Give details information about the splenomegaly from the modern surgery book
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from Schwartz's Principles of Surgery (11th Edition). Here is a detailed, well-organized answer:
Splenomegaly — Schwartz's Principles of Surgery, 11th Edition
1. Definition and Terminology
Splenomegaly refers simply to abnormal enlargement of the spleen. The surgical literature describes it variably as moderate, massive, and hyper, reflecting a lack of universal consensus. The most widely accepted criteria are:
- Splenomegaly: organ weighing ≥500 g and/or averaging ≥15 cm in pole-to-pole length
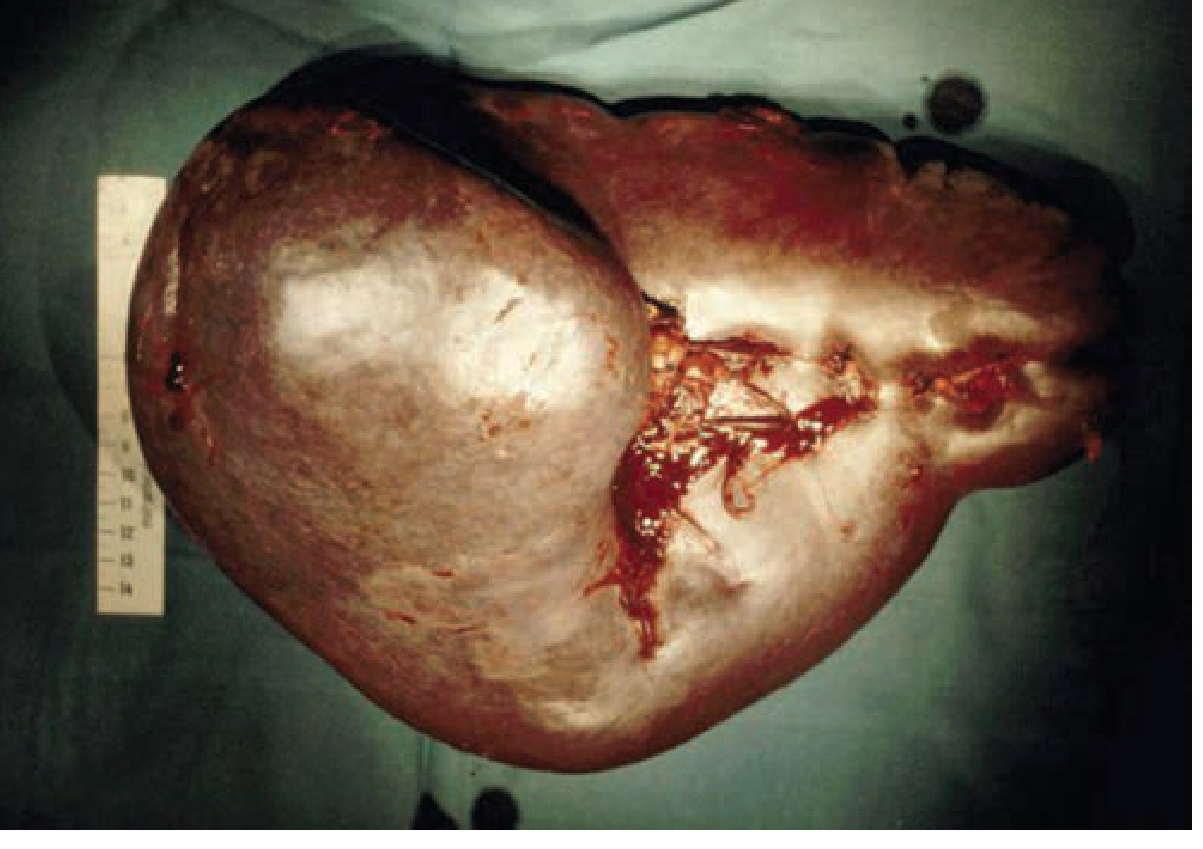
- Massive splenomegaly: spleen >1 kg in mass or >22 cm in length (Figure 34-4)
- Spleens palpable below the left costal margin are estimated to weigh at least ≥750 g and to be at least double normal size
Critical distinction: Splenomegaly ≠ Hypersplenism. Hypersplenism is defined as one or more cytopenias in the context of a normally functioning bone marrow, and while it often accompanies splenomegaly, the two are not synonymous.
2. Pathophysiology
How Splenomegaly Develops
In patients with chronic hemolytic disorders, the reticular spaces of the red pulp become distended with macrophages engorged with the products of erythrocyte breakdown, leading to permanent hypertrophy.
Consequences on Blood Cells
| Cell Type | Normal Kinetics | Effect of Splenomegaly |
|---|---|---|
| Platelets | 10-day lifespan; 1/3 of pool normally sequestered | Up to 80% of platelet pool sequestered → thrombocytopenia |
| Neutrophils | ~6-hour half-life in circulation | Sequestration or removal → neutropenia |
| Red blood cells | Filtered continuously | Accelerated destruction → anemia |
Hypersplenism disorders can be categorized as:
- (a) Increased destruction of abnormal blood cells in an intrinsically normal spleen (e.g., hemolytic anemias)
- (b) Primary disorders of the spleen causing sequestration/destruction of normal blood cells (e.g., infiltrative disorders)
3. Causes of Splenomegaly
A. Red Blood Cell Disorders (Benign)
Autoimmune Hemolytic Anemia (AIHA)
- One-third to one-half of patients with warm-antibody AIHA present with splenomegaly, sometimes palpable on exam
- Diagnosis: hemolysis markers (anemia, reticulocytosis, elevated bilirubin) + positive direct Coombs' test
- Treatment: corticosteroids (mainstay) → rituximab → splenectomy (3rd-line, effective in ~75–85%)
Sickle Cell Disease
- Sequestration occurs in the spleen → splenomegaly early in the disease course
- Subsequent infarction leads to autosplenectomy in most patients
- Indications for splenectomy: recurrent acute sequestration crises, hypersplenism, splenic abscess
B. Platelet Disorders (Benign)
Idiopathic Thrombocytopenic Purpura (ITP)
- Splenomegaly is uncommon in ITP — its presence should prompt a search for another cause of thrombocytopenia
- Up to 10% of children may have a palpable spleen tip
C. Myeloproliferative Disorders (Malignant)
The common underlying problem leading to splenectomy in all myeloproliferative disorders is symptomatic splenomegaly. Symptoms from mass effect include:
- Early satiety
- Poor gastric emptying
- Heaviness or pain in the left upper quadrant
- Even diarrhea
| Disorder | Splenomegaly Feature | Splenectomy Indication |
|---|---|---|
| CML | Found in ~50% of patients; LUQ pain, early satiety | Symptom relief from massive splenomegaly |
| AML | Can occur | Intolerable symptomatic splenomegaly |
| Myelofibrosis | Prominent feature | Symptomatic relief |
| Polycythemia vera | Common | Symptomatic splenomegaly |
D. Lymphomas and Leukemias
Hairy Cell Leukemia (HCL)
- Classic triad: splenomegaly, pancytopenia, abnormal hairy lymphocytes on peripheral smear
- Splenectomy was historically the mainstay but is now rarely performed due to effective drugs (rituximab, cladribine, pentostatin)
Chronic Lymphocytic Leukemia (CLL)
- Enlarged spleen may be massive or barely palpable; splenectomy 75% effective for cytopenias
Hodgkin's Lymphoma (HL)
- Massive splenomegaly is not common; large spleens do not necessarily signify splenic involvement
- Staging laparotomy largely replaced by CT and PET imaging
Non-Hodgkin's Lymphoma (NHL)
- Splenomegaly exists in some but not all forms; splenectomy does not alter natural history but is indicated in certain cases
E. Storage and Infiltrative Diseases
| Disease | Mechanism | Splenomegaly Features |
|---|---|---|
| Gaucher's disease | Glucocerebroside deposition (lysosomal hydrolase deficiency) | Organomegaly, early satiety, hypersplenism |
| Niemann-Pick disease | Sphingomyelin/cholesterol storage (Types A & B most affected) | Splenomegaly with concomitant symptoms |
| Amyloidosis | Abnormal extracellular protein deposition | Splenic involvement in ~5% (primary); secondary form may cause splenomegaly + rupture |
| Sarcoidosis | Noncaseating granulomas | Splenomegaly in ~25%; massive splenomegaly (>1 kg) in ~3%; spontaneous rupture reported |
F. Portal Hypertension & Vascular Causes
Portal Hypertension (usually from cirrhosis)
- Splenomegaly and splenic congestion are common; lead to sequestration and destruction of blood cells
- Splenectomy is not indicated for hypersplenism per se — no correlation between pancytopenia and long-term survival
- Exception: splenic vein thrombosis (sinistral hypertension) → potentially curable with splenectomy
Idiopathic Portal Hypertension (IPH)
- Triad: splenomegaly + pancytopenia + normocellular bone marrow → may require splenic artery embolization or splenectomy
G. Autoimmune/Connective Tissue
Felty's Syndrome
- Classic triad: rheumatoid arthritis + splenomegaly + neutropenia
- Occurs in ~3% of patients with rheumatoid arthritis (two-thirds are women)
4. Postoperative Specimen — Enlarged Spleen
5. Surgical Management: Splenectomy for Splenomegaly
General Indications
Splenectomy is performed for:
- Cure or palliation of hematological disease (hypersplenism)
- Symptom relief from mass effect of splenomegaly (early satiety, LUQ pain)
- Control of infection or hemorrhage
- Diagnosis of splenic pathology
Symptoms from Mass Effect (Requiring Intervention)
- Early satiety
- Poor gastric emptying
- Left upper quadrant heaviness or pain
- Diarrhea
- Radiation therapy has been used since 1903 for myeloproliferative-related splenomegaly when surgery is not an option
Laparoscopic vs. Open Approach
- Laparoscopic splenectomy is generally preferred
- However, the benefits may not apply for patients with splenomegaly — a 2019 matched case study found that for patients with moderate splenomegaly, the approach requires more careful patient selection
Summary Table: Causes of Splenomegaly by Category
| Category | Key Conditions |
|---|---|
| Hemolytic anemias | AIHA, sickle cell disease, thalassemia |
| Myeloproliferative | CML, AML, myelofibrosis, polycythemia vera |
| Lymphoma/leukemia | HCL, CLL, NHL, HL |
| Storage diseases | Gaucher's, Niemann-Pick, amyloidosis, sarcoidosis |
| Portal hypertension | Liver cirrhosis, splenic vein thrombosis |
| Autoimmune | Felty's syndrome, AIHA secondary to SLE |
| Infectious | (Not detailed in surgery text — more in medicine texts) |
Source: Schwartz's Principles of Surgery, 2-Volume Set, 11th Edition — Chapter 34: The Spleen (pp. 1548–1559)
This is a shared conversation. Sign in to Orris to start your own chat.