Renal Cell Carcinoma
Reading File
Finding Sources
Searching PubMed
"renal cell carcinoma"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent. I now have comprehensive content covering all major aspects of RCC. Let me compile the full answer.
Renal Cell Carcinoma (RCC)
Definition and Overview
Renal cell carcinoma is not a single entity but a group of distinguishable epithelial neoplasms arising from the renal tubular epithelium, each with a strong relationship between its morphologic and genetic features. It represents 80-85% of all primary malignant renal neoplasms and 2-3% of all adult cancers, accounting for roughly 65,000-75,000 new diagnoses per year in the United States and approximately 14,000 deaths annually.
- 6th most common cancer in men, 9th in women
- Male:female ratio of ~2:1 to 3:1
- Peak incidence in the 6th-7th decade
- Highest incidence in Black Americans; lowest in Asians/Pacific Islanders
- Only 4-6% of cases are familial; the vast majority are sporadic
Risk Factors
| Risk Factor | Notes |
|---|---|
| Cigarette smoking | Most established modifiable risk |
| Obesity | Risk rises with increasing BMI |
| Hypertension | Independent risk factor |
| Diuretic use | Hard to separate from hypertension risk |
| Chronic dialysis / Acquired polycystic disease | 30-fold increased risk |
| Horseshoe kidney, polycystic kidney disease | Pre-existing renal injury |
| Occupational cadmium exposure | Less common |
| Genetic syndromes (VHL, HLRCC, BHD, SDH) | Familial forms |
Classification and Pathology
RCC is classified by morphology, growth pattern, and molecular genetics. The three main subtypes:
1. Clear Cell Carcinoma (65% of RCC; 90% of metastases)
- Derived from the proximal convoluted tubule
- Grossly: solitary, well-circumscribed, golden yellow due to cytoplasmic lipid
- Histologically: cells with clear cytoplasm arranged in nests surrounded by delicate vasculature
- Molecular hallmark: loss/inactivation of both VHL alleles on chromosome 3p25
- VHL normally causes oxygen-dependent degradation of HIFs (hypoxia-inducible factors)
- Loss of VHL --> HIF stabilization even in normoxia --> upregulation of VEGF --> tumor vascularization
- Also involves loss-of-function mutations in histone methylation regulators (epigenomic changes)
- Frequently invades the renal vein (and can extend into the inferior vena cava)
- Most virulent subtype
2. Papillary RCC (10-15%; largely indolent)
- Characteristic papillary growth pattern
- Frequently multifocal and bilateral
- Often presents as early-stage tumor
- Molecular hallmark: increased MET signaling (chromosome 7q)
- Sporadic: increased MET copy number or somatic activating MET mutations
- Familial: germline activating MET mutations
- Hypointense on T2-weighted MRI; hypoenhancing on all post-contrast phases
- Lower metastatic potential than clear cell
3. Chromophobe RCC (~5%; indolent)
- Neoplastic cells have eosinophilic cytoplasm with prominent cell membranes (like plant cells)
- Avid enhancement in corticomedullary phase on CT/MRI, but less than clear cell
- Better prognosis than clear cell or papillary
- Associated with Birt-Hogg-Dube (BHD) syndrome
Other Subtypes
- Collecting duct carcinoma: very rare, aggressive
- Oncocytoma: benign (10% of all renal tumors), mahogany-brown color, central stellate scar; cannot be reliably distinguished from RCC on imaging
- Sarcomatoid differentiation: can occur in any subtype; indicates aggressive biology and poor prognosis
Hereditary Syndromes
| Syndrome | Gene / Locus | RCC Subtype | Features |
|---|---|---|---|
| Von Hippel-Lindau (VHL) | VHL, 3p25 (AD) | Clear cell (bilateral, multiple) | Hemangioblastomas (cerebellum/retina), pheochromocytoma, pancreatic cysts |
| Hereditary Papillary RCC | MET, 7q (AD) | Papillary type 1 (bilateral, multiple) | No extrarenal manifestations |
| Hereditary Leiomyomatosis RCC (HLRCC) | Fumarate hydratase (FH), 1q42-43 (AD) | Papillary type 2 (solitary, aggressive) | Cutaneous + uterine leiomyomas; collecting duct carcinoma possible |
| Birt-Hogg-Dube (BHD) | Folliculin (FLCN), 17p (AD) | Chromophobe / oncocytic (bilateral) | Fibrofolliculomas, pulmonary cysts, spontaneous pneumothorax |
| SDH-RCC | SDHA/B/C/D, SDHAF2 | SDH-deficient RCC | Pheochromocytoma, paraganglioma; early onset (<40 yrs) |
Clinical Presentation
Most tumors (~50%) are now detected incidentally on CT or ultrasound performed for unrelated reasons. The classic triad of hematuria + flank pain + palpable mass is now seen in <10% of patients and usually indicates advanced disease.
Common symptoms and signs:
| Finding | Frequency |
|---|---|
| Anemia | 52% |
| Hepatic dysfunction (Stauffer syndrome) | 32% |
| Weight loss | 23% |
| Hypoalbuminemia | 20% |
| Malaise | 19% |
| Hypercalcemia | 13% |
| Anorexia | 11% |
| Thrombocytosis | 9% |
| Fever / Night sweats | 8% |
| Erythrocytosis | 4% |
| Hypertension | 3% |
Paraneoplastic syndromes are a hallmark of RCC:
- Hypercalcemia (~20%): from PTH-rP, IL-6-driven osteoclast activation, or bony mets
- Erythrocytosis: ectopic erythropoietin production
- Hypertension: excess renin secretion
- Stauffer syndrome: reversible hepatic dysfunction without hepatic metastases (resolves after nephrectomy)
- Fever of unknown origin: from cytokine (IL-6, IL-1) secretion
RCC is also known for venous extension - tumor thrombus can grow into the renal vein and up through the inferior vena cava into the right atrium, without necessarily carrying a worse prognosis stage-for-stage.
Imaging
CT (multiphasic contrast-enhanced) is the standard for characterization:
| Subtype | Enhancement Pattern |
|---|---|
| Clear cell | Avid corticomedullary enhancement, becomes hypoenhancing in nephrographic phase |
| Chromophobe | Avid enhancement, but less than clear cell |
| Papillary | Hypoenhancing on all post-contrast phases; hypointense on T2 MRI |
MRI is preferred when CT contrast is contraindicated (renal insufficiency) and is more sensitive for detecting enhancement within cystic lesions (subtraction imaging).
Bosniak Classification is used for cystic lesions:
- Category I/II: benign, no follow-up needed
- Category IIF: follow-up required
- Category III: surgical exploration (51% malignant)
- Category IV: surgical resection (>90% malignant)
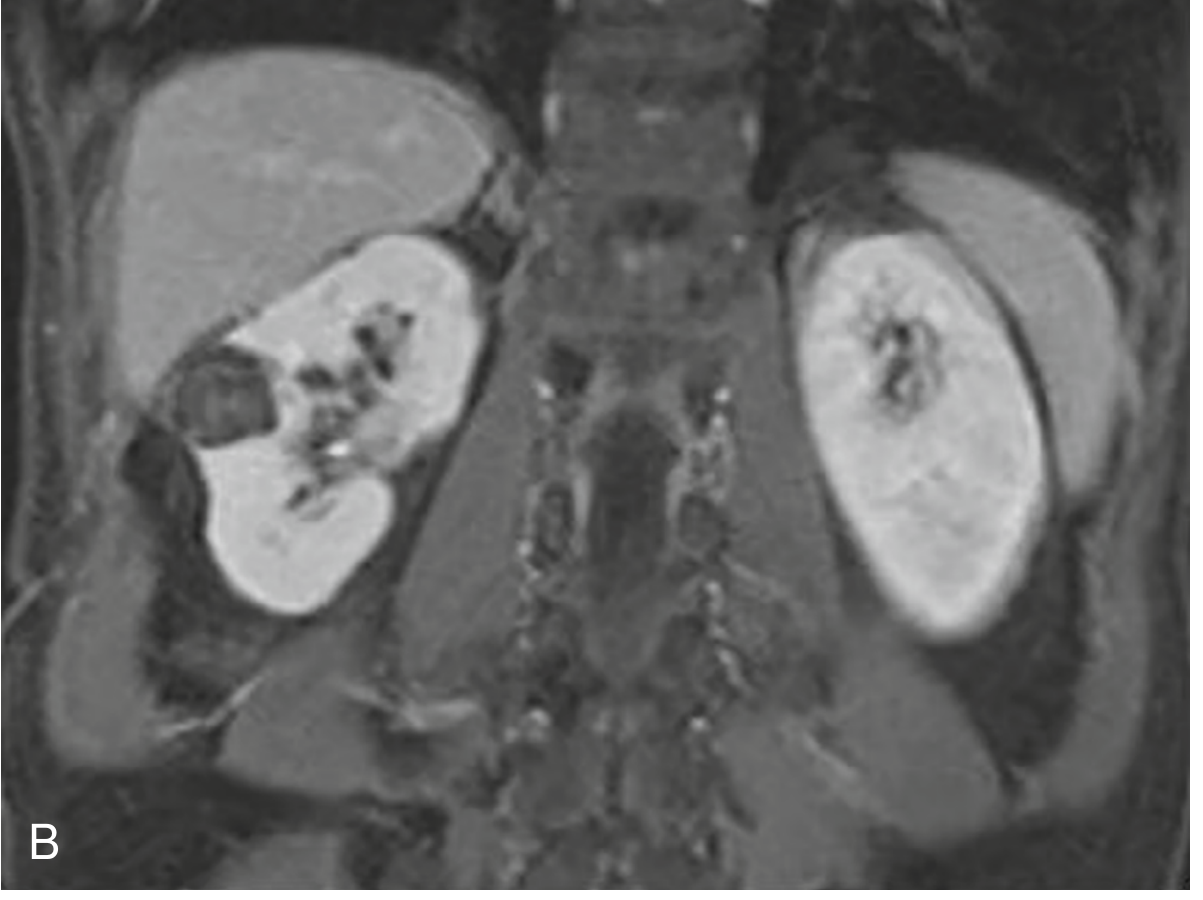
Below is a coronal MRI showing bilateral renal masses in a patient with bilateral RCC (as seen in VHL disease):
Staging (AJCC 8th Edition)
| Stage | T | N | M | Description |
|---|---|---|---|---|
| I | T1 | N0 | M0 | Tumor ≤7 cm, confined to kidney |
| II | T2 | N0 | M0 | Tumor >7 cm, confined to kidney |
| III | T1-2 | N1 | M0 | Regional lymph node involvement |
| III | T3a-c | N0-1 | M0 | Perinephric/renal vein/IVC extension below diaphragm |
| IV | T4 | Any N | M0 | Beyond Gerota fascia / adrenal invasion |
| IV | Any T | Any N | M1 | Distant metastasis |
- T3a: invasion of renal sinus fat or perinephric fat
- T3b: tumor thrombus in renal vein or IVC below diaphragm
- T3c: tumor thrombus in IVC above diaphragm or into right atrium
- ~30% of patients present with metastatic (Stage IV) disease
Common metastatic sites: lung (most common), bone, liver, brain, adrenal glands, and contralateral kidney.
Treatment
Localized Disease (Stages I-III)
Surgery is the only curative modality. RCC is resistant to conventional radiation therapy and cytotoxic chemotherapy.
- Partial nephrectomy (nephron-sparing): preferred for T1 tumors (≤7 cm) and when kidney preservation is important (solitary kidney, bilateral tumors, impaired renal function)
- Radical nephrectomy: standard for larger or more locally advanced tumors; can be performed laparoscopically or open (flank, transperitoneal, or transthoracic approach); ipsilateral adrenal gland often removed; lymph node dissection is optional and controversial
Adjuvant therapy (for high-risk patients post-nephrectomy):
- Sunitinib (VEGF-targeted TKI) - adjuvant use in high-risk patients
- Pembrolizumab (anti-PD-1 checkpoint inhibitor) - superior disease-free survival in high-risk patients after resection
Metastatic Disease (Stage IV)
Approximately 30% present with metastases; another 20-30% relapse after surgery.
Current first-line systemic therapy is combination immunotherapy + targeted therapy:
| Regimen | Notes |
|---|---|
| Nivolumab + Ipilimumab (anti-PD-1 + anti-CTLA-4) | Intermediate/poor risk; superior OS vs sunitinib |
| Nivolumab + Cabozantinib (anti-PD-1 + TKI) | Improved PFS and OS vs sunitinib |
| Pembrolizumab + Axitinib (anti-PD-1 + VEGFR TKI) | Superior PFS/OS vs sunitinib, all risk groups |
| Pembrolizumab + Lenvatinib (anti-PD-1 + TKI) | Superior PFS/OS vs sunitinib, all risk groups |
| Avelumab + Axitinib (anti-PD-L1 + TKI) | Option for favorable risk |
Key principle: Pembrolizumab + TKI (axitinib or lenvatinib) is recommended regardless of risk group. Nivolumab + ipilimumab is specifically recommended for intermediate/poor risk patients.
Surgery in metastatic disease:
- Cytoreductive nephrectomy: less commonly used in the current era of effective systemic therapy
- Metastasectomy: may extend survival and can cure selected patients (best candidates: disease-free interval >1 year, solitary metastatic site, lung metastases)
Radiation therapy: used for palliation of bone metastases and multiple brain metastases; stereotactic radiosurgery (SRS) for limited brain mets.
Prognosis
- Localized disease (Stage I-II): 5-year survival >80-90%
- Stage III: ~50-60%
- Metastatic (Stage IV): historically <10% at 5 years, but improving significantly with immunotherapy combinations
- Clear cell has the worst metastatic potential (90% of all RCC metastases)
- Chromophobe and papillary have lower metastatic rates but still require careful follow-up
- Sarcomatoid differentiation in any subtype is a poor prognostic indicator
Key High-Yield Points
- VHL gene (3p25) is the molecular hallmark of clear cell RCC - loss leads to HIF accumulation --> VEGF overexpression --> angiogenesis
- Clear cell RCC is prone to renal vein invasion and IVC thrombosis
- RCC is one of the great mimics - causes fever of unknown origin, hypercalcemia, erythrocytosis, and Stauffer syndrome
- Classic triad (hematuria + flank pain + mass) is now uncommon (<5-10%); most are found incidentally
- RCC is resistant to chemotherapy and conventional radiation - surgery for localized disease, immunotherapy combinations for metastatic
- Oncocytoma (benign) cannot be reliably distinguished from RCC on imaging - most are surgically resected
- VHL disease: bilateral clear cell RCC in 40-60% of affected individuals; autosomal dominant, 3p25
Sources: Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine, 26th ed.; Campbell-Walsh-Wein Urology; National Kidney Foundation Primer on Kidney Diseases, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.