Classification of empyema for md exams 10 marks answer
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the information needed for a comprehensive 10-mark exam answer. Let me compile it:
Classification of Empyema
Definition
Empyema thoracis is a collection of pus (purulent fluid) within the pleural space. It most commonly occurs as a complication of pneumonia (parapneumonic empyema) but may also follow trauma, surgery, esophageal rupture, or haematogenous spread.
I. Pathological / Stage-Based Classification (Most Important for Exams)
This is the primary classification based on temporal evolution of the pleural infection. It was originally described by the American Thoracic Society and has three stages progressing over approximately 3 weeks.
Stage I - Exudative Phase (Week 1)
| Feature | Details |
|---|---|
| Fluid character | Thin, serous, free-flowing, sterile |
| Pleural fluid | Low WBC, normal glucose, normal pH (>7.2), LDH <1000 IU/L |
| Fibrin | Absent or minimal |
| Loculation | None - fluid flows freely |
| Lung | Expands fully on drainage |
| Treatment | Systemic antibiotics + simple chest tube drainage (pigtail catheter sufficient) |
- The pleural membrane is still intact
- Fluid is an exudate (meets Light's criteria) but not yet purulent
- Spontaneous resolution possible with antibiotics alone
Stage II - Fibrinopurulent Phase (Week 2)
| Feature | Details |
|---|---|
| Fluid character | Turbid, purulent, viscous |
| Pleural fluid | pH <7.2, glucose <60 mg/dL, LDH >1000 IU/L |
| Fibrin | Fibrinous exudative deposits on visceral pleural surface |
| Loculation | Present - multiple loculated collections form |
| Lung | Partially trapped by adhesions |
| Treatment | VATS / fibrinolytics (tPA + DNase) to break loculations; simple chest drain usually insufficient |
- Fibrin strands create loculations that prevent adequate single-drain drainage
- Intrapleural tPA (10 mg alteplase) + DNase (5 mg dornase alfa) can be instilled to lyse septations
- VATS offers direct lysis of adhesions, re-expansion of lung, and optimal chest tube placement
Stage III - Fibrous / Organising Phase (Week 3+)
| Feature | Details |
|---|---|
| Fluid character | Thick, gelatinous; may be semi-solid |
| Pleural fluid | Frank pus; pH very low |
| Fibrin | Thick fibrous rind (peel) encasing the lung |
| Loculation | Dense, fibrous - cannot be broken by fibrinolytics |
| Lung | "Trapped lung" - cannot re-expand; capillary ingrowth into peel |
| Treatment | Open thoracotomy + decortication (removal of fibrous peel) |
- Fibroblast ingrowth creates an inelastic cortex that prevents lung expansion
- Results in restrictive lung defect and persistent pleural space with risk of chronic empyema
- Decortication removes both visceral and parietal fibrous peels to allow full re-expansion
II. Classification by Aetiology
| Type | Cause |
|---|---|
| Parapneumonic | Most common (50-60%); complicates bacterial pneumonia |
| Post-traumatic | Penetrating chest injury, haemothorax becoming infected |
| Post-operative | After thoracic surgery, oesophagectomy; bronchopleural fistula |
| Oesophageal rupture | Boerhaave syndrome - chemical + bacterial contamination |
| Haematogenous | Septicaemia seeding the pleural space (rare) |
| Transdiaphragmatic | Extension from subphrenic / hepatic abscess |
| Tuberculous | Mycobacterium tuberculosis; endemic areas, immunocompromised |
| Fungal | Aspergillus, Candida (immunocompromised hosts) |
III. Classification by Microbiological Aetiology
| Category | Organisms |
|---|---|
| Community-acquired | Streptococcus pneumoniae, Streptococcus milleri group, anaerobes |
| Hospital-acquired | Staphylococcus aureus (MRSA), gram-negatives (Klebsiella, Pseudomonas, E. coli) |
| Anaerobic | Fusobacterium nucleatum, Prevotella spp., Bacteroides fragilis, Peptostreptococcus spp. - particularly in aspiration, dental infections |
| Mycobacterial | M. tuberculosis - milky fluid, lymphocyte-predominant |
| Fungal | Aspergillus, Candida spp. |
IV. Classification by Duration
| Type | Time course | Characteristics |
|---|---|---|
| Acute | <6 weeks | Stages I-II; amenable to drainage ± VATS |
| Chronic | >6 weeks | Stage III; thick peel; requires decortication |
V. Parapneumonic Effusion Classification (Light's Classification - Clinically Relevant)
Light's classification stratifies parapneumonic effusions to guide the need for drainage:
| Class | Description | Pleural Fluid Findings | Management |
|---|---|---|---|
| 1 | Insignificant PPE | <10 mm on decubitus CXR | Antibiotics only; no thoracentesis needed |
| 2 | Typical PPE | >10 mm; glucose >60; pH >7.2; Gram stain/culture negative | Antibiotics; monitor |
| 3 | Borderline complicated PPE | pH 7.0-7.2; LDH >1000; glucose 40-60 | Drainage + antibiotics |
| 4 | Simple complicated PPE | pH <7.0; glucose <40; culture/Gram stain positive; non-loculated | Drainage + antibiotics |
| 5 | Complex complicated PPE | pH <7.0; glucose <40; multiloculated | Drainage; often VATS |
| 6 | Simple empyema | Frank pus; single locule or free-flowing | Chest tube; VATS |
| 7 | Complex empyema | Frank pus; multiloculated | VATS / open drainage |
(Classes 1-2 = no drainage; Classes 3-7 = drainage required)
VI. Diagnosis - Key Pleural Fluid Parameters
| Parameter | Empyema | Simple PPE |
|---|---|---|
| Appearance | Turbid / frank pus | Serous/straw |
| pH | <7.1 (diagnostic) | >7.2 |
| Glucose | <30-40 mg/dL | >60 mg/dL |
| LDH | >1000 IU/L | <1000 IU/L |
| WBC | >20,000 cells/mm³ | Variable |
| Gram stain / culture | Often positive (but negative if pretreated) | Negative |
CT Appearances of the Three Stages
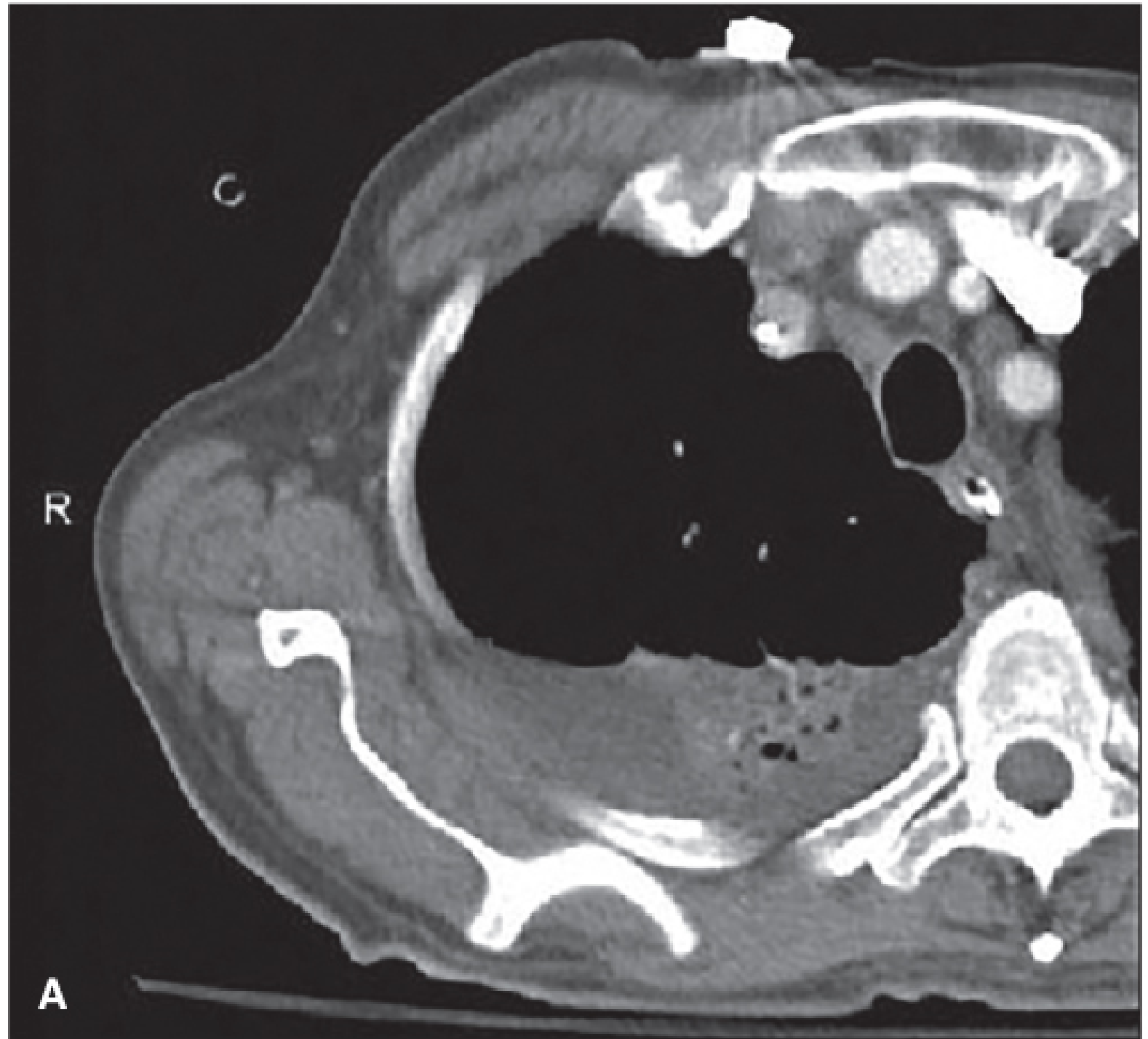
CT chest showing Stage I parapneumonic effusion - dependent, lenticular, free-flowing fluid with no loculation (Fischer's Mastery of Surgery)
- Stage I (CT): Dependent, lenticular fluid; no pleural thickening; no septations
- Stage II (CT): Loculated fluid; linear septations; mediastinal pleural fluid; "split pleura" sign (enhancing thickened visceral and parietal layers)
- Stage III (CT): Thick pleural rind; contracted hemithorax; fibrous cortex encasing the lung
Summary Table for Quick Revision
| Feature | Stage I (Exudative) | Stage II (Fibrinopurulent) | Stage III (Organising) |
|---|---|---|---|
| Duration | Week 1 | Week 2 | Week 3+ |
| Fluid | Thin, serous | Turbid, purulent | Thick pus/gelatinous |
| pH | >7.2 | <7.2 | Very low |
| Glucose | Normal | <60 | <40 |
| Loculation | None | Present | Dense/fibrous |
| Pleural peel | Absent | Fibrinous deposits | Thick fibrous rind |
| Treatment | Antibiotics + chest tube | VATS / fibrinolytics | Decortication |
Key exam points:
- The 3-stage classification (Exudative - Fibrinopurulent - Organising) is the most tested
- Each stage has a specific treatment: antibiotics alone → VATS/fibrinolytics → decortication
- Pleural fluid pH <7.1 is the single most important indicator for drainage
- "Trapped lung" is the hallmark of Stage III requiring decortication
- The "split pleura" sign on CT is characteristic of empyema (enhancing thickened visceral and parietal pleura separated by fluid)
Sources: Fishman's Pulmonary Diseases and Disorders; Fischer's Mastery of Surgery 8th ed.; Sabiston Textbook of Surgery; Schwartz's Principles of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.