
IMG-20260401-WA0006.jpg
Answer
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have enough from the textbooks to answer all three questions comprehensively.
Answers
Question 1: What is A, B, C?
From the image:
- A — Cervical (Pap) smear: A spatula/brush is used to collect cells from the ectocervix and endocervical canal onto a glass slide (or into liquid). The image shows the wooden spatula and glass slide alongside a cross-section of the cervix being sampled.
- B — Colposcopy: A binocular magnifying instrument (colposcope) that illuminates and magnifies the cervix. Biopsy forceps are used to take targeted biopsies of abnormal areas identified under colposcopic visualization.
- C — Cold cone biopsy (Cervical conization): A large cone-shaped area of tissue is excised around the cervix — both diagnostic and therapeutic. The image shows the cervix viewed through a speculum with the patient in lithotomy position and the cone-shaped excision being performed.
Question 2: Give the alternative to A (Pap smear), and what is it used for?
Alternative: Liquid-Based Cytology (LBC) — e.g., ThinPrep or SurePath.
Instead of smearing cells directly onto a glass slide, the spatula/brush is rinsed into a vial of liquid preservative. The advantages over conventional Pap smear:
- Reduces obscuring blood and mucus artifacts
- Allows co-testing for HPV from the same sample
- Lower unsatisfactory specimen rates
- Can be used for additional molecular testing (e.g., chlamydia, gonorrhoea)
Both conventional Pap smear and liquid-based cytology are used for cervical cancer screening — detecting squamous and glandular intraepithelial lesions (CIN / LSIL / HSIL) caused predominantly by high-risk HPV.
Question 3: A Pap smear was done for a patient showing HSIL — what is the next step?
Next step: Colposcopy (with directed biopsy)
Per the Bethesda classification, women with HSIL on Pap smear should undergo colposcopy to evaluate the extent and severity of neoplasia. The goals are:
- Visualize the entire transformation zone (TZ) including the squamocolumnar junction (SCJ)
- Apply acetic acid → identify acetowhite areas (abnormal areas turn white)
- Take directed biopsies of all abnormal areas
- Perform endocervical curettage (ECC) if the TZ cannot be fully visualized
If colposcopy is unsatisfactory (entire TZ/SCJ cannot be seen, lesion extends into canal, or there is a discrepancy between colposcopic impression and cytology), the next step is cold knife cone biopsy (cervical conization) or LEEP (Loop Electrosurgical Excision Procedure) — which is both diagnostic and therapeutic for HSIL/CIN 2–3.
Summary algorithm: HSIL on Pap → Colposcopy + biopsy → If unsatisfactory colposcopy or confirmed CIN 2–3 → Cone biopsy / LEEP
(Creasy & Resnik's Maternal-Fetal Medicine, p. 1351; Pfenninger & Fowler's Procedures for Primary Care, p. 960)
Latest guidelines for tb
Finding Sources
Searching PubMed
tuberculosis treatment guidelines
Searching the Web
WHO tuberculosis treatment guidelines 2024 2025
Finding Sources
Reading Article
PMID: 40693952
Reading Web Page
https://www.who.int/news/item/15-04-2025-who-announces-landm…
Reading File
Searching the Web
WHO TB guidelines April 2025 BDLLfxC MDR TB regimen details latent TB
Here is a comprehensive summary of the latest TB treatment guidelines (2025), incorporating the WHO April 2025 consolidated guidelines and the January 2025 ATS/CDC/ERS/IDSA update.
Tuberculosis: Latest Guidelines (2025)
Key Guideline Sources
- WHO Consolidated Guidelines on TB, Module 4: Treatment and Care — April 2025 (most up-to-date, consolidates all prior modules)
- ATS/CDC/ERS/IDSA Clinical Practice Guideline — January 2025 (PMID: 40693952)
1. Latent TB Infection (LTBI) Treatment
No changes since 2020. Preferred options (shortest, most effective):
| Regimen | Duration | Notes |
|---|---|---|
| 3HP: Isoniazid + Rifapentine | Weekly × 12 doses (3 months) | Preferred — adults, children >2 yrs, HIV+ |
| 1HP: Isoniazid + Rifapentine daily | 1 month | HIV-positive patients |
| 4R: Rifampin alone | Daily × 4 months | Alternative; avoid if HIV+ on ART (drug interactions) |
| 3HR: Isoniazid + Rifampin | Daily × 3 months | Alternative |
| 6–9H: Isoniazid alone | Daily × 6–9 months | Acceptable but less preferred |
Pyridoxine (vitamin B6) 25–50 mg/day should be co-administered with any isoniazid-containing regimen.
2. Drug-Susceptible (DS) Active TB — Adults & Adolescents ≥12 yrs
✅ NEW: Preferred 4-Month Regimen (Conditional Recommendation, Moderate Evidence)
2HPZM / 2HPM (total 17 weeks):
| Drug | Dose | Duration |
|---|---|---|
| Isoniazid (H) | 300 mg daily | 17 weeks |
| Rifapentine (P) | 1,200 mg daily | 17 weeks |
| Pyrazinamide (Z) | Weight-based (1,000–2,000 mg) | 8 weeks |
| Moxifloxacin (M) | 400 mg daily | 17 weeks |
Based on the TB-SEQUEL / TBTC Study 31 showing non-inferiority to 6-month HRZE at 12 months.
Standard 6-Month Regimen (Still acceptable as alternative)
2HRZE / 4HR:
| Phase | Drugs | Duration |
|---|---|---|
| Intensive | Isoniazid + Rifampin + Pyrazinamide + Ethambutol | 2 months |
| Continuation | Isoniazid + Rifampin | 4 months |
Extend continuation to 7 months (total 9 months) if:
- Cavitary disease on CXR
- Sputum culture still positive at 2 months
- Pyrazinamide not completed in intensive phase
3. Drug-Susceptible TB — Children (Non-Severe)
NEW: 4-Month Regimen for Children with Non-Severe TB
| Phase | Drugs | Duration |
|---|---|---|
| Intensive | Isoniazid + Rifampin + Pyrazinamide ± Ethambutol | 8 weeks |
| Continuation | Isoniazid + Rifampin | 8 weeks |
Non-severe = smear-negative, no extensive disease, no systemic symptoms
4. Drug-Resistant TB (MDR/RR-TB)
🆕 LANDMARK: New WHO April 2025 Recommendation — BDLLfxC (6 months, all-oral)
The biggest change in the April 2025 WHO guidelines. Based on the BEAT-TB and endTB clinical trials:
| Drug | Regimen Code |
|---|---|
| Bedaquiline | B |
| Delamanid | D |
| Linezolid | L |
| Levofloxacin | Lfx |
| Clofazimine | C |
- Recommended for MDR/RR-TB with or without fluoroquinolone resistance (pre-XDR-TB)
- All-oral, 6 months
- Major improvement over the previous 18–20-month injectable-containing regimens
Pre-XDR / XDR-TB: BPaL or BPaLM (ATS/CDC/ERS/IDSA 2025)
| Drug | Dose | Duration |
|---|---|---|
| Bedaquiline | 400 mg daily ×2 wks → 200 mg 3×/wk ×24 wks | 26 weeks |
| Pretomanid | 200 mg daily | 26 weeks |
| Linezolid | 600 mg daily | 26 weeks |
| + Moxifloxacin (if FQ-susceptible = BPaLM) | 400 mg daily | 26 weeks |
Modified 9-Month All-Oral Regimen (MDR/RR-TB, FQ-susceptible)
Still recommended where FQ resistance is excluded.
5. Special Situations
| Scenario | Key Guidance |
|---|---|
| HIV co-infection | Start ART within 2–8 weeks of TB treatment; caution with rifamycin–ART interactions |
| TB meningitis | New 2026 Lancet Infectious Diseases guideline (PMID: 40840485); intensified regimens with dexamethasone |
| Pregnancy | Avoid pyrazinamide in some guidelines; standard HRZE generally used; streptomycin contraindicated |
| Monitoring | DOT (directly observed therapy) or video-DOT (vDOT) — equivalent efficacy per CDC 2023 |
| Culture conversion | Failure to convert at 2 months → investigate drug resistance |
6. Diagnosis (for context)
- Preferred: Xpert MTB/RIF (WHO-recommended rapid diagnostic) — simultaneous TB detection + rifampin resistance
- Smear microscopy, culture (gold standard), IGRA/TST for LTBI
- Drug susceptibility testing (DST) mandatory to guide DR-TB regimens
Bottom line of 2025 updates:
- DS-TB: 4-month rifapentine-moxifloxacin regimen is now a valid alternative to the standard 6-month HRZE
- MDR/RR-TB: New all-oral 6-month BDLLfxC regimen (WHO April 2025) — landmark change
- XDR/pre-XDR-TB: BPaL/BPaLM remains the standard
- LTBI: No changes — 3HP preferred
(Harrison's Principles of Internal Medicine 22E, p. 1422; ATS/CDC/ERS/IDSA 2025 Guideline, PMID 40693952; WHO Module 4 April 2025)
TACO AND TRALI
Finding Sources
Finding Sources
Searching the Web
TACO vs TRALI transfusion reactions comparison 2024 2025 guidelines
Reading File
Reading File
Reading File
TACO vs TRALI — Comprehensive Comparison
Both are life-threatening pulmonary complications of blood transfusion presenting within 6 hours with bilateral pulmonary infiltrates and hypoxia — but they have completely different mechanisms, management, and outcomes.
TACO — Transfusion-Associated Circulatory Overload
Definition
Hydrostatic (cardiogenic) pulmonary edema caused by volume/fluid overload from transfused blood products. Currently the #1 cause of transfusion-related death.
Pathophysiology
- Excessive transfusion volume → ↑ hydrostatic pressure in pulmonary capillaries → transudative pulmonary edema
- Aggravated by poor cardiac reserve, renal insufficiency
Risk Factors
| Category | Factors |
|---|---|
| Patient | Age >60, female sex, CHF, CKD, low body weight, pre-existing lung disease |
| Transfusion | Rapid infusion rate, large volume, multiple units, plasma transfusion |
Clinical Features
- Acute respiratory distress within 6 hours of transfusion
- Hypertension (key distinguisher from TRALI)
- Tachycardia, tachypnea
- S3 gallop, elevated JVP, peripheral oedema
- Bilateral crackles/rales
- Positive fluid balance
Investigations
- CXR: bilateral infiltrates + cardiomegaly, pleural effusions
- ↑ BNP / NT-proBNP (strongly supports TACO)
- PCWP >18 mmHg (elevated)
- Pulmonary edema fluid: transudate (low protein)
- Normal/↑ WBC
Diagnosis (NHSN Criteria) — ≥3 of the following within 6h of transfusion:
- Acute respiratory distress (new or worsened)
- Radiographic pulmonary edema
- Elevated CVP
- Evidence of left heart failure
- Elevated BNP
- Positive fluid balance
Management
- Stop/slow the transfusion immediately
- IV diuretics (furosemide) — hallmark treatment; rapid improvement expected
- Supplemental O₂ / NIV (BiPAP/CPAP)
- Upright positioning
- Fluid restriction
TRALI — Transfusion-Related Acute Lung Injury
Definition
Non-cardiogenic pulmonary edema (ALI) caused by immune-mediated neutrophil activation in the pulmonary microvasculature after transfusion of plasma-containing blood products (FFP > platelets > pRBCs).
Pathophysiology — "Two-Hit" Model
- Hit 1 (priming): Recipient's neutrophils are primed by underlying illness (sepsis, surgery, shock, smoking)
- Hit 2 (activation): Donor anti-leukocyte antibodies (anti-HLA class I/II, anti-HNA) in transfused product bind to primed neutrophils → neutrophil degranulation → capillary permeability → exudative pulmonary edema
- Multiparous female donors are the most common source (antibodies formed against paternal HLA antigens during pregnancy) — exclusion of multiparous female plasma donors has significantly reduced TRALI incidence
Risk Factors
| Category | Factors |
|---|---|
| Recipient | Sepsis, surgery, trauma, shock, chronic alcohol abuse, smoking, mechanical ventilation, hematologic malignancy |
| Donor | Multiparous female, prior transfusions, high-titer anti-HLA antibodies |
| Product | FFP (highest risk), platelets, pRBCs; prolonged storage |
Clinical Features
- Dramatic sudden onset of respiratory failure during or within 6 hours of transfusion
- Hypotension (key distinguisher from TACO)
- Fever (immune-mediated)
- Severe hypoxia (PaO₂/FiO₂ ≤300)
- No signs of volume overload
Investigations
- CXR: bilateral diffuse infiltrates, no cardiomegaly, no pleural effusions
- PCWP <18 mmHg (normal — no left heart failure)
- Normal/low BNP
- Transient leukopenia (neutrophil sequestration in lungs)
- Pulmonary edema fluid: exudate (high protein)
- Donor testing may reveal anti-HLA or anti-HNA antibodies
TRALI Definition (Delphi Consensus)
- Type I: No ARDS risk factors + acute hypoxia (PaO₂/FiO₂ ≤300 or SpO₂ <90% on RA) + bilateral infiltrates + no LAH + within 6h of transfusion
- Type II: Pre-existing mild ARDS (PaO₂/FiO₂ 200–300) or ARDS risk factor present, but clear respiratory deterioration attributable to transfusion
Management
- Stop transfusion immediately
- Supportive care — oxygen, mechanical ventilation if needed
- Diuretics are NOT effective (not volume overload) and may worsen hypotension
- Vasopressors if hypotensive
- Report to blood bank → test donor for anti-HLA/HNA antibodies
- Discard implicated unit; avoid same donor products
Side-by-Side Comparison
| Feature | TACO | TRALI |
|---|---|---|
| Mechanism | Volume overload (hydrostatic) | Immune-mediated (non-cardiogenic) |
| Timing | Within 6–12 hours | During or within 6 hours |
| Blood pressure | Hypertension | Hypotension |
| Temperature | Normal | Fever |
| BNP/NT-proBNP | Elevated | Normal |
| PCWP | >18 mmHg | <18 mmHg |
| Edema fluid | Transudate | Exudate |
| WBC | Normal or elevated | Transient leukopenia |
| Chest X-ray | Bilateral infiltrates + cardiomegaly/effusions | Bilateral infiltrates, no cardiomegaly |
| Response to diuretics | Rapid improvement | No response |
| Cardiac function | Impaired (↑ CVP, S3) | Normal |
| Key treatment | Diuretics | Supportive care / mechanical ventilation |
| Mortality | Leading cause of transfusion death | 5% (uncomplicated) → up to 67% (critically ill) |
| Most common product | Any (high volume) | FFP > platelets > pRBCs |
Prevention
| TACO | TRALI |
|---|---|
| Restrictive transfusion strategy | Exclude multiparous female plasma donors |
| Slow infusion rates | Use male-predominant or never-pregnant plasma |
| Pre-emptive diuretics in high-risk patients | Screen donors for anti-HLA/HNA antibodies |
| Close monitoring of fluid balance | Avoid unnecessary plasma-rich products |
Memory hook: TACO = Too much fluid → HYPERtension, treat with diuretics. TRALI = Immune reaction → HYPOtension, no diuretics.
(Murray & Nadel's Respiratory Medicine, p. 2989–2990; Robbins & Kumar Basic Pathology, p. 3206–3219)
Heart
Asking for Preferences
Finding Sources
Searching Images
heart anatomy diagram chambers valves
Finding Sources
Loading Image
Finding Sources
Searching Images
cardiac conduction system SA node AV node bundle of His
Reading File
Loading Image
Since "Heart" is broad, here is a comprehensive overview covering anatomy, physiology, blood flow, conduction, and coronary supply — the essential foundation for all of cardiac medicine.
The Heart — Complete Overview
1. Anatomy & Chambers
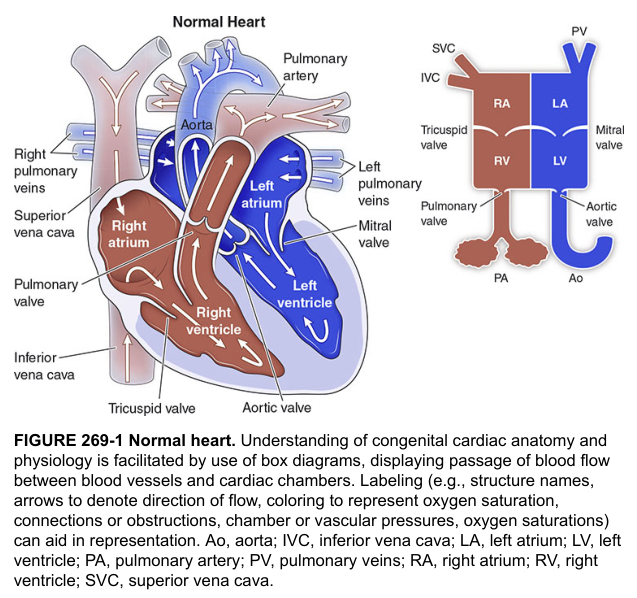
The heart has 4 chambers divided into right and left sides by the interventricular and interatrial septa:
| Chamber | Function | Wall Thickness |
|---|---|---|
| Right Atrium (RA) | Receives deoxygenated blood from SVC + IVC | Thin |
| Right Ventricle (RV) | Pumps to pulmonary circulation (low pressure) | Moderate |
| Left Atrium (LA) | Receives oxygenated blood from pulmonary veins | Thin |
| Left Ventricle (LV) | Pumps to systemic circulation (high pressure) | Thick (3× RV) |
2. Valves
| Valve | Location | Type | Prevents |
|---|---|---|---|
| Tricuspid | RA → RV | AV valve (3 leaflets) | Back-flow to RA |
| Pulmonary | RV → Pulmonary artery | Semilunar | Back-flow to RV |
| Mitral (Bicuspid) | LA → LV | AV valve (2 leaflets) | Back-flow to LA |
| Aortic | LV → Aorta | Semilunar | Back-flow to LV |
Mnemonic: "Try Pulling My Aorta" (Tricuspid → Pulmonary → Mitral → Aortic, right-to-left flow)
3. Blood Flow — Dual Circulation
Systemic veins → SVC/IVC → RA → [Tricuspid] → RV → [Pulmonary valve]
→ Pulmonary artery → Lungs (gas exchange)
→ Pulmonary veins → LA → [Mitral valve] → LV → [Aortic valve]
→ Aorta → Systemic circulation
- Right side = low-pressure pulmonary circuit (~25/10 mmHg)
- Left side = high-pressure systemic circuit (~120/80 mmHg)
4. Cardiac Conduction System
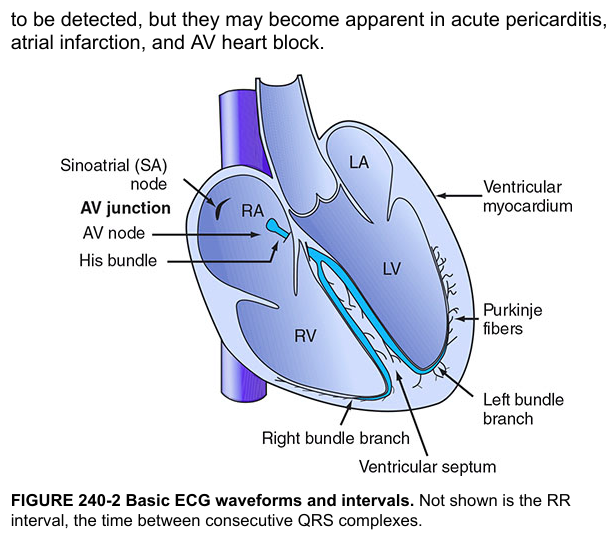
| Structure | Location | Rate | Function |
|---|---|---|---|
| SA Node | Right atrium (near SVC) | 60–100 bpm | Primary pacemaker |
| AV Node | Inferior atrial septum (Triangle of Koch) | 40–60 bpm | Delays impulse → allows atrial emptying |
| Bundle of His | Interventricular septum | — | Conducts to ventricles |
| Right + Left Bundle Branches | Septum | — | Distribute to each ventricle |
| Purkinje Fibers | Ventricular walls | 20–40 bpm | Rapid conduction → synchronous contraction |
ECG correlation:
- P wave → atrial depolarization (SA node activity)
- PR interval → AV node delay (0.12–0.20 s)
- QRS → ventricular depolarization (<0.12 s)
- T wave → ventricular repolarization
5. Coronary Circulation
The heart receives its own blood supply from two coronary arteries arising from the aortic root (behind aortic valve cusps):
Left Coronary Artery (LCA)
- Left Anterior Descending (LAD) — "widow maker"
- Supplies: anterior LV, interventricular septum (2/3), apex
- Left Circumflex (LCx)
- Supplies: lateral and posterior LV, left atrium
Right Coronary Artery (RCA)
- Supplies: RV, RA, inferior LV, SA node (60%), AV node (85–90%)
- Gives posterior descending artery (PDA) in right-dominant circulation (~85% of people)
Coronary blood flow is predominantly diastolic — the LV compresses its own vessels during systole, so perfusion occurs when the heart relaxes.
6. Cardiac Physiology
The Cardiac Cycle
| Phase | Event |
|---|---|
| Systole | Ventricular contraction → ejects blood |
| Diastole | Ventricular relaxation → fills with blood |
| Isovolumetric contraction | All valves closed, pressure rising |
| Isovolumetric relaxation | All valves closed, pressure falling |
Key Parameters
| Parameter | Normal Value |
|---|---|
| Stroke volume (SV) | 70 mL/beat |
| Heart rate (HR) | 60–100 bpm |
| Cardiac output (CO = SV × HR) | ~5 L/min |
| Ejection fraction (EF) | ≥55% |
| End-diastolic volume (EDV) | ~120 mL |
| End-systolic volume (ESV) | ~50 mL |
Frank-Starling Law
↑ Preload (venous return) → ↑ myocardial stretch → ↑ force of contraction → ↑ stroke volume
Determinants of Cardiac Output
- Preload (filling pressure / EDV)
- Afterload (resistance against which heart pumps = SVR)
- Contractility (intrinsic myocardial force)
- Heart rate
7. Pericardium
- Fibrous pericardium: tough outer layer, anchors heart
- Serous pericardium: visceral (epicardium) + parietal layers with ~20–50 mL pericardial fluid for lubrication
- Pathology: pericarditis (inflammation), cardiac tamponade (fluid compression)
8. Cardiac Muscle (Myocardium) — Key Features
- Involuntary, striated muscle
- Connected by intercalated discs with gap junctions → functions as a syncytium
- Action potential plateau phase (Phase 2) due to slow Ca²⁺ influx — prolongs contraction, prevents tetany
- Energy: primarily fatty acids (60–70%), glucose, lactate; relies almost entirely on aerobic metabolism
- Capillary density: >3,000/mm² (much higher than skeletal muscle)
(Medical Physiology — Boron & Boulpaep, p. 823; Harrison's Principles of Internal Medicine 22E; Fuster & Hurst's The Heart 15E)
This is a shared conversation. Sign in to Orris to start your own chat.