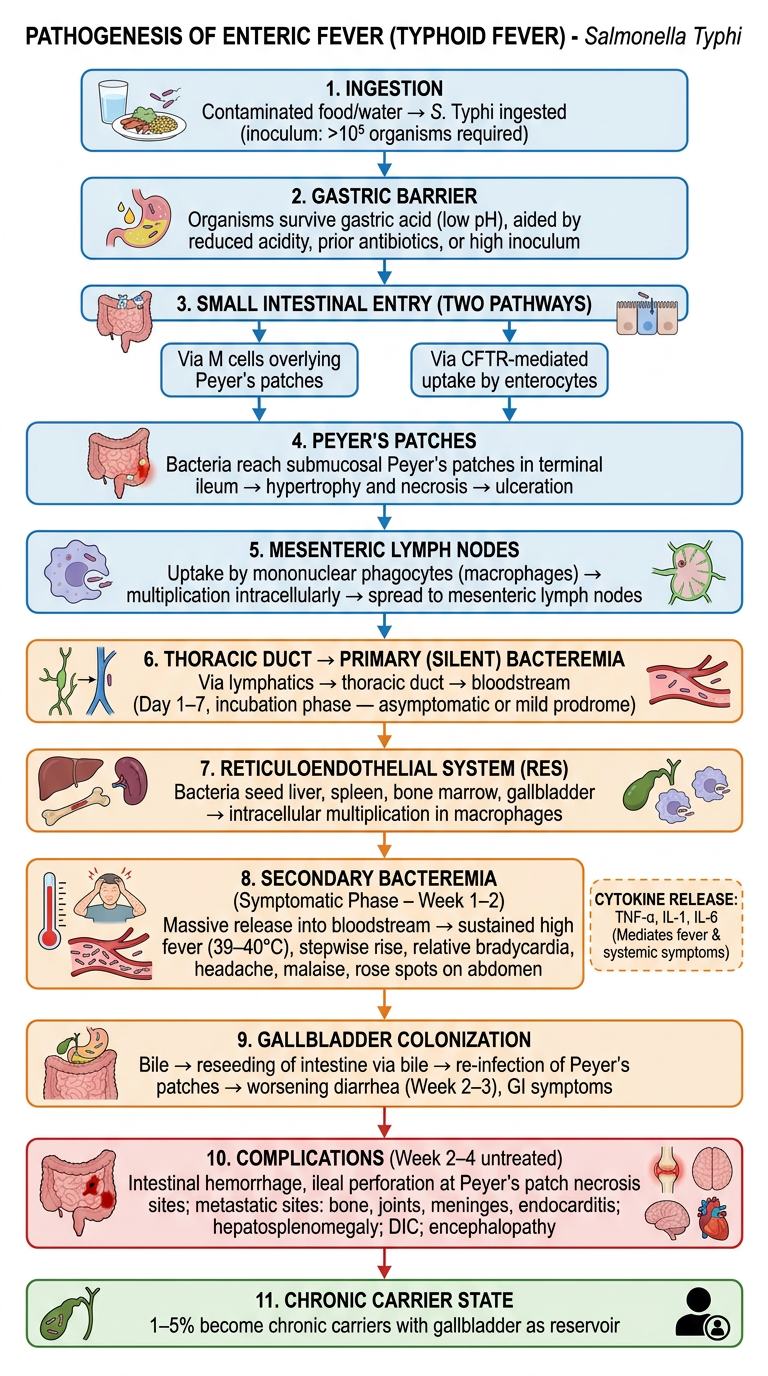
Pathogenesis of enteric fever from apurba sastry microbiology textbook in flow chart form
A detailed medical flowchart showing the pathogenesis of enteric fever (typhoid fever) caused by Salmonella Typhi. The flowchart should be vertical, clean, academic style with labeled boxes and arrows. Include these sequential steps with labels: 1. INGESTION: Contaminated food/water → S. Typhi ingested (inoculum: >10^5 organisms required) 2. GASTRIC BARRIER: Organisms survive gastric acid (low pH), aided by reduced acidity, prior antibiotics, or high inoculum 3. SMALL INTESTINAL ENTRY (TWO PATHWAYS): Via M cells overlying Peyer's patches OR via CFTR-mediated uptake by enterocytes 4. PEYER'S PATCHES: Bacteria reach submucosal Peyer's patches in terminal ileum → hypertrophy and necrosis → ulceration 5. MESENTERIC LYMPH NODES: Uptake by mononuclear phagocytes (macrophages) → multiplication intracellularly → spread to mesenteric lymph nodes 6. THORACIC DUCT → PRIMARY (SILENT) BACTEREMIA: Via lymphatics → thoracic duct → bloodstream (Day 1–7, incubation phase — asymptomatic or mild prodrome) 7. RETICULOENDOTHELIAL SYSTEM (RES): Bacteria seed liver, spleen, bone marrow, gallbladder → intracellular multiplication in macrophages 8. SECONDARY BACTEREMIA (Symptomatic Phase – Week 1–2): Massive release into bloodstream → sustained high fever (39–40°C), stepwise rise, relative bradycardia, headache, malaise, rose spots on abdomen 9. GALLBLADDER COLONIZATION: Bile → reseeding of intestine via bile → re-infection of Peyer's patches → worsening diarrhea (Week 2–3), GI symptoms 10. COMPLICATIONS (Week 2–4 untreated): Intestinal hemorrhage, ileal perforation at Peyer's patch necrosis sites; metastatic sites: bone, joints, meninges, endocarditis; hepatosplenomegaly; DIC; encephalopathy 11. CHRONIC CARRIER STATE: 1–5% become chronic carriers with gallbladder as reservoir Include cytokine release (TNF-α, IL-1, IL-6) as a side note near the secondary bacteremia step. Use color coding: blue for entry/ingestion, orange for bacteremia phases, red for complications, green for chronic carrier. Add small icons for bacteria, macrophage, liver/spleen, intestine. Clean white background, professional medical textbook style.
Pathogenesis of Enteric Fever - Step by Step
1. Ingestion
- Contaminated food or water ingested
- Infective dose: typically >10^5 organisms (lower if gastric acidity is reduced)
- S. Typhi is the main agent; S. Paratyphi A, B, C cause milder disease
2. Gastric Acid Barrier
- Most organisms are killed by gastric acid (pH <2)
- Surviving organisms proceed to the small intestine
- Risk increases with: achlorhydria, antacid/PPI use, prior antibiotics (which reduce competing flora), large inoculum
3. Intestinal Penetration (Two Pathways)
- Via M cells overlying Peyer's patches in the terminal ileum (primary route)
- Via CFTR-mediated uptake by enterocytes (explains why CFTR mutations confer partial protection)
4. Peyer's Patches (Terminal Ileum)
- Bacteria enter the submucosa
- Taken up by mononuclear phagocytes/macrophages within Peyer's patches
- Bacteria survive and multiply intracellularly (resist killing inside phagosomes)
- Peyer's patches undergo hypertrophy then necrosis - the basis for ulceration and later perforation
5. Mesenteric Lymph Nodes
- Infected macrophages drain to mesenteric lymph nodes
- Further intracellular multiplication
6. Primary (Silent) Bacteremia - Incubation Phase (Days 1-14)
- Via the thoracic duct → bloodstream
- This is transient and silent - patient is asymptomatic or has mild prodrome
- Corresponds to the incubation period (mean 10-14 days, range 5-21 days)
7. Seeding of Reticuloendothelial System (RES)
- S. Typhi seeds the liver, spleen, bone marrow, and gallbladder
- Massive intracellular multiplication inside tissue macrophages
- Bone marrow is the most sensitive culture site even after antibiotics
8. Secondary (Sustained) Bacteremia - Symptomatic Phase (Week 1-2)
- Organisms released back into bloodstream in large numbers
- Cytokine storm: TNF-α, IL-1β, IL-6 released by activated macrophages
- Clinical features: stepwise rising fever (39-40.5°C), relative bradycardia (Faget's sign), headache, myalgia, malaise, anorexia
- Rose spots on abdomen/chest in ~30% of light-skinned patients (salmon-colored maculopapules - S. Typhi can be cultured from them)
- Hepatosplenomegaly in ~50%
9. Gallbladder Colonization → Intestinal Reseeding (Week 2-3)
- Gallbladder becomes infected (bile is an excellent culture medium)
- Organisms re-enter intestine via bile
- Re-infection of Peyer's patches → worsening diarrhea, GI symptoms more prominent in second week
- Stool cultures become positive at this stage
10. Complications (Week 2-4, untreated)
| Complication | Mechanism |
|---|---|
| Intestinal hemorrhage (~5%) | Necrosis of Peyer's patches erodes blood vessels |
| Ileal perforation (~1-3%) | Full-thickness necrosis at Peyer's patch sites |
| Hepatosplenomegaly | RES infiltration |
| Encephalopathy/delirium | Endotoxin + cytokine effect on CNS |
| Myocarditis | Endotoxin-mediated |
| DIC | Sustained bacteremia, endotoxin |
| Metastatic foci | Bone, joints, meninges, endocardium, liver abscess |
11. Chronic Carrier State
- 1-5% of patients become chronic carriers (>1 year shedding)
- Gallbladder is the reservoir (especially with cholelithiasis)
- Detected by anti-Vi antibody serology
- These carriers are the main human reservoir maintaining transmission
Diagnostic Correlation with Pathogenesis
| Week | Best Culture | Reason |
|---|---|---|
| Week 1 | Blood (sensitivity 70-90%) | Primary/secondary bacteremia |
| Week 2-3 | Bone marrow (80-95%), stool | RES seeding; biliary reseeding |
| Week 3 onward | Urine, stool | Urinary excretion begins |
| Any time | Bone marrow | Most sensitive, unaffected by antibiotics |