Hyperthyroidism and hypothyroidism treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
hyperthyroidism treatment guidelines
Searching PubMed
hypothyroidism levothyroxine treatment
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to provide a detailed, well-structured answer. Let me compile it.
Hyperthyroidism and Hypothyroidism: Treatment
HYPOTHYROIDISM
First-Line Treatment: Levothyroxine (T4)
Levothyroxine (LT4) is the treatment of choice for hypothyroidism. It is preferred over T3 (liothyronine) or T3/T4 combination products (liotrix) because:
- Better tolerated
- Longer half-life (~7 days)
- Once-daily dosing
- Steady state achieved in 6-8 weeks
The American Thyroid Association (ATA) does not recommend routine combination therapy (LT4 + liothyronine), as evidence of superiority over monotherapy is inconsistent. However, a 2026 meta-analysis (PMID: 40579157) found that liothyronine-containing regimens were associated with reduced risk of dementia and mortality - this emerging evidence may influence future guidelines.
Dosing
| Population | Typical Dose |
|---|---|
| Standard adults | ~1.8 mcg/kg/day |
| Elderly (>65) | ~0.5 mcg/kg/day |
| Ischemic heart disease | Start low, titrate slowly |
| Infants/young children | Higher doses (per kg) |
- Start at the lower end of the expected optimal dose
- Exception: in longstanding disease or ischemic heart disease, always start low and titrate up
Timing of Administration
- Take 30-60 minutes before breakfast (food and caffeine impair absorption)
- Bedtime administration is equally effective and may improve compliance
Monitoring Goals
- Primary hypothyroidism: target TSH within reference interval
- Central hypothyroidism: target free T4 toward the upper end of reference interval
- Check TSH no earlier than 4-6 weeks after dose change
- Repeat at 4-6 months, then annually once stable
Subclinical Hypothyroidism (SCH)
- TSH >10 mIU/L: treat with LT4 (especially in patients <65-70 years)
- TSH <10 mIU/L with symptoms: consider LT4; stop if symptoms don't improve
- Age >80-85 years with TSH ≤10: wait-and-see approach recommended
Drug Interactions (reduce LT4 efficacy)
| Category | Examples |
|---|---|
| CYP450 inducers | Phenytoin, rifampin, phenobarbital |
| Absorption reducers | Iron, calcium carbonate, cholestyramine, sucralfate |
| Dietary inhibitors | Coffee, fiber, soy, grapes, papaya |
Toxicity Signs (excess dosing = mimics hyperthyroidism)
Nervousness, palpitations, tachycardia, heat intolerance, weight loss
Special caution: In central hypothyroidism, always exclude concomitant adrenal insufficiency before starting LT4 - precipitating an adrenal crisis is a real risk.
Sources: Tietz Textbook of Laboratory Medicine, 7th Ed.; Lippincott Illustrated Reviews: Pharmacology
HYPERTHYROIDISM
Three Main Treatment Strategies
| Approach | Methods |
|---|---|
| Ablation of gland | Radioactive iodine (RAI / ¹³¹I), surgery |
| Inhibit hormone synthesis | Thioamides (methimazole, PTU) |
| Block hormone release | Iodide (short-term), beta-blockers |
1. Radioactive Iodine (RAI / ¹³¹I)
- Selectively taken up by thyroid follicular cells and destroys them
- Most patients develop hypothyroidism afterward and require LT4 long-term
- Preferred for:
- Older adults (>65) with persistent Graves disease + comorbidities
- Toxic multinodular goiter (TMNG) or autonomously functioning solitary nodule
- Patients where definitive therapy is needed to prevent cardiac progression
2. Thioamides - Methimazole and PTU
Both drugs inhibit:
- Iodination of tyrosyl groups (oxidative process)
- Coupling of iodotyrosines to form T3 and T4
PTU additionally blocks peripheral conversion of T4 → T3.
Important: Neither drug affects pre-formed thyroglobulin already stored in the gland. Clinical effects are delayed until stores are depleted (weeks).
| Feature | Methimazole | PTU |
|---|---|---|
| Dosing frequency | Once daily (longer half-life) | Multiple times daily |
| Preferred agent | Yes (first-line) | Second-line |
| Agranulocytosis risk | Yes (both agents) | Yes (both agents) |
| Hepatotoxicity | Mild-moderate | Severe (potentially fatal liver failure) |
| Use in pregnancy | Avoid 1st trimester | Preferred in 1st trimester |
| Mechanism | Synthesis inhibition | Synthesis + peripheral T4→T3 block |
Adverse effects: Rash, pruritus, arthralgia, agranulocytosis, hepatotoxicity
3. Iodide (Short-term use only)
- Inhibits iodination ("Wolff-Chaikoff effect") - lasts only a few days
- Inhibits release of thyroid hormones from thyroglobulin
- Uses: Thyroid storm, pre-operative preparation (reduces vascularity)
- Not for long-term use
- Adverse effects: Sore mouth/throat, tongue swelling, metallic taste, mucosal ulcerations
4. Beta-Blockers (Symptom control)
Propranolol, metoprolol, atenolol - blunt the widespread sympathetic stimulation.
- Reduce palpitations, tremor, anxiety, tachycardia
- Do NOT reduce thyroid hormone levels
- Also used in thyroid storm
Treatment Selection by Etiology (Braunwald's Algorithm)
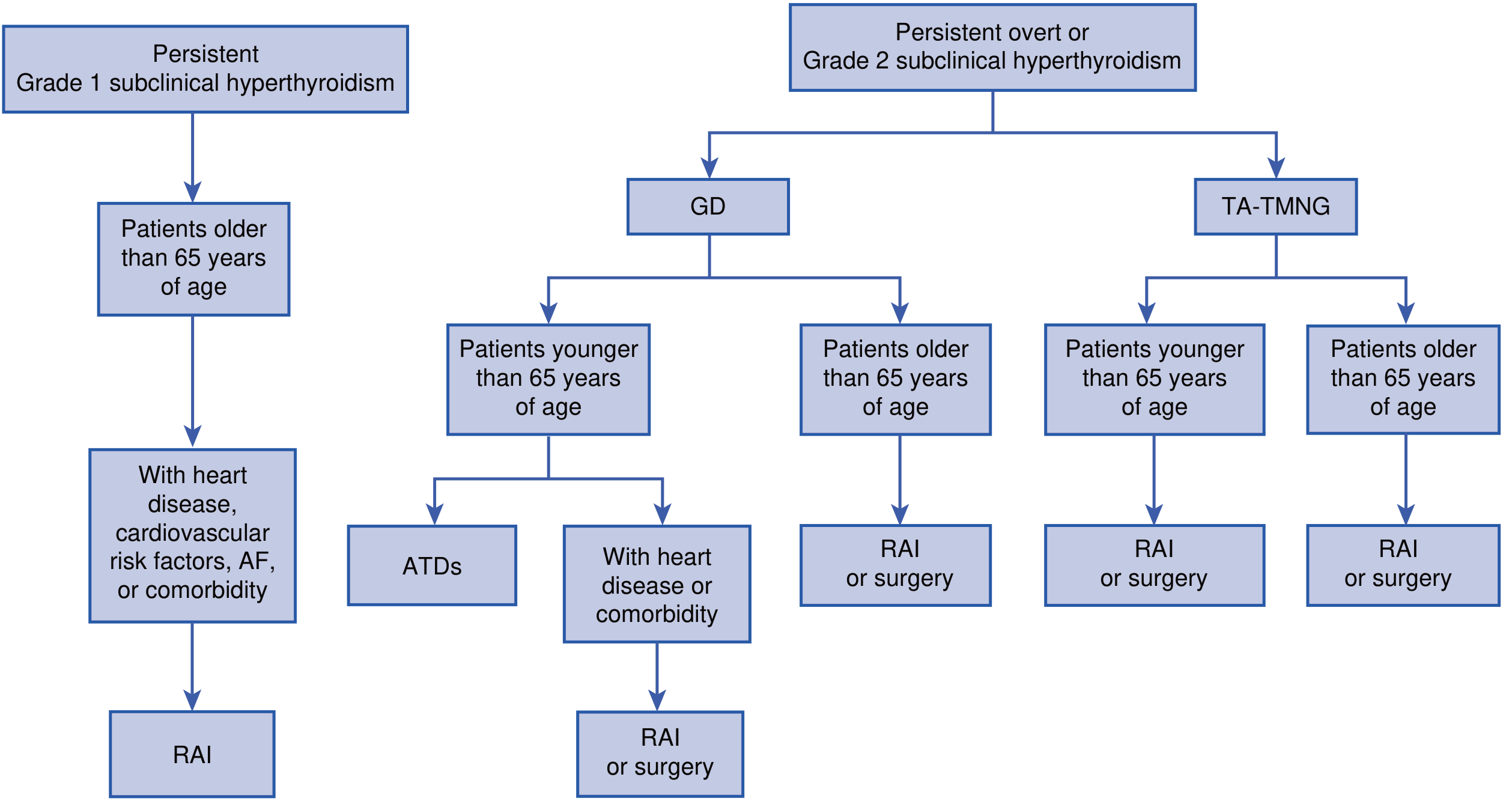
Figure: Treatment decision flowchart for hyperthyroidism - GD = Graves Disease, TA-TMNG = Toxic Adenoma/Toxic Multinodular Goiter, ATDs = Antithyroid Drugs, RAI = Radioactive Iodine. (Braunwald's Heart Disease)
Key decision points:
- Graves disease, patient <65, no comorbidities: Antithyroid drugs (methimazole) - may remit spontaneously
- Graves disease, patient >65 or with heart disease: RAI or surgery (definitive therapy)
- TMNG or solitary toxic nodule, any age: RAI or surgery
- Grade 1 subclinical hyperthyroidism (TSH 0.1-0.4), asymptomatic young/premenopausal: No treatment needed (insufficient evidence of harm)
Thyroid Storm (Hyperthyroid Emergency)
Thyroid storm is the most severe form of hyperthyroidism. Mortality can reach 50%.
Clinical features: Altered mental status, high fever, GI symptoms, extreme tachycardia, new atrial fibrillation, hypotension, cardiovascular collapse.
Treatment (same drugs as for hyperthyroidism, but higher doses, more frequent):
- High-dose thioamides (PTU preferred - also blocks T4→T3 conversion)
- Potassium iodide (given AFTER thioamides to avoid iodine fueling synthesis)
- Beta-blockers (IV esmolol with caution; avoid if heart failure or hypotension)
- ICU monitoring
- Treat precipitating cause (infection, trauma, amiodarone)
Summary Comparison
| Feature | Hypothyroidism Tx | Hyperthyroidism Tx |
|---|---|---|
| First-line drug | Levothyroxine (T4) | Methimazole |
| Monitoring | TSH (every 4-6 weeks until stable) | TSH (low = response) |
| Definitive cure | Lifelong LT4 replacement | RAI or thyroidectomy |
| Pregnancy | Continue LT4 (increase dose) | PTU in 1st trimester |
| Emergency | Myxedema coma: IV T4 ± T3 | Thyroid storm: PTU + iodide + beta-blocker + ICU |
Recent evidence note (PubMed, 2025-2026):
- A 2026 network meta-analysis (PMID: 39290156) found patients prefer combination LT4+T3 over LT4 alone, despite current ATA guidelines favoring monotherapy - watch for guideline updates.
- A 2026 meta-analysis (PMID: 40579157) suggests liothyronine-containing regimens reduce dementia risk and mortality compared to LT4 alone, which may support a role for combination therapy in select patients.
Sources: Lippincott Illustrated Reviews: Pharmacology; Braunwald's Heart Disease, 2-Vol Set; Tietz Textbook of Laboratory Medicine, 7th Ed.
Create a clinical reference guide comparing hyperthyroid treatment options
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.