ABG analysis from basic to clinical.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have all the content needed for a comprehensive, well-organized response. Let me compile everything into a thorough ABG analysis guide.
Arterial Blood Gas (ABG) Analysis: Basic to Clinical
1. What Is an ABG?
An ABG is a blood sample drawn from an artery (typically the radial artery) that reports the partial pressures of oxygen and carbon dioxide, the direct serum pH, and a calculated bicarbonate. Modern analyzers also report lactate, total hemoglobin, and electrolytes.
"An arterial blood sample is the reference standard for pH, oxygen, carbon dioxide, and lactate content providing a description of the oxygen and carbon dioxide content of the blood after leaving the pulmonary circulation and before any gas exchange in the peripheral tissues has occurred."
- Tintinalli's Emergency Medicine
2. Normal Reference Values
| Parameter | Normal Value |
|---|---|
| pH | 7.35 - 7.45 |
| PaO₂ | 80 - 100 mmHg (room air) |
| PaCO₂ | 35 - 45 mmHg |
| HCO₃⁻ | 22 - 26 mEq/L |
| SaO₂ | ≥ 95% |
| Base excess (BE) | -2 to +2 mEq/L |
3. Basic Physiology: The Henderson-Hasselbalch Equation
The arterial pH is governed by the ratio of bicarbonate to dissolved CO₂:
pH = 6.1 + log₁₀ ( [HCO₃⁻] / [0.03 × PaCO₂] )
This reveals the two systems controlling pH:
- Respiratory system controls PaCO₂ (lungs)
- Renal system controls HCO₃⁻ (kidneys)
The fundamental equilibrium is:
CO₂ + H₂O ⇌ H₂CO₃ ⇌ HCO₃⁻ + H⁺
- Increased PaCO₂ → pushes reaction right → more H⁺ → pH falls (respiratory acidosis)
- Decreased PaCO₂ → pushes reaction left → less H⁺ → pH rises (respiratory alkalosis)
- Decreased HCO₃⁻ → more H⁺ generated → pH falls (metabolic acidosis)
- Increased HCO₃⁻ → H⁺ consumed → pH rises (metabolic alkalosis)
Medical Physiology (Boron): Protons are present in exceedingly low concentrations, yet have a major impact on biochemical reactions because pH-sensitive molecules include enzymes, receptors, ion channels, and structural proteins.
4. The 7-Step Systematic Approach
Use this stepwise approach every time - it prevents errors and catches mixed disorders.
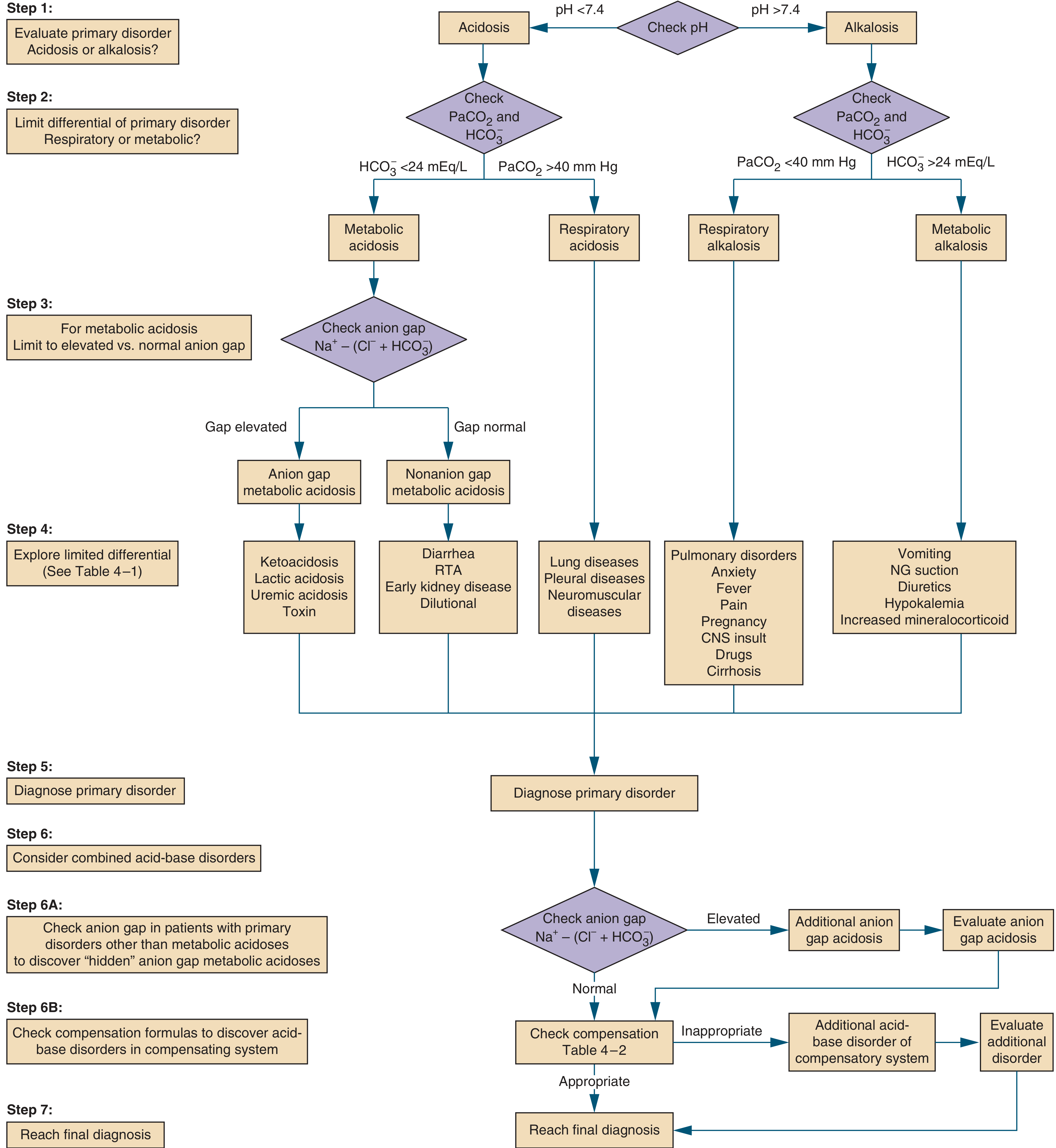
Step 1: Is it Acidosis or Alkalosis?
Check pH:
- pH < 7.35 = Acidemia (primary process is an acidosis)
- pH > 7.45 = Alkalemia (primary process is an alkalosis)
- pH 7.35-7.45 = Can still have a primary disorder with full compensation, or a mixed disorder
Step 2: Is It Respiratory or Metabolic?
Check PaCO₂ and HCO₃⁻:
| pH | PaCO₂ | HCO₃⁻ | Primary Disorder |
|---|---|---|---|
| Low | High (>40) | High (compensation) | Respiratory acidosis |
| Low | Low (compensation) | Low (<24) | Metabolic acidosis |
| High | Low (<40) | Low (compensation) | Respiratory alkalosis |
| High | High (compensation) | High (>24) | Metabolic alkalosis |
Key rule: Whatever matches the pH direction is the primary disorder.
Step 3: Anion Gap (for Metabolic Acidosis)
Anion Gap (AG) = Na⁺ - (Cl⁻ + HCO₃⁻)
Normal = 12 ± 4 mEq/L (some labs use 7-9 mEq/L depending on method)
"An elevated anion gap suggests one of those processes is the cause of the metabolic acidosis. Processes that lose HCO₃⁻ do not generate unmeasured anions and the anion gap remains normal." - Symptom to Diagnosis, 4th Ed.
Important: Always correct the AG for albumin:
- Corrected AG = Measured AG + 2.5 × (4.0 - measured albumin)
- For every 1 g/dL drop in albumin, the AG falls ~2.5 mEq/L
High Anion Gap Metabolic Acidosis (HAGMA) - Mnemonics:
MUDPILES or GOLD MARK:
- Methanol
- Uremia
- Diabetic ketoacidosis (DKA)
- Propylene glycol / Paracetamol
- Isoniazid / Iron
- Lactic acidosis
- Ethylene glycol
- Salicylates
Normal Anion Gap Metabolic Acidosis (NAGMA) - "HARD UP":
- Hyperchloremia
- Adrenal insufficiency
- Renal tubular acidosis (RTA)
- Diarrhea (bicarbonate loss from gut)
- Ureterodiversion
- Pancreatic fistula
Step 4: Check Compensation (Are the Compensatory Responses Appropriate?)
Compensation never fully normalizes pH (except chronic respiratory alkalosis). If compensation is inappropriate, a second primary disorder co-exists.
Compensation Formulas (from Harrison's Principles, 22nd Ed.):
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic acidosis | PaCO₂ = (1.5 × HCO₃⁻) + 8 ± 2 (Winter's equation) |
| Metabolic alkalosis | PaCO₂ increases 0.7 mmHg per 1 mEq/L rise in HCO₃⁻ (or: PaCO₂ = 40 + 0.7 × [HCO₃⁻ - 24] ± 5) |
| Acute respiratory acidosis | HCO₃⁻ rises 1 mEq/L per 10 mmHg rise in PaCO₂ |
| Chronic respiratory acidosis | HCO₃⁻ rises 3.5 mEq/L per 10 mmHg rise in PaCO₂ |
| Acute respiratory alkalosis | HCO₃⁻ falls 2 mEq/L per 10 mmHg fall in PaCO₂ |
| Chronic respiratory alkalosis | HCO₃⁻ falls 4-5 mEq/L per 10 mmHg fall in PaCO₂ |
Clinical Interpretation of Winter's formula:
- Measured PaCO₂ = predicted → appropriate compensation only; simple metabolic acidosis
- Measured PaCO₂ > predicted → concurrent respiratory acidosis
- Measured PaCO₂ < predicted → concurrent respiratory alkalosis
Step 5: Delta-Delta Ratio (Δ/Δ) - for High AG Metabolic Acidosis
This checks whether a concurrent metabolic alkalosis or non-AG metabolic acidosis is hiding behind the anion gap acidosis.
Δ/Δ = (Measured AG - 12) / (24 - Measured HCO₃⁻)
| Δ/Δ Ratio | Interpretation |
|---|---|
| < 1 | Concurrent non-AG metabolic acidosis (gap doesn't account for all the HCO₃⁻ fall) |
| 1 - 2 | Pure HAGMA |
| > 2 | Concurrent metabolic alkalosis or compensated chronic respiratory acidosis |
Step 6: Assess Oxygenation
A-a Gradient (Alveolar-Arterial Oxygen Gradient)
PAO₂ = [FiO₂ × (Patm - PH₂O)] - (PaCO₂ / 0.8)
At sea level on room air:
- Patm = 760 mmHg, PH₂O = 47 mmHg, FiO₂ = 0.21
- PAO₂ ≈ 150 - (PaCO₂ / 0.8)
P(A-a)O₂ = PAO₂ - PaO₂
Normal A-a gradient:
- Young adult: < 10-15 mmHg
- Age-adjusted: age/4 + 4 mmHg
Elevated A-a gradient suggests V/Q mismatch, shunt, or diffusion defect (NOT simple hypoventilation alone).
PaO₂/FiO₂ Ratio (P/F Ratio)
P/F = PaO₂ / FiO₂
| P/F Ratio | Clinical Significance |
|---|---|
| > 400 | Normal |
| 200-300 | Mild ARDS |
| 100-200 | Moderate ARDS |
| < 100 | Severe ARDS |
"A healthy person on 40% oxygen would be expected to have a ratio of approximately 600, representing a normal physiologic shunt of approximately 5%. As the shunt increases, the ratio decreases." - Tintinalli's Emergency Medicine
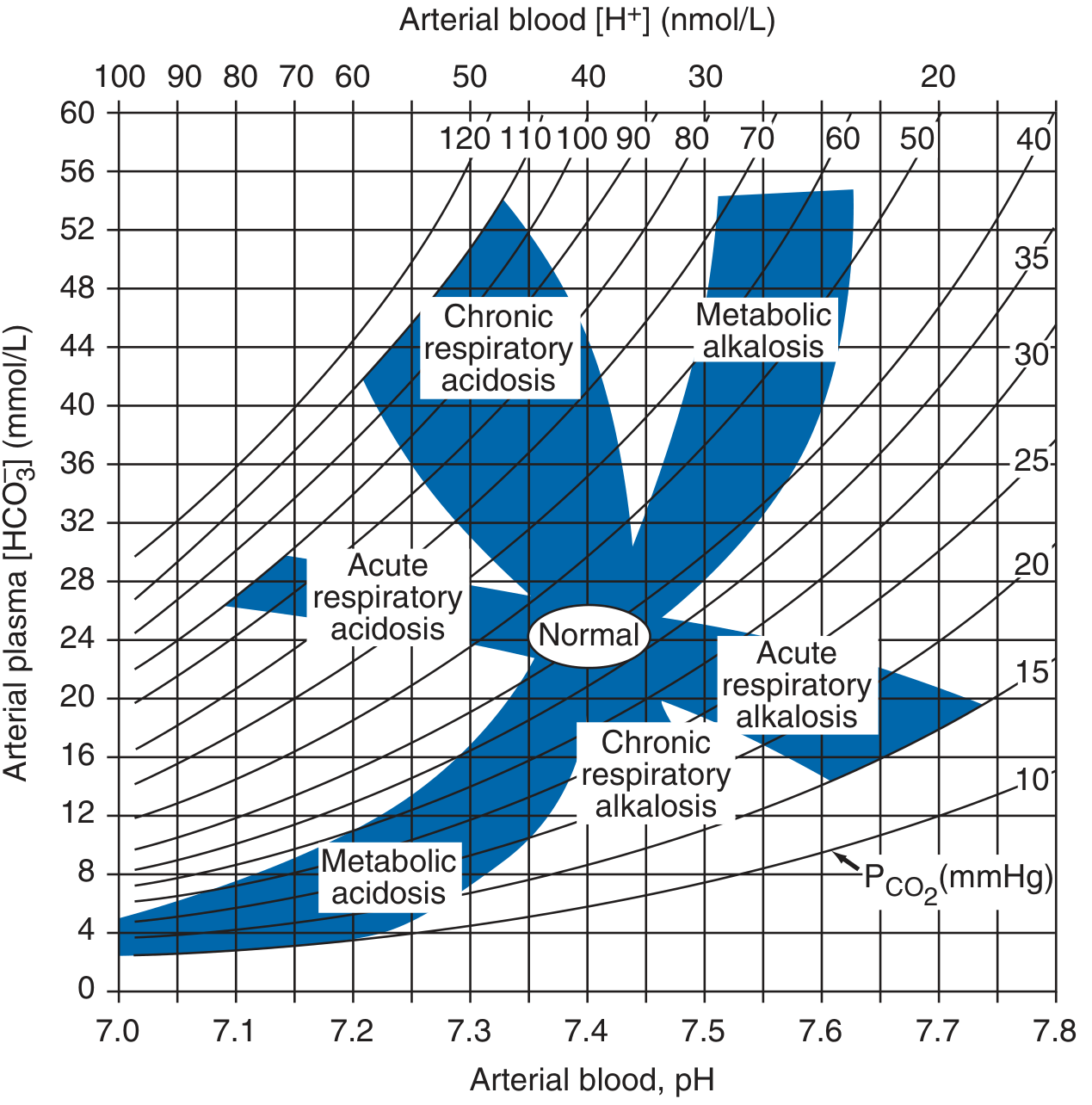
Step 7: Reach Final Diagnosis
Integrate all findings. Consider the clinical context. Now refer to the acid-base nomogram:
5. The Four Primary Disorders - Details
Metabolic Acidosis
Definition: Primary HCO₃⁻ fall (< 22 mEq/L), leading to low pH.
Causes:
- HAGMA: Lactic acidosis (sepsis, shock, ischemia), DKA, uremia, toxins
- NAGMA: Diarrhea, RTA types 1/2/4, saline infusion (dilutional), early CKD
Compensation: Kussmaul breathing (deep, rapid breathing = hyperventilation), driven by medullary chemoreceptors. Use Winter's formula to verify.
Urine Anion Gap (for NAGMA): = Na⁺ + K⁺ - Cl⁻ (urine)
- Negative (< 0): GI loss of HCO₃⁻ (diarrhea) - kidneys working normally
- Positive (> 0): Renal loss - suggests RTA or renal insufficiency
Metabolic Alkalosis
Definition: Primary HCO₃⁻ rise (> 26 mEq/L), leading to high pH.
Causes:
- Chloride-responsive (urine Cl⁻ < 25 mEq/L): Vomiting, NG suction, diuretics, post-hypercapnia
- Chloride-resistant (urine Cl⁻ > 25 mEq/L): Hyperaldosteronism, Cushing's, hypokalemia, increased mineralocorticoids, Bartter/Gitelman syndrome
Compensation: Hypoventilation (CO₂ retention). Expected PaCO₂ = 40 + 0.7 × (HCO₃⁻ - 24).
"Metabolic alkalosis is the most common acid-base disorder in hospitalized patients." - Harrison's Principles
Respiratory Acidosis
Definition: Primary PaCO₂ rise (> 45 mmHg) due to hypoventilation.
Causes:
- CNS depression (opioids, sedatives, stroke)
- Neuromuscular disorders (GBS, MG, ALS)
- Obstructive lung disease (COPD, severe asthma)
- Thoracic cage abnormalities
- Obesity hypoventilation
- Pneumothorax / pleural effusion
Compensation (renal):
- Acute: HCO₃⁻ ↑ 1 mEq/L per 10 mmHg ↑ PaCO₂
- Chronic: HCO₃⁻ ↑ 3.5 mEq/L per 10 mmHg ↑ PaCO₂ (takes 3-5 days)
"Respiratory acidosis incurs some beneficial effects: increased catecholamine release leading to increased cardiac output; it shifts the oxygen dissociation curve of hemoglobin to the right (Bohr effect), which increases oxygen unloading to the tissues." - Barash Clinical Anesthesia, 9th Ed.
Respiratory Alkalosis
Definition: Primary PaCO₂ fall (< 35 mmHg) due to hyperventilation.
Causes:
- Hypoxemia (high altitude, pulmonary embolism, pneumonia)
- Anxiety, pain, fever
- Pregnancy (progesterone stimulates respiration)
- Liver failure (cirrhosis)
- CNS insults (meningitis, stroke, tumor)
- Drugs (salicylates - early phase)
- Mechanical ventilation (iatrogenic)
Compensation (renal):
- Acute: HCO₃⁻ ↓ 2 mEq/L per 10 mmHg ↓ PaCO₂
- Chronic: HCO₃⁻ ↓ 4-5 mEq/L per 10 mmHg ↓ PaCO₂ (may normalize pH)
6. Mixed Acid-Base Disorders
Mixed disorders are two or more independent primary disorders occurring simultaneously (not just compensation). These are common in critically ill patients.
"The diagnosis of mixed acid-base disorders requires consideration of the anion gap... Changes in PaCO₂ and [HCO₃⁻] in opposite directions indicate a mixed acid-base disturbance." - Harrison's Principles, 22nd Ed.
Common clinically important mixed disorders:
| Mixed Disorder | Key Clue | Example |
|---|---|---|
| Metabolic acidosis + respiratory alkalosis | PaCO₂ below predicted (Winter's) | Sepsis, salicylate toxicity |
| Metabolic acidosis + respiratory acidosis | PaCO₂ above predicted | Cardiorespiratory arrest |
| Metabolic acidosis + metabolic alkalosis | Near-normal pH with AG; Δ/Δ > 2 | DKA with vomiting |
| Metabolic alkalosis + respiratory acidosis | PaCO₂ above predicted | COPD + diuretics |
| Metabolic alkalosis + respiratory alkalosis | Markedly high pH | Liver failure + NG suction |
7. Venous vs. Arterial Blood Gas
| Parameter | Arterial | Venous (peripheral) | Venous (central) |
|---|---|---|---|
| pH | Reference standard | ~0.05 lower | ~0.03 lower |
| PaCO₂ | Reference | Up to ±20 mmHg | ~5 mmHg higher |
| HCO₃⁻ | Reference | Close correlation | Close correlation |
| PaO₂ / O₂ saturation | Required for oxygenation | Cannot use | Cannot use |
"Normal venous carbon dioxide is predictive of normal PaCO₂; however, the clinical outcomes of substituting venous carbon dioxide for evaluation of hypercarbia have not been described." - Tintinalli's Emergency Medicine
Bottom line: VBG is acceptable for pH and CO₂ monitoring. ABG is mandatory for oxygenation assessment.
8. Worked Clinical Example (DKA)
Values: Na⁺ 138, K⁺ 6.2, HCO₃⁻ 6, Cl⁻ 100, glucose 389 mg/dL, pH 7.18, PaCO₂ 20 mmHg
| Step | Action | Result |
|---|---|---|
| 1. pH | 7.18 | Acidemia |
| 2. HCO₃⁻ vs PaCO₂ | HCO₃⁻ low (6) with acidemia | Metabolic acidosis (PaCO₂ low = compensation) |
| 3. Anion gap | 138 - (6+100) = 32 (normal ~12) | High AG metabolic acidosis |
| 4. Winter's formula | Expected PaCO₂ = 1.5×6 + 8 ± 2 = 17-19 mmHg | Measured PaCO₂ = 20; slightly above range = borderline; appropriate compensation |
| 5. Δ/Δ | (32-12) / (24-6) = 20/18 = 1.1 | Pure HAGMA |
| 6. Diagnosis | DKA (type 1 DM history, glucose 389, HAGMA, appropriate compensation) | High AG metabolic acidosis due to DKA |
9. Quick Reference Summary Table
| Disorder | pH | PaCO₂ | HCO₃⁻ |
|---|---|---|---|
| Metabolic acidosis | ↓ | ↓ (compensation) | ↓ (primary) |
| Metabolic alkalosis | ↑ | ↑ (compensation) | ↑ (primary) |
| Respiratory acidosis | ↓ | ↑ (primary) | ↑ (compensation) |
| Respiratory alkalosis | ↑ | ↓ (primary) | ↓ (compensation) |
Sources
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapter 58: Acidosis and Alkalosis
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - ABG Analysis, Alveolar Gas Exchange
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed. - Stepwise Acid-Base Approach
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Ed. - ABG Interpretation table, Delta-Delta
- Medical Physiology (Boron & Boulpaep) - Acid-Base Physiology chapter
- Comprehensive Clinical Nephrology, 7th Ed. - Mixed Acid-Base Disorders
This is a shared conversation. Sign in to Orris to start your own chat.