ABG all concepts and clinical application
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have rich content from multiple authoritative textbooks. Let me compile the comprehensive ABG guide.
Arterial Blood Gas (ABG): All Concepts and Clinical Application
Sources: Roberts & Hedges' Clinical Procedures in Emergency Medicine; Symptom to Diagnosis (4th Ed.); Goldman-Cecil Medicine; Tintinalli's Emergency Medicine; Barash Clinical Anesthesia; Fishman's Pulmonary Diseases
1. What is an ABG?
An ABG is a sample of arterial blood that simultaneously reports:
- pH - overall acid-base status
- PaCO2 - adequacy of ventilation
- PaO2 - oxygenation
- HCO3- - calculated bicarbonate (Henderson-Hasselbalch)
- Base excess/deficit - overall metabolic deviation from normal
- Often also includes: lactate, SpO2, hemoglobin, electrolytes
Arterial blood provides data after pulmonary gas exchange but before peripheral tissue uptake - the gold standard for ventilation and oxygenation assessment.
"An arterial blood sample is the reference standard for pH, oxygen, carbon dioxide, and lactate content, providing a description of the oxygen and carbon dioxide content of the blood after leaving the pulmonary circulation." - Tintinalli's Emergency Medicine
2. Normal ABG Values
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaCO2 | 35 - 45 mm Hg |
| PaO2 | 70 - 95 mm Hg (age-dependent) |
| HCO3- | 22 - 26 mEq/L |
| SaO2 | 95 - 100% |
| Base excess | -2 to +2 mEq/L |
Age-adjusted PaO2 (sitting): PaO2 = 104.2 - (0.27 x age in years)
3. The Henderson-Hasselbalch Relationship
The key equation underlying ABG interpretation:
CO2 + H2O ⇌ H2CO3 ⇌ HCO3- + H+
- ↑ PaCO2 → reaction shifts right → ↑ H+ → ↓ pH = Respiratory Acidosis
- ↓ PaCO2 → reaction shifts left → ↓ H+ → ↑ pH = Respiratory Alkalosis
- ↑ HCO3- → reaction shifts left → ↓ H+ → ↑ pH = Metabolic Alkalosis
- ↓ HCO3- → reaction shifts right → ↑ H+ → ↓ pH = Metabolic Acidosis
4. Step-by-Step ABG Interpretation
Step 1: Is the patient acidemic or alkalemic?
- pH < 7.35 = Acidemia
- pH > 7.45 = Alkalemia
- pH 7.35-7.45 = Normal (but a disorder may still exist - "compensated")
Step 2: Identify the primary disorder
| Condition | pH | Primary Change |
|---|---|---|
| Respiratory acidosis | < 7.35 | PaCO2 > 45 mm Hg |
| Respiratory alkalosis | > 7.45 | PaCO2 < 35 mm Hg |
| Metabolic acidosis | < 7.35 | HCO3- < 22 mEq/L |
| Metabolic alkalosis | > 7.45 | HCO3- > 26 mEq/L |
Rule: The parameter that "matches" the pH direction is the primary disorder. If both PaCO2 and HCO3- are abnormal, whichever explains the pH change is primary.
Step 3: Check for compensation
Compensation is always in the same direction as the primary change (partial correction), but never overcorrects.
| Primary Disorder | Compensatory Response | Formula |
|---|---|---|
| Metabolic acidosis | ↓ PaCO2 (hyperventilation) | Expected PaCO2 = 1.5 × [HCO3-] + 8 ± 2 (Winter's formula) OR ΔPaCO2 = 1.3 × ΔHCO3- |
| Metabolic alkalosis | ↑ PaCO2 (hypoventilation) | ΔPaCO2 = 0.6 × ΔHCO3- |
| Respiratory acidosis (acute) | ↑ HCO3- by 1 mEq/L per 10 mm Hg ↑ PaCO2 | |
| Respiratory acidosis (chronic) | ↑ HCO3- by 4 mEq/L per 10 mm Hg ↑ PaCO2 | |
| Respiratory alkalosis (acute) | ↓ HCO3- by 2 mEq/L per 10 mm Hg ↓ PaCO2 | |
| Respiratory alkalosis (chronic) | ↓ HCO3- by 5 mEq/L per 10 mm Hg ↓ PaCO2 |
If the actual compensation does NOT match the predicted, a mixed disorder is present.
Step 4: Calculate the Anion Gap (if metabolic acidosis)
AG = Na+ - (HCO3- + Cl-)
- Normal = 12 ± 4 mEq/L (some labs use 7-9)
- High AG = unmeasured anions present (acid production)
- Normal AG = bicarbonate loss
Albumin correction: Normal AG is 2.5 mEq/L lower for every 1 g/dL drop in albumin below 4.4 g/dL.
5. The Acid-Base Map
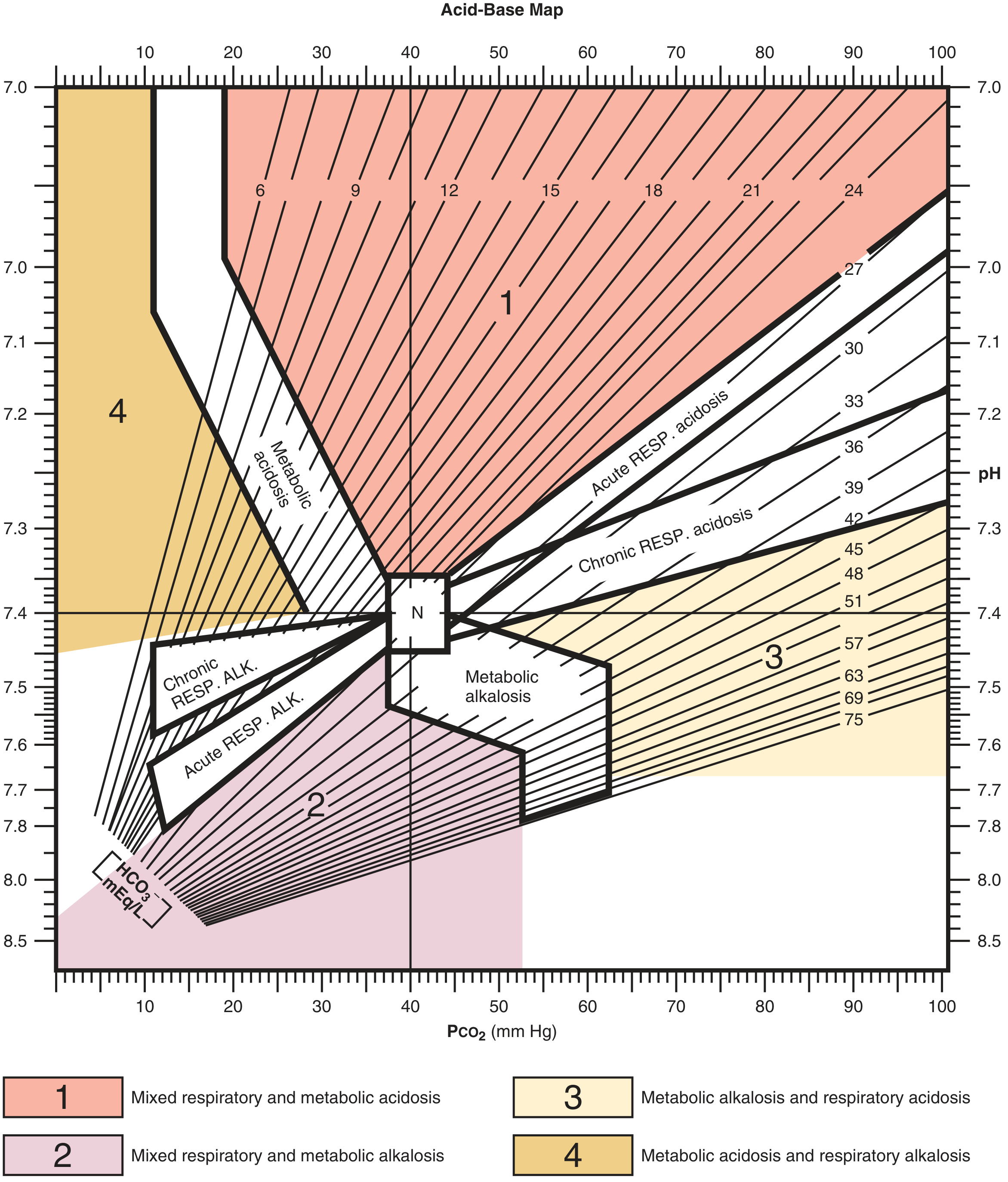
Acid-Base Map (Roberts & Hedges'). N = normal. Zones 1-4 represent mixed disorders. Each numbered zone and labeled band indicates expected compensation ranges.
Plotting a patient's pH and PaCO2 on this map:
- Falls within a labeled band = simple (single) disorder
- Falls outside any band / in a numbered zone = mixed disorder
6. Differential Diagnosis by Category
Metabolic Acidosis - Anion Gap (MUDPILES / KULT)
| Mnemonic | Causes |
|---|---|
| Ketoacidosis | DKA, alcoholic, starvation |
| Uremia | Chronic kidney disease |
| Lactic acidosis | Shock (septic, cardiogenic, hypovolemic), hypoxia, CO poisoning, seizures, metformin |
| Toxins | Methanol, ethylene glycol, salicylates, D-lactic acidosis, rhabdomyolysis |
Metabolic Acidosis - Normal Anion Gap (HARD-UP / DRIED)
| Cause |
|---|
| Diarrhea (most common) |
| Renal tubular acidosis (RTA) |
| Iatrogenic (saline, carbonic anhydrase inhibitors - acetazolamide) |
| Early kidney disease |
| Dilutional acidosis |
Metabolic Alkalosis
- Vomiting / nasogastric suction (H+ loss)
- Diuretics (volume contraction, Cl- loss)
- Hypokalemia
- Primary hyperaldosteronism (Conn's syndrome)
- Cushing syndrome / exogenous steroids
- Excessive licorice ingestion (mineralocorticoid-like effect)
Respiratory Acidosis (Hypoventilation)
| Category | Examples |
|---|---|
| Pulmonary | COPD, asthma, pneumonia, pulmonary edema, pleural effusion, pneumothorax |
| CNS | Stroke, opioids/sedatives, sleep apnea |
| Spinal cord | Trauma, ALS, polio |
| Nerve | Guillain-Barre syndrome |
| NMJ | Myasthenia gravis |
| Chest wall | Flail chest, muscular dystrophy |
Respiratory Alkalosis (Hyperventilation)
| Category | Examples |
|---|---|
| Pulmonary | PE, pneumonia, asthma, ILD, mechanical ventilation |
| CNS | Anxiety, pain, fever, CNS lesion |
| Systemic | Pregnancy, cirrhosis, sepsis (early), high altitude |
| Drugs | Salicylates (early), progesterone |
7. Assessing Oxygenation from the ABG
Alveolar-Arterial (A-a) Gradient
P(A-a)O2 = [FiO2 × (Patm - PH2O) - (PaCO2/0.8)] - PaO2
At room air (FiO2=0.21), sea level (Patm=760), body temp (PH2O=47 mm Hg):
PAO2 = 0.21 × (760-47) - (PaCO2/0.8) = 149.7 - (PaCO2 × 1.25)
Normal A-a gradient: < 15 mm Hg in young adults; age/4 + 4 for age-adjusted estimate
| A-a Gradient | Interpretation |
|---|---|
| Normal | Hypoventilation only (e.g., opioids, CNS cause) |
| Elevated | V/Q mismatch, shunt, diffusion impairment |
P/F Ratio (PaO2/FiO2)
- Normal: ~500 mm Hg (on room air PaO2 ~100 / FiO2 0.21)
- Mild ARDS: 200-300 mm Hg
- Moderate ARDS: 100-200 mm Hg
- Severe ARDS: < 100 mm Hg
"The PaO2/FiO2 ratio is the most frequently used parameter for evaluating the severity of lung failure and is included in the current definition for acute lung injury/ARDS." - Tintinalli's Emergency Medicine
8. Mixed Acid-Base Disorders
A mixed disorder is present when the compensation does NOT match predictions, or when values fall outside the expected compensation bands.
Delta-Delta Gap (ΔAG / ΔHCO3-)
Used when an anion gap metabolic acidosis is confirmed - to detect a concomitant second disorder.
Formula:
ΔAG = Measured AG - Normal AG (12) ΔHCO3- = Normal HCO3- (24) - Measured HCO3- Delta/Delta ratio = ΔAG / ΔHCO3-
| Delta/Delta Ratio | Interpretation |
|---|---|
| ~1:1 (0.8-2.0) | Pure anion gap metabolic acidosis |
| < 1 (< 0.8) | AGMA + concomitant non-anion gap acidosis (HCO3- falls more than expected) |
| > 2 (> 2.0) | AGMA + concomitant metabolic alkalosis (HCO3- falls less than expected due to alkalosis offsetting) |
Note: In lactic acidosis ΔAG/ΔHCO3- is typically 1.6:1; in ketoacidosis ~1:1 due to ketonuria.
Common Mixed Patterns
| Pattern | Example |
|---|---|
| Metabolic acidosis + Respiratory alkalosis | Sepsis, salicylate toxicity |
| Metabolic alkalosis + Respiratory acidosis | COPD with chronic diuretic use |
| Mixed metabolic acidosis + metabolic alkalosis | Alcoholic with vomiting and diarrhea |
| Triple disorder | DKA + vomiting + respiratory failure |
9. Venous Blood Gas (VBG) vs. ABG
| Parameter | VBG vs. ABG |
|---|---|
| pH | VBG ≈ ABG (differ by ± 0.05) - clinically interchangeable for monitoring |
| PaCO2 | VBG is 3-8 mm Hg higher; correlates but varies (up to ±20 mm Hg) |
| PaO2 | VBG does NOT correlate with arterial O2 - cannot assess oxygenation |
| Lactate | Venous correlates well with arterial at normal/markedly abnormal values; mildly elevated venous should be confirmed arterially |
"Normal venous CO2 is predictive of normal PaCO2; however, venous PaCO2 values do not correlate with arterial oxygen content and cannot be used for evaluation of oxygenation." - Tintinalli's Emergency Medicine
10. Clinical Examples (Worked Cases)
Case 1: Diarrhea (Non-Anion Gap Metabolic Acidosis)
ABG: pH 7.26, PaCO2 13, HCO3- 5
- Acidemia → metabolic (HCO3- low)
- Winter's formula: Expected PaCO2 = 1.5×5 + 8 = 15.5 ± 2 → actual 13 ≈ predicted → pure metabolic acidosis, adequate compensation
- AG = Na 133 - (118 + 5) = 10 → normal AG → non-anion gap metabolic acidosis
- Diagnosis: Diarrhea-induced bicarbonate loss
Case 2: Sepsis (Anion Gap Metabolic Acidosis)
ABG: pH 7.28, PaCO2 30, HCO3- 14; Na 138, Cl 102
- Acidemia → metabolic (HCO3- low, PaCO2 low = compensation)
- AG = 138 - (102+14) = 22 → elevated AG metabolic acidosis
- Predicted PaCO2 = 1.5×14 + 8 = 29 ± 2 → actual 30 ≈ adequate compensation
- Diagnosis: Lactic acidosis from sepsis
Case 3: COPD Exacerbation (Respiratory Acidosis)
ABG: pH 7.28, PaCO2 70, HCO3- 27; Na 138, Cl 102
- Acidemia → PaCO2 elevated = respiratory acidosis
- Compensation check: chronic respiratory acidosis → expected HCO3- rise = 4×(70-40)/10 = 12 → expected HCO3- = 24+12 = 36 mEq/L; actual 27
- HCO3- only 27 suggests acute-on-chronic respiratory acidosis (or inadequate renal compensation), suggesting an acute component
- AG = 138 - (27+102) = 9 → normal (no metabolic acidosis)
- Diagnosis: Acute-on-chronic respiratory acidosis (COPD exacerbation)
Case 4: DKA with Vomiting (Mixed Disorder)
ABG: pH 7.10, PaCO2 20, HCO3- 12; Na 138, Cl 100; AG = 138-(12+100) = 26
- ΔAG = 26-12 = 14; ΔHCO3- = 24-12 = 12
- Δ/Δ = 14/12 = 1.17 → pure AGMA
- But if vomiting coexists: expected HCO3- should be lower based on pure AGMA - if actual HCO3- is higher than predicted → concomitant metabolic alkalosis
- Diagnosis: Guide therapy accordingly
11. Urine Anion Gap (UAG) - Extension of ABG Interpretation
When non-AG metabolic acidosis is present, UAG distinguishes renal vs. GI cause:
UAG = Urine (Na+ + K+) - Urine Cl-
| UAG | Interpretation |
|---|---|
| Negative (< 0) | GI bicarbonate loss (diarrhea) - kidneys excreting NH4+ appropriately |
| Positive (> 0) | Renal tubular acidosis - kidneys NOT excreting NH4+ |
12. Quick Clinical Algorithm Summary
Step 1: Check pH
↓ pH (<7.35) = Acidemia | ↑ pH (>7.45) = Alkalemia
Step 2: Identify primary disorder
Acidemia: ↑ PaCO2 = Resp Acidosis | ↓ HCO3- = Met Acidosis
Alkalemia: ↓ PaCO2 = Resp Alkalosis | ↑ HCO3- = Met Alkalosis
Step 3: Check compensation (expected vs. actual)
Match = Simple disorder
Mismatch = Mixed disorder
Step 4 (if Met Acidosis): Calculate AG
High AG → MUDPILES
Normal AG → HARDUPS (diarrhea, RTA, etc.)
Step 5 (if High AG): Calculate Delta-Delta
<0.8 = AG + Non-AG acidosis
0.8-2 = Pure AG acidosis
>2 = AG acidosis + metabolic alkalosis
Step 6: Assess Oxygenation
A-a gradient (normal vs. elevated)
P/F ratio (ARDS severity)
13. Key Pearls
-
Compensation is never complete - if pH normalizes, a mixed disorder is present
-
Chronic vs. acute respiratory disorders differ in degree of HCO3- compensation (1 vs. 4 mEq/L per 10 mm Hg PaCO2 for acidosis)
-
Hypoalbuminemia lowers the normal AG - must correct before concluding AG is normal
-
Salicylate toxicity classically causes a mixed picture: respiratory alkalosis (direct brainstem stimulation) + anion gap metabolic acidosis (uncouples oxidative phosphorylation)
-
Normal PaO2 does NOT rule out respiratory failure if the patient is on supplemental oxygen
-
VBG can safely replace ABG for pH monitoring but NOT for oxygenation assessment
-
A PaO2 target of 60 mm Hg is as good as 90 mm Hg in ICU patients with acute hypoxemic respiratory failure requiring high-flow oxygen
-
Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 1734
-
Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed., pp. 69-72
-
Goldman-Cecil Medicine, p. 258
-
Tintinalli's Emergency Medicine, pp. 121-122
-
Barash Clinical Anesthesia, 9th Ed., pp. 1162-1163
This is a shared conversation. Sign in to Orris to start your own chat.