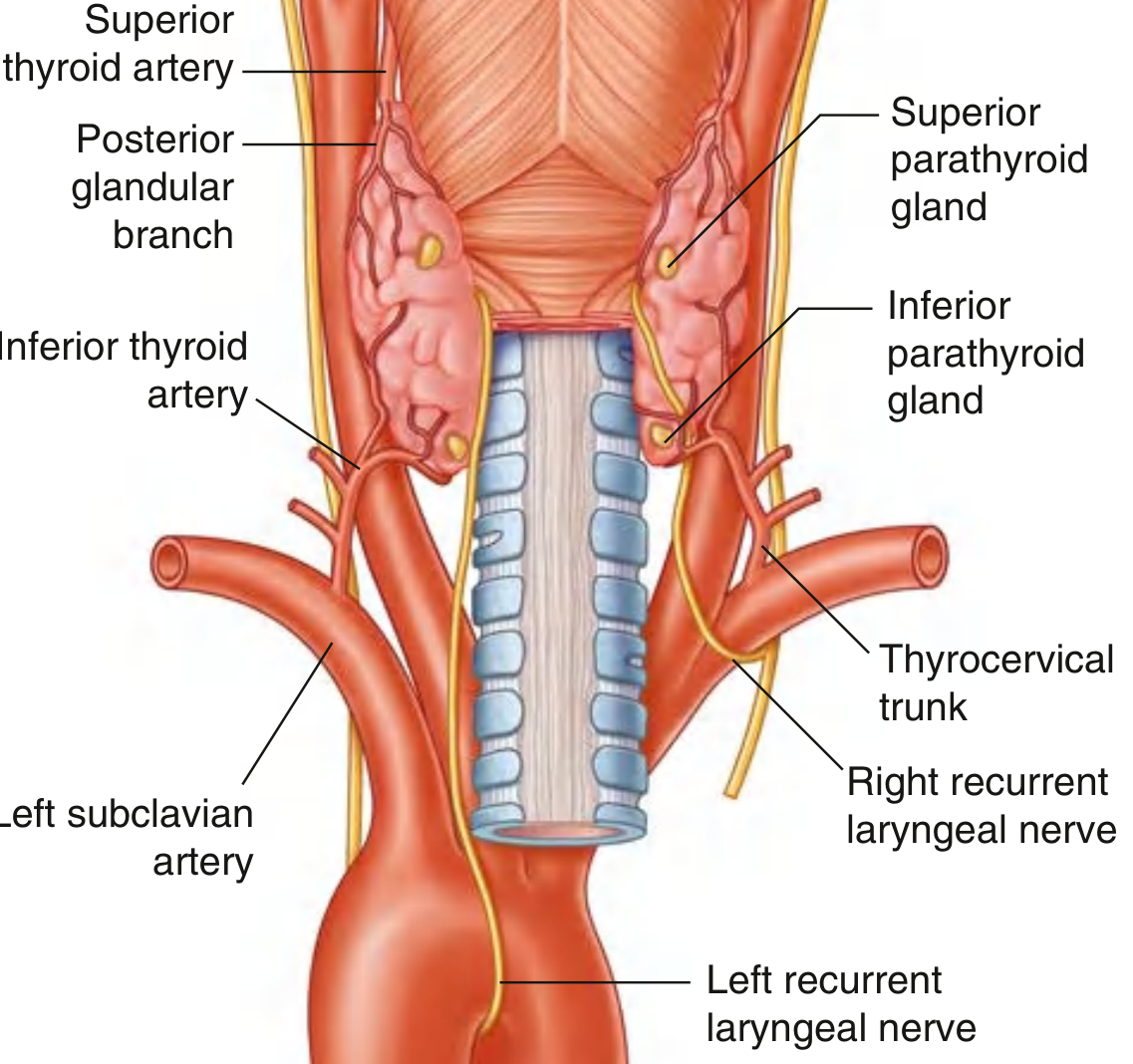
Arterial Supply (2 main arteries)
| Artery | Origin | Supply |
|---|---|---|
| Superior thyroid artery | First branch of external carotid artery | Superior pole; anterior branch anastomoses across isthmus with opposite side; posterior branch may anastomose with inferior thyroid artery |
| Inferior thyroid artery | Thyrocervical trunk (from 1st part of subclavian artery) | Inferior pole and parathyroid glands; inferior branch anastomoses with superior thyroid artery |
Occasional extra artery:
- Thyroidea ima artery - arises from the brachiocephalic trunk or arch of the aorta; ascends on the anterior trachea to the isthmus (present in ~3-10% of individuals - important during tracheostomy)
Fig. 8.183 - Gray's Anatomy for Students
Venous Drainage (3 veins)
| Vein | Drains into |
|---|---|
| Superior thyroid vein | Internal jugular vein |
| Middle thyroid vein | Internal jugular vein |
| Inferior thyroid vein | Right and left brachiocephalic veins respectively |
6. Lymphatic Drainage
- Paratracheal nodes (beside the trachea)
- Deep cervical nodes (along the internal jugular vein)
- Clinically important in spread of thyroid carcinoma
7. Nerve Supply
- Sympathetic fibers from the superior, middle, and inferior cervical ganglia (travel along the blood vessels)
- These are vasomotor - they control blood flow, not secretion
- Secretion is controlled hormonally by TSH (from the anterior pituitary)
8. Important Surgical Relations
Recurrent Laryngeal Nerve (RLN)
- Branches off the vagus nerve [CN X]
- Right RLN loops around the right subclavian artery
- Left RLN loops around the arch of the aorta (longer course)
- Both ascend in the tracheoesophageal groove
- Pass deep to the posteromedial surface of each thyroid lobe
- Closely related to the inferior thyroid artery and the ligament of Berry
- Damage during thyroidectomy causes hoarseness (unilateral) or respiratory distress (bilateral)
External Branch of Superior Laryngeal Nerve
- Runs with the superior thyroid artery near the superior pole
- Supplies the cricothyroid muscle (affects pitch of voice)
- At risk during ligation of the superior thyroid artery
Parathyroid Glands
-
2 pairs (superior and inferior) of small, ovoid, yellowish glands on the posterior surface of the thyroid lateral lobes
-
Superior parathyroids: derived from 4th pharyngeal pouch; more constant in position
-
Inferior parathyroids: derived from 3rd pharyngeal pouch; more variable in position (may be in the mediastinum)
-
Blood supply: inferior thyroid arteries (primarily)
-
At risk of inadvertent removal during thyroidectomy, causing hypoparathyroidism and hypocalcemia
-
Gray's Anatomy for Students, p. 1159-1160
9. Microscopic Anatomy (Histology)
The thyroid has a distinctive microscopic appearance, unlike any other endocrine gland.
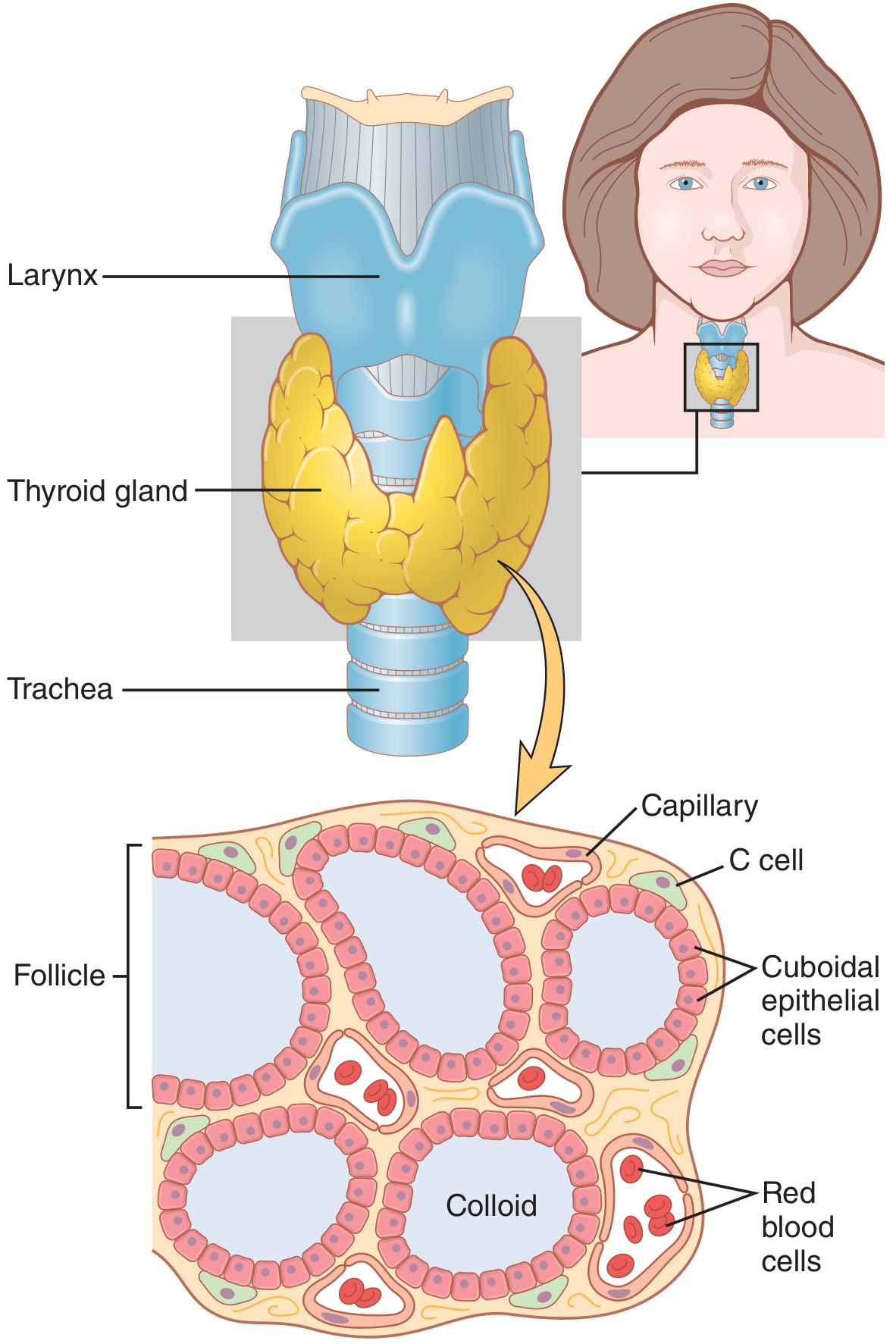
Thyroid Follicles
- The parenchyma is composed of millions of rounded follicles (100-300 µm diameter)
- Each follicle consists of:
- Simple epithelial lining (thyrocytes/follicular cells)
- Central lumen filled with gelatinous, acidophilic colloid
- Colloid = large glycoprotein thyroglobulin (660 kDa) - the precursor for T3 and T4
- Follicles are separated by sparse reticular connective tissue with fenestrated capillaries
- Enough hormone stored in follicles to supply the body for up to 3 months
Two Types of Cells
| Cell Type | Also Called | Features | Hormone |
|---|---|---|---|
| Follicular cells | Thyrocytes | Simple epithelium; shape varies - squamous (inactive) to low columnar (active); under TSH control | T3 and T4 |
| Parafollicular cells | C cells | Larger, pale-staining; found within the follicular wall or between follicles; derived from neural crest | Calcitonin (lowers plasma Ca²⁺) |
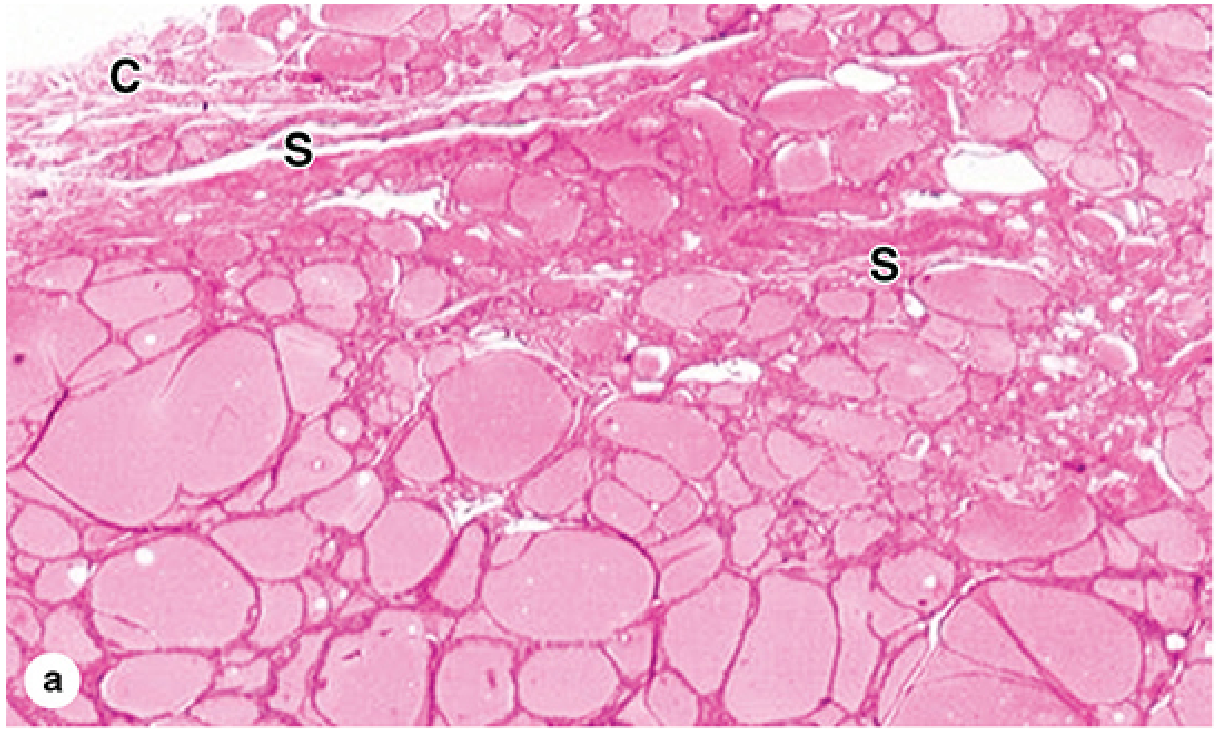
Follicular cell activity correlates with cell height:
-
Cuboidal/columnar = active (stimulated by TSH)
-
Squamous/flat = hypoactive
-
Junqueira's Basic Histology, p. 1034-1036
-
Guyton & Hall Medical Physiology, p. 930
10. Functions at a Glance
| Hormone | Cell of origin | Function |
|---|---|---|
| T3 (triiodothyronine) | Follicular cells | Regulates basal metabolic rate, growth, development; more potent form |
| T4 (thyroxine / tetraiodothyronine) | Follicular cells | Converted to T3 peripherally; less active |
| Calcitonin | Parafollicular (C) cells | Lowers blood calcium; inhibits osteoclasts |
Iodine requirement: ~50 mg/year (1 mg/week) of iodine for normal T3/T4 synthesis.
11. Clinical Correlates (Exam Favorites)
| Condition | Key Point |
|---|---|
| Thyroglossal duct cyst | Midline swelling; moves up with swallowing AND tongue protrusion; Tx: Sistrunk's operation (excise cyst + mid portion of hyoid bone) |
| Goiter | Enlarged thyroid; visible neck swelling that moves on swallowing |
| Thyroidectomy complications | Damage to RLN (hoarseness/stridor), parathyroid removal (hypocalcemia - tetany), thyroidea ima artery hemorrhage |
| Iodine deficiency | Endemic goiter; in pregnancy causes cretinism in fetus |
| Lingual thyroid | Only thyroid tissue in body - removal causes hypothyroidism; always do thyroid scan before excision |
12. Summary Table - Key Facts
| Feature | Detail |
|---|---|
| Location | Anterior neck, C5-T1 vertebral level |
| Fascia | Pretracheal fascia (false capsule) |
| Arterial supply | Superior thyroid a. (ext. carotid) + Inferior thyroid a. (thyrocervical trunk) |
| Venous drainage | Superior & middle → IJV; Inferior → brachiocephalic veins |
| Lymphatics | Paratracheal + deep cervical nodes |
| Isthmus level | 2nd-3rd tracheal cartilage |
| Embryological origin | Foramen cecum; thyroglossal duct |
| Histology | Colloid-filled follicles; thyrocytes + C cells |
| Key surgical nerve | Recurrent laryngeal nerve (RLN) |
Sources:
- [Gray's Anatomy for Students](Gray's Anatomy for Students), Chapter 8 (Neck), pp. 1157-1160
- [Junqueira's Basic Histology: Text and Atlas, 17e](Junqueira's Basic Histology), pp. 1034-1036
- [Guyton & Hall Textbook of Medical Physiology](Guyton and Hall Textbook of Medical Physiology), Chapter 77, p. 930
This is a shared conversation. Sign in to Orris to start your own chat.