Transthoracic pressure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Here is a thorough explanation of transthoracic pressure drawn from authoritative pulmonary and anesthesia textbooks.
Transthoracic Pressure
Definition and Formula
Transthoracic pressure (P_TT) is the pressure difference between the alveoli (or mouth, under static no-flow conditions) and the body surface:
P_TT = P_A - P_bs (Alveolar pressure minus body-surface/atmospheric pressure)
It represents the total distending pressure applied to the entire respiratory system - lungs plus chest wall together - when the respiratory muscles are completely relaxed.
- Fishman's Pulmonary Diseases and Disorders (Appendix, p. 2701) defines it precisely as P_A - P_bs, distinguishing it from:
- Transpulmonary pressure (P_A - P_pl) - distending pressure across the lung alone
- Pressure across the chest wall (P_pl - P_bs) - distending pressure across the chest wall alone
The relationship between the three pressures is:
P_A - P_bs = (P_A - P_pl) + (P_pl - P_bs) Transthoracic = Transpulmonary + Chest wall pressure
From Morgan and Mikhail's Clinical Anesthesiology (7e):
"Transthoracic pressure equals atmospheric pressure minus intrapleural pressure." (This is the chest wall component, P_pl - P_bs, which is the distending pressure for the chest wall in isolation.)
Role in Respiratory Mechanics
Chest Wall Compliance
Chest wall compliance (C_W) is defined as:
$$C_W = \frac{\Delta \text{Volume}}{\Delta \text{Transthoracic pressure}}$$
Normal C_W is approximately 200 mL/cmH₂O. Total respiratory compliance combines lung and chest wall in series:
$$\frac{1}{C_{total}} = \frac{1}{C_W} + \frac{1}{C_L}$$
Since C_W ≈ C_L ≈ 200 mL/cmH₂O, total compliance ≈ 100 mL/cmH₂O.
Measurement of Total Respiratory System Elasticity
The elasticity of the respiratory system as a whole is determined by measuring how volume changes in response to changes in transthoracic pressure while the muscles are fully relaxed (relaxation technique or continuous positive pressure technique). At each point of zero airflow, mouth pressure equals alveolar pressure, so transthoracic pressure is directly measurable.
Transthoracic Pressure at Key Lung Volumes
The figure below from Fishman's shows the pressure-volume curves for the lung alone (blue dashed), chest wall alone (green dotted), and both together (red solid):
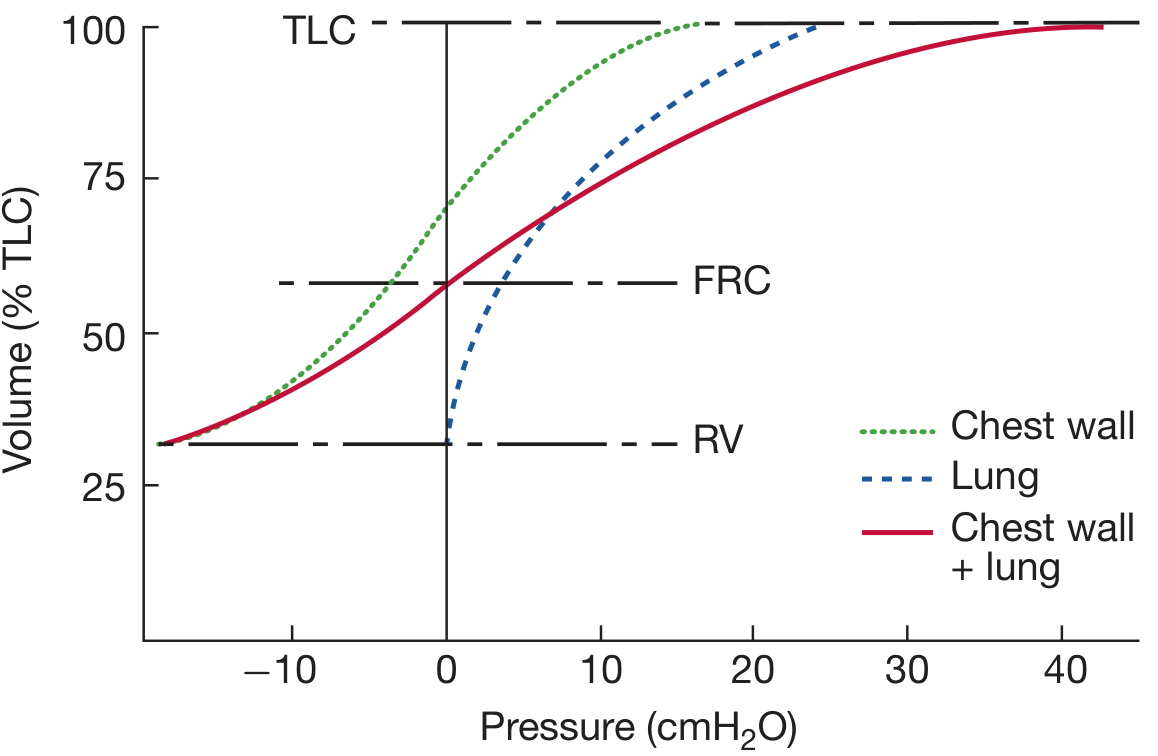
Key observations:
| Lung Volume | Transthoracic Pressure | Meaning |
|---|---|---|
| FRC (functional residual capacity, ~60% TLC) | 0 cmH₂O | Chest wall outward recoil exactly balances lung inward recoil; system is at rest |
| TLC (total lung capacity) | High positive | Both lung and chest wall recoil inward; large pressure needed to hold lungs open |
| RV (residual volume) | Negative (chest wall recoil outward, lung contribution minimal) | Chest wall springs outward; lung recoil is minimal at low volumes |
| ~70% TLC | Chest wall recoil = 0 | Below this volume the chest wall springs outward; above this it springs inward |
At FRC specifically:
"The outwardly directed recoil of the chest wall balances the inwardly directed recoil of the lung, and the transthoracic pressure is zero (i.e., P_A - P_bs = 0). The system 'comes to rest' at FRC because of the counterbalancing of these forces at that volume." - Fishman's Pulmonary Diseases and Disorders, p. 582
Assessment Method
The chest wall pressure across it (P_pl - P_bs) for any given lung volume is calculated as:
P_pl - P_bs = (P_A - P_bs) - (P_A - P_pl) = Transthoracic pressure - Transpulmonary pressure
Pleural pressure (P_pl) is estimated clinically using an esophageal balloon catheter (esophageal pressure, P_es ≈ P_pl).
Clinical Relevance
-
Airway obstruction - Narrowed airways require a greater transthoracic pressure gradient for inspiratory airflow; this increases the resistive work of breathing.
-
Diving / immersion - Breathing through a snorkel at depth is limited by the ability of the inspiratory muscles to breathe against the transthoracic pressure imposed by the surrounding water pressure (hydrostatic pressure difference between water surface and the lung).
-
Mechanical ventilation - Understanding transthoracic pressure helps distinguish ventilator-applied pressure from the pressure that actually distends the lungs (transpulmonary) vs. the chest wall.
-
Supine position - Chest wall compliance falls in the supine position because abdominal contents push against the diaphragm, altering the transthoracic pressure needed for a given volume change.
Sources:
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set, pp. 581-582, 2701 (Sections: Static Compliance of the Chest Wall; Elastic Properties of the Respiratory System as a Whole; Appendices)
- Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 922 (Section: Compliance)
Transpulmonary pressure between inspiration and expiration
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Here is a complete, textbook-grounded explanation of how transpulmonary pressure changes between inspiration and expiration.
Transpulmonary Pressure: Inspiration vs. Expiration
Definition
Transpulmonary pressure (P_L) is the pressure difference across the lung wall:
P_L = P_alveolar - P_pleural
It represents the elastic distending force on the lung at any moment, and is also called the recoil pressure - the force the lung exerts trying to collapse inward.
Pressure Values at Each Phase of the Breathing Cycle
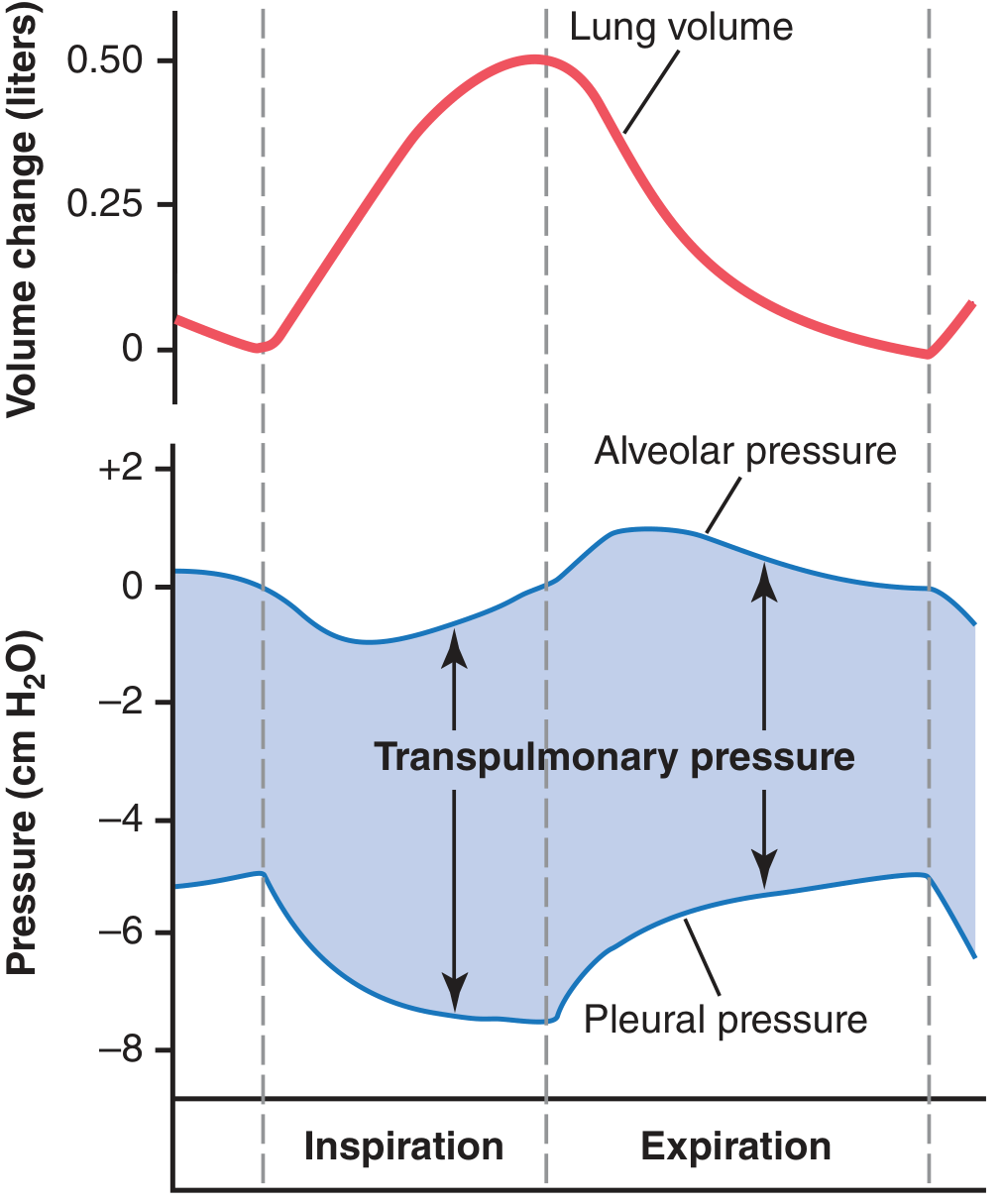
The diagram below from Guyton and Hall Medical Physiology shows exactly how lung volume, alveolar pressure, pleural pressure, and transpulmonary pressure all change across a breath:
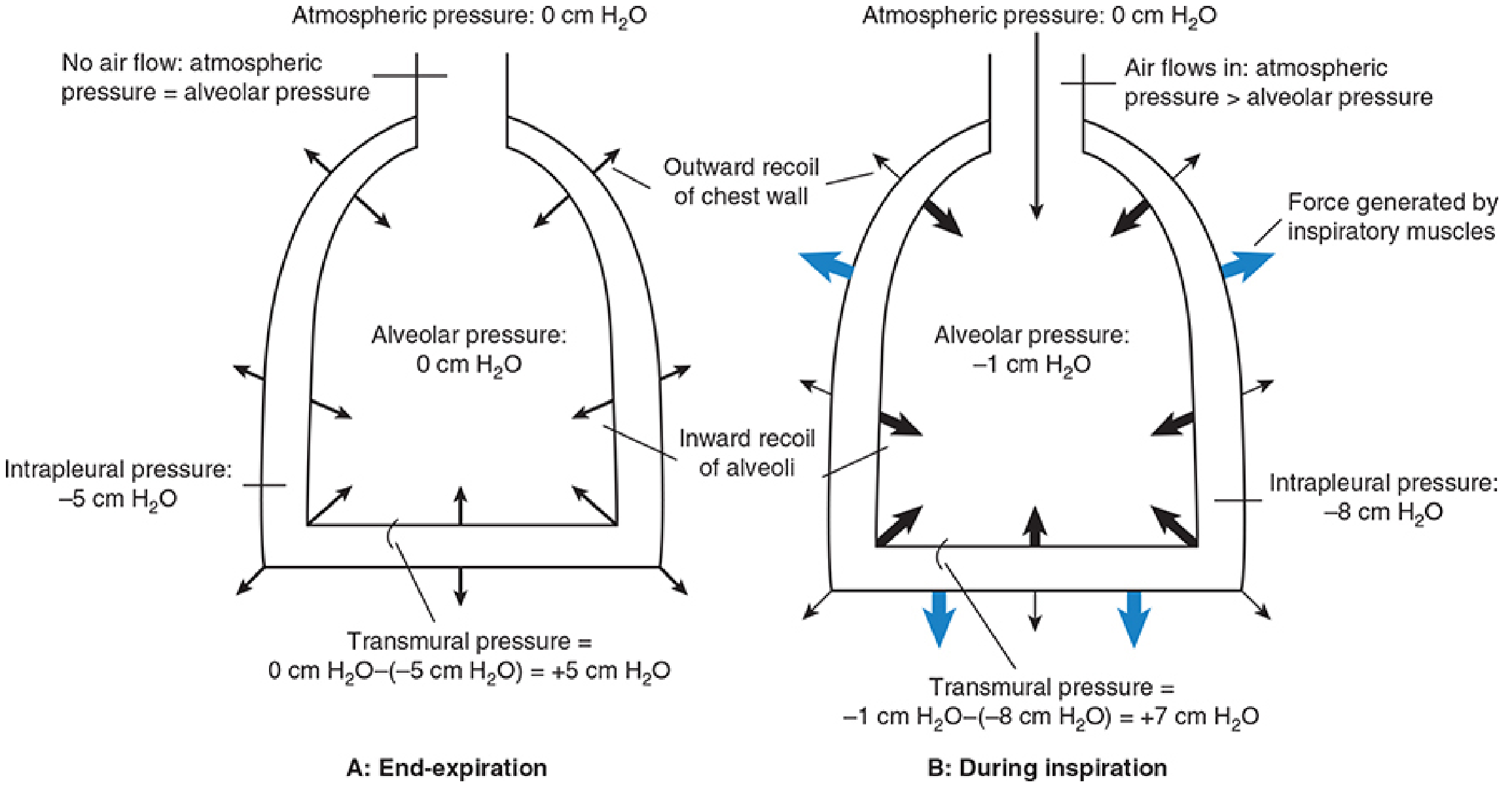
And below, the interaction of lung and chest wall at end-expiration (A) and during inspiration (B), showing exact pressure values - from Morgan and Mikhail's Clinical Anesthesiology:
| Phase | P_alveolar | P_pleural | P_L (transpulmonary) |
|---|---|---|---|
| End-expiration (FRC, at rest) | 0 cmH₂O | -5 cmH₂O | +5 cmH₂O |
| During inspiration (mid-breath) | -1 cmH₂O | -7.5 to -8 cmH₂O | ~+7 cmH₂O |
| End-inspiration | 0 cmH₂O (flow = 0) | -7.5 cmH₂O | +7.5 cmH₂O |
| During expiration | +1 cmH₂O | -5 to -7 cmH₂O | ~+6 to +5 cmH₂O |
| End-expiration (next cycle) | 0 cmH₂O | -5 cmH₂O | +5 cmH₂O |
Step-by-Step Mechanism
Inspiration
- Diaphragm and intercostal muscles contract, pulling the chest wall outward.
- Pleural pressure falls from -5 cmH₂O to about -7.5 to -8 cmH₂O (more negative).
- This more negative pleural pressure is transmitted to the alveoli, pulling the lung outward and dropping alveolar pressure to about -1 cmH₂O (below atmospheric).
- The alveolar-to-mouth pressure gradient (-1 vs. 0) drives air inward.
- Lung volume increases by ~0.5 L (normal tidal volume).
- P_L = (-1) - (-8) = +7 cmH₂O - larger than at rest, so the lung is more distended and holds more recoil energy.
"Diaphragmatic and intercostal muscle activation during inspiration expands the chest and decreases intrapleural pressure from -5 cmH₂O to -8 or -9 cmH₂O. As a result, alveolar pressure also decreases, and an alveolar-upper airway gradient is established; gas flows from the upper airway into alveoli."
- Morgan and Mikhail's Clinical Anesthesiology (7e), p. 919
At End-Inspiration (No Flow)
When flow stops at peak inspiration, alveolar pressure returns to 0. Pleural pressure is still -7.5 cmH₂O. So:
P_L = 0 - (-7.5) = +7.5 cmH₂O
This represents stored elastic energy - maximum recoil pressure of the lung at that volume.
"At end-inspiration, the lungs contain more air, and the distending pressure, which also represents the recoil pressure, is greater."
- Fishman's Pulmonary Diseases and Disorders, p. (Chapter 10)
Expiration
- Inspiratory muscles relax - pleural pressure returns toward -5 cmH₂O.
- The stored elastic recoil of the lung causes alveolar pressure to rise to about +1 cmH₂O (above atmospheric).
- The alveolar-to-mouth gradient (+1 vs. 0) drives air outward.
- Lung volume returns to FRC.
- Normal quiet expiration is entirely passive - driven by stored elastic recoil, no muscular effort required.
- P_L decreases back to +5 cmH₂O.
"Diaphragmatic relaxation returns intrapleural pressure to -5 cmH₂O during expiration in normal breathing. Now the transpulmonary pressure does not support the new lung volume, and the elastic recoil of the lung causes a reversal of the previous alveolar-upper airway gradient."
- Morgan and Mikhail's Clinical Anesthesiology (7e), p. 920
Hysteresis: Inspiratory vs. Expiratory Compliance Curves
Transpulmonary pressure is not the same during inspiration and expiration at the same lung volume - a phenomenon called hysteresis. For a given lung volume, less transpulmonary pressure is needed during expiration than during inspiration. The compliance diagram of the lung forms a loop, not a single line:
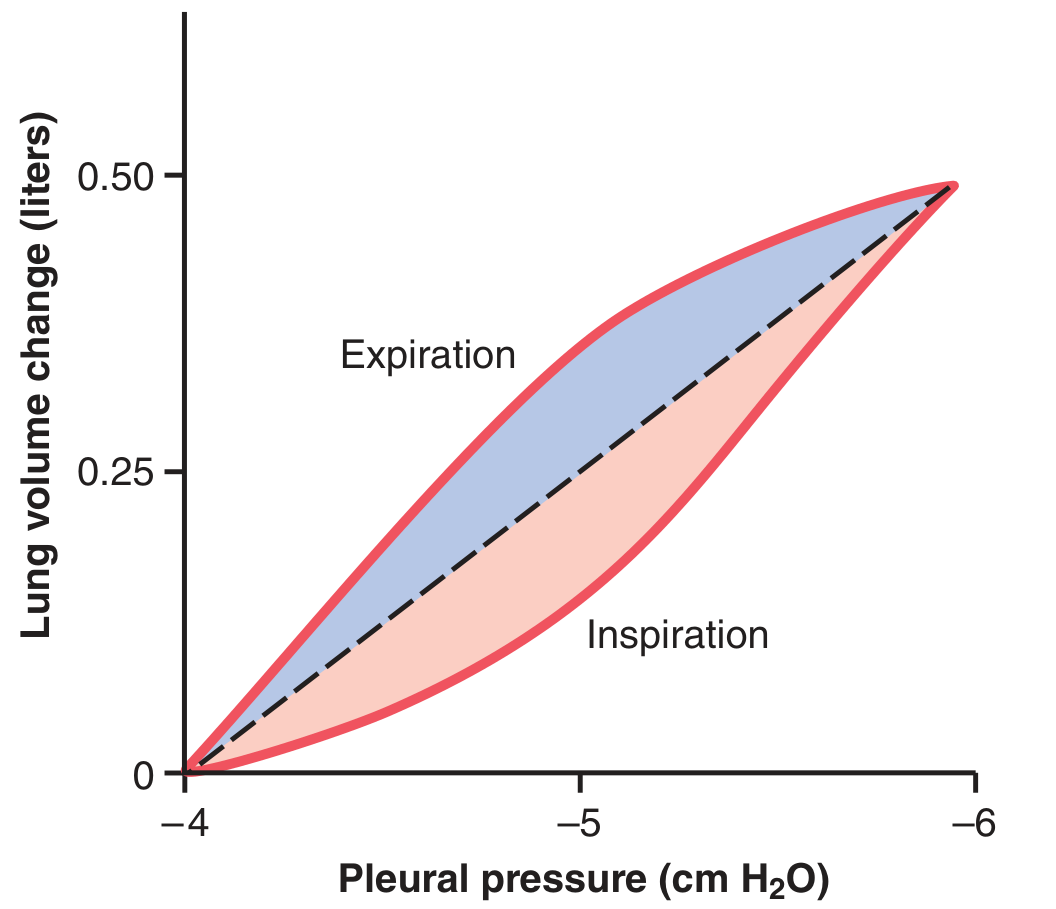
This loop arises because:
- Surface tension in alveoli is higher during inflation (air-fluid interface stretching) and lower during deflation (surfactant concentrating as alveoli shrink).
- Tissue viscoelastic resistance - energy is dissipated during expansion.
- Surfactant (~2/3 of total lung elasticity) acts differently during inflation vs. deflation.
Key Concept: P_L as Recoil Pressure
P_L is simultaneously:
- The distending pressure - what keeps the lung open against its tendency to collapse.
- The elastic recoil pressure - the force the lung exerts trying to collapse inward at that volume.
At any lung volume, P_L = lung's elastic recoil pressure. The larger the lung volume, the greater the recoil, and therefore the greater P_L must be to hold it open.
Summary Table
| Parameter | End-Expiration | During Inspiration | End-Inspiration |
|---|---|---|---|
| P_alveolar | 0 | -1 cmH₂O | 0 |
| P_pleural | -5 cmH₂O | -7.5 to -8 | -7.5 cmH₂O |
| P_transpulmonary | +5 cmH₂O | ~+7 cmH₂O | +7.5 cmH₂O |
| Airflow | None | Into lungs | None |
| Muscle activity | Relaxed | Active (diaphragm) | Relaxed/transitioning |
Sources:
- Guyton and Hall Textbook of Medical Physiology, pp. 493-494 (Figs. 38.2, 38.3)
- Morgan and Mikhail's Clinical Anesthesiology, 7e, pp. 918-920
- Fishman's Pulmonary Diseases and Disorders, Chapter 10
This is a shared conversation. Sign in to Orris to start your own chat.