Sedative and hypnotic pharmacology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"sedative hypnotic" pharmacology
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I have rich content from multiple authoritative sources. Let me now compile a comprehensive, well-structured answer.
Sedative and Hypnotic Pharmacology
Overview and Historical Context
A sedative decreases activity, moderates excitement, and calms the patient, while a hypnotic produces drowsiness and facilitates onset and maintenance of sleep from which the patient can be aroused. Many drugs exhibit both properties in a dose-dependent fashion.
Historically, bromides (1850s), chloral hydrate, and paraldehyde preceded barbiturates (barbital 1903, phenobarbital 1912). The synthesis of chlordiazepoxide and its clinical introduction in 1961 ushered in the era of benzodiazepines, which largely replaced barbiturates due to their far superior safety profile. "Z-drugs" (zolpidem, zaleplon, eszopiclone) then followed as even more selective agents.
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 447
- Lippincott Illustrated Reviews: Pharmacology, p. 546
Drug Classes
| Class | Key Agents | Primary Mechanism |
|---|---|---|
| Benzodiazepines | Diazepam, lorazepam, midazolam, alprazolam, clonazepam | GABA-A positive allosteric modulator (increases Cl⁻ channel opening frequency) |
| Z-drugs (Non-BZD BZR agonists) | Zolpidem, zaleplon, eszopiclone | GABA-A positive allosteric modulator (BZ site, alpha-1 selective) |
| Barbiturates | Phenobarbital, thiopental, pentobarbital | GABA-A (increases Cl⁻ channel duration) + NMDA block |
| Melatonin receptor agonists | Ramelteon, tasimelteon | MT1/MT2 agonism (circadian regulation) |
| Orexin receptor antagonists | Suvorexant, lemborexant | Dual orexin receptor antagonism (wake-drive inhibition) |
| Miscellaneous | Chloral hydrate, meprobamate | Barbiturate-like (low therapeutic index) |
| Antihistamines | Diphenhydramine, doxylamine | H1 antagonism |
| Tricyclic antidepressant | Doxepin (low dose) | H1 antagonism |
1. Benzodiazepines
Mechanism of Action
Benzodiazepines act on GABA-A receptors, which are pentameric ligand-gated chloride channels composed of α, β, and γ subunits. GABA binding opens the chloride channel, causing hyperpolarization and inhibiting action potential formation.
Benzodiazepines bind to a specific high-affinity allosteric site at the interface of the α and γ subunits (distinct from the GABA binding site). This binding:
- Increases the frequency of chloride channel openings (not duration - that is barbiturates)
- Requires GABA to be present (positive allosteric modulation, not direct agonism)
- Clinical effects correlate well with binding affinity for the GABA-A receptor
The α1 subunit mediates sedation, amnesia, and anticonvulsant effects; the α2/α3 subunits mediate anxiolytic and muscle-relaxant effects. The γ subunit is required for benzodiazepine binding.
Lippincott Illustrated Reviews: Pharmacology, pp. 547-548
Pharmacokinetics and Classification
Benzodiazepines are classified by duration of action:
| Duration | Drug | t½ | Active Metabolites | Notes |
|---|---|---|---|---|
| Ultra-short | Triazolam | 2-4 h | None | Rebound insomnia common |
| Short | Oxazepam, lorazepam, temazepam | 10-20 h | None | Preferred in elderly/liver disease |
| Intermediate | Alprazolam, clonazepam | 12-24 h | Minimal | |
| Long | Diazepam, chlordiazepoxide, flurazepam | 24-100+ h | Yes (active) | Accumulation risk |
Lorazepam, oxazepam, and temazepam ("LOT") undergo only Phase II glucuronidation - safe in hepatic impairment and elderly.
Most benzodiazepines are highly lipid-soluble, well absorbed orally, and highly protein-bound. They are CYP3A4 substrates.
Clinical Uses
- Anxiety disorders (GAD, panic, social phobia) - though SSRIs/SNRIs now preferred first-line
- Insomnia (short-term)
- Seizure disorders - diazepam, lorazepam (status epilepticus); clonazepam (myoclonic seizures)
- Alcohol withdrawal - chlordiazepoxide, diazepam, lorazepam
- Procedural sedation / premedication - midazolam (rapid onset, short duration)
- Muscle spasm - diazepam
- Spasticity - clonazepam
Adverse Effects
- Sedation, psychomotor impairment, anterograde amnesia
- Respiratory depression (potentiated by opioids, alcohol - major risk)
- Tolerance and physical dependence (with chronic use)
- Rebound anxiety/insomnia on discontinuation
- Falls and cognitive impairment in elderly (use with caution)
Safety Profile
The benzodiazepine therapeutic index is remarkable - the lethal dose is over 1,000-fold greater than the typical therapeutic dose:
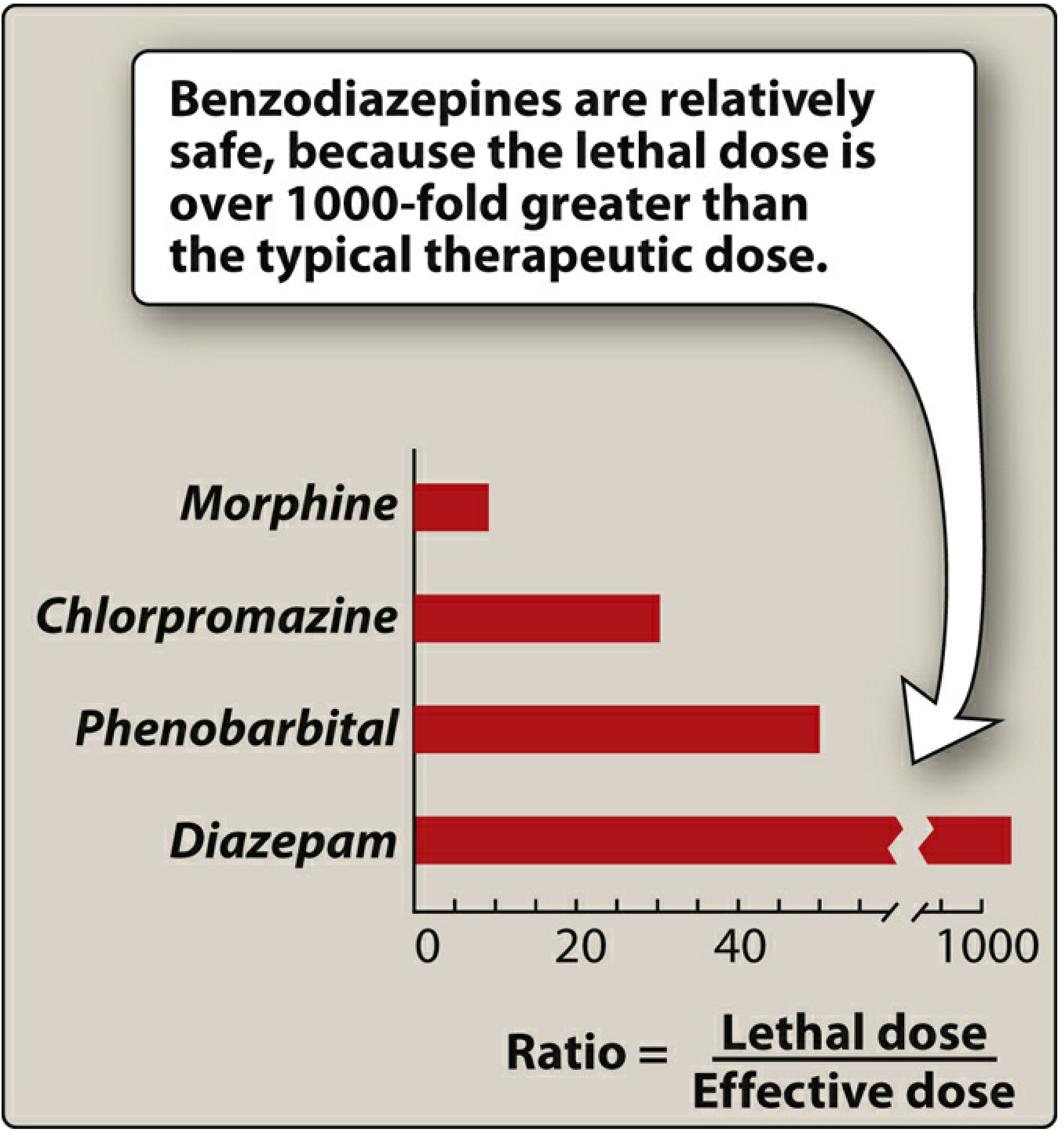
Lippincott Illustrated Reviews: Pharmacology, p. 547
Tolerance and Dependence
Tolerance involves:
- Downregulation and desensitization of GABA-A receptors
- Structural receptor changes and uncoupling from the drug
- Cross-tolerance with barbiturates and other GABA-A modulators
Withdrawal syndrome: Anxiety, agitation, insomnia, tachycardia, palpitations, and - in severe cases - seizures. Taper is essential; abrupt cessation can be life-threatening.
Flumazenil (Reversal Agent)
A competitive benzodiazepine receptor antagonist used IV for benzodiazepine overdose. Caution: can precipitate seizures in chronic BZ users or in those who have co-ingested proconvulsant drugs (e.g., tricyclic antidepressants). Short half-life (~1 h) requires monitoring for re-sedation.
2. Z-Drugs (Non-Benzodiazepine BZ-Receptor Agonists)
Zolpidem (imidazopyridine), zaleplon (pyrazolopyrimidine), and eszopiclone (cyclopyrrolone) are structurally distinct from benzodiazepines but bind to the same benzodiazepine site on GABA-A receptors. Key distinction:
- Benzodiazepines activate all three GABA-BZ binding sites on the receptor
- Z-drugs are alpha-1 subunit selective - this confers sedation/hypnosis with less anxiolysis, muscle relaxation, and anticonvulsant effect
Key pharmacokinetic advantage: Rapid metabolism, no active metabolites - avoids the accumulation seen with long-acting benzodiazepines.
| Drug | t½ | Notes |
|---|---|---|
| Zaleplon | ~1 h | Shortest - useful for middle-of-night awakening |
| Zolpidem | 1.5-2.5 h | Extended-release formulation available |
| Eszopiclone | 5-7 h | Longest among Z-drugs; approved for longer-term use |
Unlike benzodiazepines, at usual hypnotic doses, Z-drugs do not significantly alter sleep stage architecture (i.e., do not suppress REM or slow-wave sleep as much) - hence often preferred as hypnotics.
Adverse effects: CNS depression, complex sleep behaviors (sleepwalking, sleep-driving), hallucinations (especially zolpidem). All are Schedule IV controlled substances with dependence potential. Flumazenil can reverse their effects.
Lippincott Illustrated Reviews: Pharmacology, p. 560; Kaplan & Sadock's Synopsis, p. 1876
3. Barbiturates
Mechanism
Barbiturates are positive allosteric modulators of GABA-A receptors but with a distinct binding site from benzodiazepines:
- Increase the duration of Cl⁻ channel opening (not frequency)
- At high (anesthetic) concentrations: directly activate the Cl⁻ channel (GABA-independent)
- Also block NMDA and AMPA/kainate receptors (glutamate antagonism)
- Inhibit voltage-dependent Na⁺ channels at anesthetic concentrations
- Block excitatory nicotinic receptor channels
Most barbiturate sedative-hypnotics bind to the alpha-1 subunit of GABA-A; etomidate and propofol act at different subunits (beta-2/beta-3).
Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 9773
Classification
| Category | Drug | t½ | Use |
|---|---|---|---|
| Ultra-short | Thiopental, methohexital | Minutes | IV anesthesia induction |
| Short-intermediate | Pentobarbital, secobarbital | 18-48 h | Sedation, ICU |
| Long | Phenobarbital | 80-120 h | Epilepsy, neonatal seizures |
Pharmacokinetics
- Highly lipid-soluble (thiopental - rapid CNS entry and redistribution explains its ultra-short action)
- Strong inducers of hepatic CYP enzymes (multiple drug interactions)
- Cause porphyria exacerbation (induce ALA synthase)
Untoward Effects and Toxicity
- Narrow therapeutic index - fatal CNS and respiratory depression possible
- Respiratory depression, hypotension in overdose
- No specific antidote - treatment is supportive (airway, ventilation, vasopressors)
- Physical dependence; severe, potentially life-threatening withdrawal (seizures)
- Tolerance develops rapidly
Barbiturate Poisoning
Supportive care is the cornerstone: airway protection (intubation), mechanical ventilation, IV fluids for hypotension. Alkalinization of urine (sodium bicarbonate) enhances renal excretion of phenobarbital (which is a weak acid).
4. Melatonin Receptor Agonists
Ramelteon and tasimelteon act as MT1/MT2 agonists:
- Regulate circadian rhythm and promote sleep onset
- No abuse potential, not scheduled
- No GABA-A activity - do not cause dependence or withdrawal
- Ramelteon: approved for sleep-onset insomnia
- Tasimelteon: approved for non-24-hour sleep-wake disorder (particularly in blind individuals)
5. Orexin Receptor Antagonists
Suvorexant and lemborexant are dual orexin receptor antagonists (DORA):
- Block orexin (hypocretin) OX1 and OX2 receptors
- Orexin normally promotes wakefulness; blocking it reduces wake drive
- Approved for sleep-onset and sleep-maintenance insomnia
- Lower dependence potential than BZDs; Schedule IV
- Adverse effect: cataplexy-like symptoms, complex sleep behaviors, next-day somnolence
6. Miscellaneous Agents
Chloral hydrate:
- Rapidly reduced to active metabolite trichloroethanol (by hepatic alcohol dehydrogenase)
- Barbiturate-like GABA-A effects
- Low therapeutic index; "knockout drops" of literary fame
- Schedule IV; used for paradoxical reactions to benzodiazepines
Meprobamate:
- Bis-carbamate ester; Schedule IV
- Benzodiazepine-like actions but cannot produce anesthesia
- Severe overdose causes respiratory depression, cardiovascular collapse
- Risk of gastric bezoar formation in overdose
- Withdrawn from EU and Canada due to side-effect profile
Buspirone (anxiolytic, not hypnotic):
- 5-HT1A partial agonist (also D2 and 5-HT2A affinity)
- Slow onset (2-4 weeks); effective for chronic GAD only - not for acute/PRN use
- No anticonvulsant or muscle-relaxant effects; no dependence potential
- Does not potentiate CNS depression of alcohol
Comparative Summary: GABA-A Pharmacology
| Drug Class | Binding Site | Effect on Cl⁻ Channel | GABA Required? |
|---|---|---|---|
| Benzodiazepines | α/γ interface | Increases frequency of opening | Yes |
| Z-drugs | α1/γ interface | Increases frequency of opening | Yes |
| Barbiturates | β subunit | Increases duration of opening; direct activation at high dose | No (at high doses) |
| Etomidate | β2/β3 subunit | GABA mimicry | Partially |
Overdose Management Summary
| Drug | Antidote | Notes |
|---|---|---|
| Benzodiazepines | Flumazenil IV | Risk of seizures in dependent patients |
| Z-drugs | Flumazenil | Also reverses effects |
| Barbiturates | None | Supportive care only; urine alkalinization for phenobarbital |
| Ethanol/GHB | None | Supportive; GHB coma resolves rapidly (3-4 h) |
Recent Evidence (2024-2026)
Recent systematic reviews have highlighted:
-
Sedative-hypnotics and Alzheimer's risk: A 2026 meta-analysis (PMID 42334823) found an association between long-term sedative-hypnotic use and increased Alzheimer's disease risk - reinforcing guidance to use the lowest effective dose for the shortest duration.
-
ICU intubation: A 2026 systematic review (PMID 40368347) examined outcomes of sedative-hypnotic agents used for endotracheal intubation in critically ill adults - ketamine and etomidate remain common, with ongoing debate about hemodynamic profiles.
-
Eszopiclone for comorbid insomnia: A 2026 systematic review (PMID 41840848) supports eszopiclone's use in insomnia comorbid with psychiatric disorders.
Key Teaching Points:
- Benzodiazepines increase frequency of Cl⁻ channel opening; barbiturates increase duration
- Z-drugs are alpha-1 selective - hypnosis without significant anxiolysis/muscle relaxation/anticonvulsion
- Only benzodiazepines and Z-drugs have a reversal agent (flumazenil)
- "LOT" benzodiazepines (lorazepam, oxazepam, temazepam) are safe in liver disease/elderly
- Barbiturate withdrawal is life-threatening; benzodiazepine withdrawal can also cause seizures
- Ramelteon and buspirone have no abuse potential and do not cause dependence
This is a shared conversation. Sign in to Orris to start your own chat.